
Heart and Circulation
Heart and Circulation
You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Josephson - Clinical Cardiac Electrophysiology Techniques AnDocument451 pagesJosephson - Clinical Cardiac Electrophysiology Techniques Anmobilica100% (5)
- Congestive Heart FailureDocument8 pagesCongestive Heart Failureiancel_038893% (27)
- Case Study Congestive Heart Failure Patho)Document8 pagesCase Study Congestive Heart Failure Patho)Mj Silva100% (3)
- A1 CardioDocument98 pagesA1 CardioTikboy TaliliNo ratings yet
- Chapter 41. Nursing Care of The Child With A Cardiovascular Disorder TermDocument11 pagesChapter 41. Nursing Care of The Child With A Cardiovascular Disorder TermJœnríčk AzueloNo ratings yet
- Lecture On Human Circulatory SystemDocument7 pagesLecture On Human Circulatory SystemolandiolettyNo ratings yet
- 3 Review CvsDocument108 pages3 Review CvsSaif AlzateemhNo ratings yet
- 1cardiovascular System DisordersDocument13 pages1cardiovascular System DisordersArvin MalondrasNo ratings yet
- Assessment of The Cardiovascular SystemDocument48 pagesAssessment of The Cardiovascular Systemkimberlyrwarren8817No ratings yet
- PerfusionDocument9 pagesPerfusionAmanda Brittain100% (2)
- HypertensionDocument11 pagesHypertensionJyoti singhNo ratings yet
- 18 Heartpart1 Basiccongestiveheartfailure 110919083613 Phpapp01Document43 pages18 Heartpart1 Basiccongestiveheartfailure 110919083613 Phpapp01Atikah PurnamasariNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- Medical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Cardiovascular SystemDocument43 pagesMedical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Cardiovascular Systemsarah morleyNo ratings yet
- The Circulatory SystemDocument25 pagesThe Circulatory SystemEduardson PHNo ratings yet
- Heart Failure: Presented By: Leslie PaguioDocument38 pagesHeart Failure: Presented By: Leslie PaguioLeslie PaguioNo ratings yet
- Med Surg 2Document76 pagesMed Surg 2sham gowliNo ratings yet
- Cardiovascular and Heart DiseaseDocument65 pagesCardiovascular and Heart DiseasesarazalnoonNo ratings yet
- Lesson9 Cardiovascular AssessmentDocument21 pagesLesson9 Cardiovascular AssessmentDennis Nabor Muñoz, RN,RMNo ratings yet
- Cardiology - Dr. Allam 2021Document141 pagesCardiology - Dr. Allam 2021MohammedNo ratings yet
- 3 Heart FailureDocument8 pages3 Heart FailureAudrey Ann AcobNo ratings yet
- Cardiovascular System: Presented byDocument76 pagesCardiovascular System: Presented bySoma Al-mutairiNo ratings yet
- AP Refresher 1 Heart PhysiologyDocument52 pagesAP Refresher 1 Heart Physiologymaxwell amponsahNo ratings yet
- Cardivascular SystemDocument11 pagesCardivascular SystemAnneMarielleManaloNo ratings yet
- Lec 3 - Circulatory SystemDocument9 pagesLec 3 - Circulatory SystemJewel Jehd AlegriaNo ratings yet
- CVS 3-3 PDFDocument24 pagesCVS 3-3 PDFafaq alismailiNo ratings yet
- Cardiovascular SystemDocument11 pagesCardiovascular SystemРахым ХасеновNo ratings yet
- Nursing Management of Patient With CCFDocument34 pagesNursing Management of Patient With CCFJayarani Ashok100% (1)
- Cardiovascular Assessment & Cardiac DisordersDocument57 pagesCardiovascular Assessment & Cardiac DisordersgtsantosNo ratings yet
- IschemicHeartDisease LectureDocument64 pagesIschemicHeartDisease Lectureahmad usmanNo ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- 42 Kelainanpatologi Cardiovasc Dr. DianDocument126 pages42 Kelainanpatologi Cardiovasc Dr. DianSurya ArhNo ratings yet
- Cor Pulmonale: Peter Celec P Ete Rcelec at GM Ail. Com W W W. Imbm. SKDocument108 pagesCor Pulmonale: Peter Celec P Ete Rcelec at GM Ail. Com W W W. Imbm. SKAppry M SilabanNo ratings yet
- Physiology in CirculationDocument54 pagesPhysiology in CirculationPrincess CabilesNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- AtherosclerosisDocument5 pagesAtherosclerosisJoanne LagusadNo ratings yet
- Caronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNDocument32 pagesCaronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNMargaret Xaira Rubio MercadoNo ratings yet
- Cardiovascular SystemDocument17 pagesCardiovascular SystemIbrahem SayedNo ratings yet
- CHF & Cardiac ArrestDocument12 pagesCHF & Cardiac ArrestRadhika BirlaNo ratings yet
- Cardiovascular DiseaseDocument27 pagesCardiovascular DiseaseKyrajane EsguerraNo ratings yet
- Alfonso Lopez CardiovascularDocument15 pagesAlfonso Lopez Cardiovascularjaniceli0207100% (1)
- Cardiovascular FunctionDocument5 pagesCardiovascular FunctionJohn Fritz Gerald BascoNo ratings yet
- Coronary Artery Diseases: Ms Flavi Almeida 1 Year MSC Zukekha Nursing College ManagaloreDocument109 pagesCoronary Artery Diseases: Ms Flavi Almeida 1 Year MSC Zukekha Nursing College ManagalorePriyaNo ratings yet
- Heart FailureDocument10 pagesHeart Failureurmila prajapatiNo ratings yet
- Exercise PhysiologyDocument24 pagesExercise PhysiologyMohammed AlharbiNo ratings yet
- Cardiovascular DisorderDocument4 pagesCardiovascular Disorderhxqf25mbvvNo ratings yet
- Ischemic Heart DiseaseDocument39 pagesIschemic Heart DiseaserahulbafnaeNo ratings yet
- As SNAB Revision NotesDocument49 pagesAs SNAB Revision NotesXneo KMeng 茗茗 ~No ratings yet
- Prepared By: Maria Lourdes P. SagunDocument50 pagesPrepared By: Maria Lourdes P. SagunAGLDNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Summary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartFrom EverandSummary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)From EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)No ratings yet
- Beating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartFrom EverandBeating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartNo ratings yet
- TV 2021Document17 pagesTV 2021c4fcz9dj4fNo ratings yet
- Power Point Panic AttackDocument7 pagesPower Point Panic Attackfrancis00090No ratings yet
- Carlson (7E) : Powerpoint Lecture OutlineDocument29 pagesCarlson (7E) : Powerpoint Lecture Outlinechat gazaNo ratings yet
- Basic Principles of Mechanical Ventilation Andventilator GraphicsDocument70 pagesBasic Principles of Mechanical Ventilation Andventilator GraphicsLauraAlvarezMulettNo ratings yet
- 10 Basic First AidDocument21 pages10 Basic First AidRUSTOM JAKENo ratings yet
- Cardiovascular - HeartDocument57 pagesCardiovascular - HeartCla NuvalNo ratings yet
- Allen 2013, Revisión TSSTDocument31 pagesAllen 2013, Revisión TSSTSara Puig PérezNo ratings yet
- CVP Vs Peep CorrectedDocument15 pagesCVP Vs Peep Correctedsabihul islamNo ratings yet
- Anatomy and Physiology II Outline NUTRITION (22755) - RADocument6 pagesAnatomy and Physiology II Outline NUTRITION (22755) - RArahafahmed20043No ratings yet
- Tranchea NotesDocument1 pageTranchea NotesStasinopoulou Maria ElisavetNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument72 pagesDrugs Acting On The Autonomic Nervous SystemDyang Wulan AprilianiNo ratings yet
- Basics of Cardiopulmonary Bypass.10Document8 pagesBasics of Cardiopulmonary Bypass.10Chaaru ShaarmaNo ratings yet
- Lecture 02 Forensic ThanatologyDocument29 pagesLecture 02 Forensic ThanatologyRoman Mamun100% (1)
- Arawali Veterinary College Bajor, SikarDocument8 pagesArawali Veterinary College Bajor, Sikarashish kumarNo ratings yet
- Parts of The Digestive System Crossword WorksheetDocument2 pagesParts of The Digestive System Crossword WorksheetGian SiblarioNo ratings yet
- Electrolytes New - 1Document186 pagesElectrolytes New - 1Annamae Therese MartinezNo ratings yet
- Respiration Lec10 SlidesDocument29 pagesRespiration Lec10 SlidesHussain IbrahimNo ratings yet
- Introduction To The Ans (TUSOM Pharmwiki)Document1 pageIntroduction To The Ans (TUSOM Pharmwiki)Dorina98No ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Stages of SleepDocument16 pagesStages of SleepMelanie100% (1)
- Campbell Biology Australian and New Zealand 11th Edition Urry Test BankDocument20 pagesCampbell Biology Australian and New Zealand 11th Edition Urry Test Bankscarletnur0hxdr100% (35)
- Biology-Ch 30 Notes On Respiratory and Circulatory SystemsDocument35 pagesBiology-Ch 30 Notes On Respiratory and Circulatory SystemsMarkOrdonoNo ratings yet
- 19-20 Midterm ExamDocument3 pages19-20 Midterm ExamDeona Faye PantasNo ratings yet
- Detailed Lesson Plan in Science 9Document7 pagesDetailed Lesson Plan in Science 9IRISNo ratings yet
- Emergency Ab Osce 2017Document22 pagesEmergency Ab Osce 2017Alwaallh MohammedNo ratings yet
- BLS Manual For Online - Clerks PDFDocument41 pagesBLS Manual For Online - Clerks PDFMiko Vargas100% (2)
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- Dengue Hemorrhagic FeverDocument12 pagesDengue Hemorrhagic FeverzeeNo ratings yet
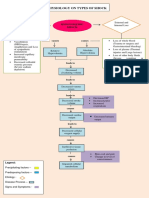
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet























































































Download as pdf or txt
You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Josephson - Clinical Cardiac Electrophysiology Techniques AnDocument451 pagesJosephson - Clinical Cardiac Electrophysiology Techniques Anmobilica100% (5)
- Congestive Heart FailureDocument8 pagesCongestive Heart Failureiancel_038893% (27)
- Case Study Congestive Heart Failure Patho)Document8 pagesCase Study Congestive Heart Failure Patho)Mj Silva100% (3)
- A1 CardioDocument98 pagesA1 CardioTikboy TaliliNo ratings yet
- Chapter 41. Nursing Care of The Child With A Cardiovascular Disorder TermDocument11 pagesChapter 41. Nursing Care of The Child With A Cardiovascular Disorder TermJœnríčk AzueloNo ratings yet
- Lecture On Human Circulatory SystemDocument7 pagesLecture On Human Circulatory SystemolandiolettyNo ratings yet
- 3 Review CvsDocument108 pages3 Review CvsSaif AlzateemhNo ratings yet
- 1cardiovascular System DisordersDocument13 pages1cardiovascular System DisordersArvin MalondrasNo ratings yet
- Assessment of The Cardiovascular SystemDocument48 pagesAssessment of The Cardiovascular Systemkimberlyrwarren8817No ratings yet
- PerfusionDocument9 pagesPerfusionAmanda Brittain100% (2)
- HypertensionDocument11 pagesHypertensionJyoti singhNo ratings yet
- 18 Heartpart1 Basiccongestiveheartfailure 110919083613 Phpapp01Document43 pages18 Heartpart1 Basiccongestiveheartfailure 110919083613 Phpapp01Atikah PurnamasariNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- Medical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Cardiovascular SystemDocument43 pagesMedical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Cardiovascular Systemsarah morleyNo ratings yet
- The Circulatory SystemDocument25 pagesThe Circulatory SystemEduardson PHNo ratings yet
- Heart Failure: Presented By: Leslie PaguioDocument38 pagesHeart Failure: Presented By: Leslie PaguioLeslie PaguioNo ratings yet
- Med Surg 2Document76 pagesMed Surg 2sham gowliNo ratings yet
- Cardiovascular and Heart DiseaseDocument65 pagesCardiovascular and Heart DiseasesarazalnoonNo ratings yet
- Lesson9 Cardiovascular AssessmentDocument21 pagesLesson9 Cardiovascular AssessmentDennis Nabor Muñoz, RN,RMNo ratings yet
- Cardiology - Dr. Allam 2021Document141 pagesCardiology - Dr. Allam 2021MohammedNo ratings yet
- 3 Heart FailureDocument8 pages3 Heart FailureAudrey Ann AcobNo ratings yet
- Cardiovascular System: Presented byDocument76 pagesCardiovascular System: Presented bySoma Al-mutairiNo ratings yet
- AP Refresher 1 Heart PhysiologyDocument52 pagesAP Refresher 1 Heart Physiologymaxwell amponsahNo ratings yet
- Cardivascular SystemDocument11 pagesCardivascular SystemAnneMarielleManaloNo ratings yet
- Lec 3 - Circulatory SystemDocument9 pagesLec 3 - Circulatory SystemJewel Jehd AlegriaNo ratings yet
- CVS 3-3 PDFDocument24 pagesCVS 3-3 PDFafaq alismailiNo ratings yet
- Cardiovascular SystemDocument11 pagesCardiovascular SystemРахым ХасеновNo ratings yet
- Nursing Management of Patient With CCFDocument34 pagesNursing Management of Patient With CCFJayarani Ashok100% (1)
- Cardiovascular Assessment & Cardiac DisordersDocument57 pagesCardiovascular Assessment & Cardiac DisordersgtsantosNo ratings yet
- IschemicHeartDisease LectureDocument64 pagesIschemicHeartDisease Lectureahmad usmanNo ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- 42 Kelainanpatologi Cardiovasc Dr. DianDocument126 pages42 Kelainanpatologi Cardiovasc Dr. DianSurya ArhNo ratings yet
- Cor Pulmonale: Peter Celec P Ete Rcelec at GM Ail. Com W W W. Imbm. SKDocument108 pagesCor Pulmonale: Peter Celec P Ete Rcelec at GM Ail. Com W W W. Imbm. SKAppry M SilabanNo ratings yet
- Physiology in CirculationDocument54 pagesPhysiology in CirculationPrincess CabilesNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- AtherosclerosisDocument5 pagesAtherosclerosisJoanne LagusadNo ratings yet
- Caronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNDocument32 pagesCaronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNMargaret Xaira Rubio MercadoNo ratings yet
- Cardiovascular SystemDocument17 pagesCardiovascular SystemIbrahem SayedNo ratings yet
- CHF & Cardiac ArrestDocument12 pagesCHF & Cardiac ArrestRadhika BirlaNo ratings yet
- Cardiovascular DiseaseDocument27 pagesCardiovascular DiseaseKyrajane EsguerraNo ratings yet
- Alfonso Lopez CardiovascularDocument15 pagesAlfonso Lopez Cardiovascularjaniceli0207100% (1)
- Cardiovascular FunctionDocument5 pagesCardiovascular FunctionJohn Fritz Gerald BascoNo ratings yet
- Coronary Artery Diseases: Ms Flavi Almeida 1 Year MSC Zukekha Nursing College ManagaloreDocument109 pagesCoronary Artery Diseases: Ms Flavi Almeida 1 Year MSC Zukekha Nursing College ManagalorePriyaNo ratings yet
- Heart FailureDocument10 pagesHeart Failureurmila prajapatiNo ratings yet
- Exercise PhysiologyDocument24 pagesExercise PhysiologyMohammed AlharbiNo ratings yet
- Cardiovascular DisorderDocument4 pagesCardiovascular Disorderhxqf25mbvvNo ratings yet
- Ischemic Heart DiseaseDocument39 pagesIschemic Heart DiseaserahulbafnaeNo ratings yet
- As SNAB Revision NotesDocument49 pagesAs SNAB Revision NotesXneo KMeng 茗茗 ~No ratings yet
- Prepared By: Maria Lourdes P. SagunDocument50 pagesPrepared By: Maria Lourdes P. SagunAGLDNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Summary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartFrom EverandSummary of Chris Case, Dr. John Mandrola & Lennard Zinn's The Haywire HeartNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)From EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)No ratings yet
- Beating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartFrom EverandBeating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartNo ratings yet
- TV 2021Document17 pagesTV 2021c4fcz9dj4fNo ratings yet
- Power Point Panic AttackDocument7 pagesPower Point Panic Attackfrancis00090No ratings yet
- Carlson (7E) : Powerpoint Lecture OutlineDocument29 pagesCarlson (7E) : Powerpoint Lecture Outlinechat gazaNo ratings yet
- Basic Principles of Mechanical Ventilation Andventilator GraphicsDocument70 pagesBasic Principles of Mechanical Ventilation Andventilator GraphicsLauraAlvarezMulettNo ratings yet
- 10 Basic First AidDocument21 pages10 Basic First AidRUSTOM JAKENo ratings yet
- Cardiovascular - HeartDocument57 pagesCardiovascular - HeartCla NuvalNo ratings yet
- Allen 2013, Revisión TSSTDocument31 pagesAllen 2013, Revisión TSSTSara Puig PérezNo ratings yet
- CVP Vs Peep CorrectedDocument15 pagesCVP Vs Peep Correctedsabihul islamNo ratings yet
- Anatomy and Physiology II Outline NUTRITION (22755) - RADocument6 pagesAnatomy and Physiology II Outline NUTRITION (22755) - RArahafahmed20043No ratings yet
- Tranchea NotesDocument1 pageTranchea NotesStasinopoulou Maria ElisavetNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument72 pagesDrugs Acting On The Autonomic Nervous SystemDyang Wulan AprilianiNo ratings yet
- Basics of Cardiopulmonary Bypass.10Document8 pagesBasics of Cardiopulmonary Bypass.10Chaaru ShaarmaNo ratings yet
- Lecture 02 Forensic ThanatologyDocument29 pagesLecture 02 Forensic ThanatologyRoman Mamun100% (1)
- Arawali Veterinary College Bajor, SikarDocument8 pagesArawali Veterinary College Bajor, Sikarashish kumarNo ratings yet
- Parts of The Digestive System Crossword WorksheetDocument2 pagesParts of The Digestive System Crossword WorksheetGian SiblarioNo ratings yet
- Electrolytes New - 1Document186 pagesElectrolytes New - 1Annamae Therese MartinezNo ratings yet
- Respiration Lec10 SlidesDocument29 pagesRespiration Lec10 SlidesHussain IbrahimNo ratings yet
- Introduction To The Ans (TUSOM Pharmwiki)Document1 pageIntroduction To The Ans (TUSOM Pharmwiki)Dorina98No ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Stages of SleepDocument16 pagesStages of SleepMelanie100% (1)
- Campbell Biology Australian and New Zealand 11th Edition Urry Test BankDocument20 pagesCampbell Biology Australian and New Zealand 11th Edition Urry Test Bankscarletnur0hxdr100% (35)
- Biology-Ch 30 Notes On Respiratory and Circulatory SystemsDocument35 pagesBiology-Ch 30 Notes On Respiratory and Circulatory SystemsMarkOrdonoNo ratings yet
- 19-20 Midterm ExamDocument3 pages19-20 Midterm ExamDeona Faye PantasNo ratings yet
- Detailed Lesson Plan in Science 9Document7 pagesDetailed Lesson Plan in Science 9IRISNo ratings yet
- Emergency Ab Osce 2017Document22 pagesEmergency Ab Osce 2017Alwaallh MohammedNo ratings yet
- BLS Manual For Online - Clerks PDFDocument41 pagesBLS Manual For Online - Clerks PDFMiko Vargas100% (2)
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- Dengue Hemorrhagic FeverDocument12 pagesDengue Hemorrhagic FeverzeeNo ratings yet
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet