Download as pdf or txt
You might also like
- The HeartDocument13 pagesThe HeartMary Ann SacramentoNo ratings yet
- Components of The Cardiovascular SystemDocument23 pagesComponents of The Cardiovascular SystemMr. DummyNo ratings yet
- Riya Arya - 21msc1279 - Biology For ChemistsDocument13 pagesRiya Arya - 21msc1279 - Biology For ChemistsSwadesh SenNo ratings yet
- Module Cardiovascular System Anatomy and PhysiologyDocument9 pagesModule Cardiovascular System Anatomy and PhysiologyPATRICIA KAYE RIONo ratings yet
- Cardiac CycleDocument6 pagesCardiac CycleShahina ShayneNo ratings yet
- HeartDocument35 pagesHeartislamicmedia188No ratings yet
- Chapter 2 - CardiovascularDocument74 pagesChapter 2 - CardiovascularNoriani ZakariaNo ratings yet
- محاظرة تشريح وفسلجة القلب والاوعية الدمويهDocument29 pagesمحاظرة تشريح وفسلجة القلب والاوعية الدمويهfaroq AlromimahNo ratings yet
- Cardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPDocument90 pagesCardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPAndra HijratulNo ratings yet
- Cardiovascular System: by DR Saad ZafarDocument154 pagesCardiovascular System: by DR Saad Zafarkhalidtalal8000No ratings yet
- Chapter 11 Cardiovascular SystemDocument6 pagesChapter 11 Cardiovascular SystemClarisse Anne QuinonesNo ratings yet
- Anatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, LudhianaDocument56 pagesAnatomy & Physiology of Heart: BY: Mr. Anurag Lecturer College of Nursing DMC & H, Ludhianapreet kaurNo ratings yet
- Week 11 THE HEART 2021Document60 pagesWeek 11 THE HEART 2021Huffy PotterNo ratings yet
- Chapter 20 Heart and Neck VesselsDocument10 pagesChapter 20 Heart and Neck Vesselsannoja selvaNo ratings yet
- Session 5Document41 pagesSession 5tazebNo ratings yet
- Anatomy and Physiology of The HeartDocument9 pagesAnatomy and Physiology of The HeartNina Anne ParacadNo ratings yet
- Heart Anatomy: LocationDocument45 pagesHeart Anatomy: LocationZaira100% (1)
- Cardiovascular SystemDocument101 pagesCardiovascular SystemBanessa Mae GarcianoNo ratings yet
- Cardiovascular System - The HeartDocument77 pagesCardiovascular System - The HeartZiraili VidalNo ratings yet
- Assignment On Anatomy and Physiology of Heart: Submitted By: Submitted To: Jayita Gayen Madam S. PoddarDocument10 pagesAssignment On Anatomy and Physiology of Heart: Submitted By: Submitted To: Jayita Gayen Madam S. PoddarJayita Gayen DuttaNo ratings yet
- Stern Chap 15Document16 pagesStern Chap 15evansternhgpNo ratings yet
- CardioDocument30 pagesCardioPamela LusungNo ratings yet
- Cardiovascular System SonDocument36 pagesCardiovascular System SonsmilingjudgeNo ratings yet
- HeartDocument36 pagesHeartSoovendran VaradarajanNo ratings yet
- Cardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryDocument73 pagesCardiovascular System: Presented by DR Aparna Ramachandran Mds 1 Dept of Public Health DentistryAparna RamachandranNo ratings yet
- H.A. Assessing Heart and Neck VesselsDocument55 pagesH.A. Assessing Heart and Neck VesselsMc Ramil B. PraderoNo ratings yet
- EKG Study Guide RevisedDocument29 pagesEKG Study Guide Revisedflashyboy506No ratings yet
- 1 Cardiovascular SystemDocument51 pages1 Cardiovascular SystemChryzl JoyNo ratings yet
- Lec 4Document59 pagesLec 4علي صفاء عبد الزهرهNo ratings yet
- Electropĥysiologioe CardiaqueDocument209 pagesElectropĥysiologioe CardiaqueAntoine TakoNo ratings yet
- Cardiovascular SystemDocument18 pagesCardiovascular SystemDeep RoyNo ratings yet
- Circulatory SystemDocument44 pagesCirculatory Systemayman.hazem66No ratings yet
- DOC-20220905-WA0036. (1) - WDocument6 pagesDOC-20220905-WA0036. (1) - WPizzaNo ratings yet
- The Cardiovascular System: Click To Edit Master Subtitle StyleDocument65 pagesThe Cardiovascular System: Click To Edit Master Subtitle StyleBien EstrellaNo ratings yet
- L6 7 CVS (2022) PDFDocument51 pagesL6 7 CVS (2022) PDFFung Shan CheungNo ratings yet
- Hear Structure NotesDocument27 pagesHear Structure NotesRaifa FathimaNo ratings yet
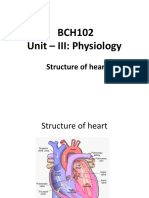
- BCH102 Unit - III: Physiology: Structure of HeartDocument17 pagesBCH102 Unit - III: Physiology: Structure of Heartdivya vajpayeeNo ratings yet
- Anatomy and Physiology - Circulatory System - The HeartDocument14 pagesAnatomy and Physiology - Circulatory System - The Heartxuxi dulNo ratings yet
- Heart Blood HistoDocument53 pagesHeart Blood HistoAnonymous 52lBinNo ratings yet
- Cardiovascular SystemDocument34 pagesCardiovascular Systemurooj100% (1)
- Cardiovascular System: Prepared by Samjhana GautamDocument71 pagesCardiovascular System: Prepared by Samjhana GautamSamjhana GautamNo ratings yet
- Cardiovascular System: Blood VesselsDocument12 pagesCardiovascular System: Blood VesselsSoniyaJI84100% (1)
- Cardiovascular System BSN 1Document16 pagesCardiovascular System BSN 1Arianne Jen GenotivaNo ratings yet
- Cardiovascular SystemDocument12 pagesCardiovascular SystemDevendra RawatNo ratings yet
- Circulatory System in AnimalsDocument42 pagesCirculatory System in AnimalsAlaina SmithNo ratings yet
- 1 Anatomy and PhysiologyDocument25 pages1 Anatomy and PhysiologyMichelle Dona MirallesNo ratings yet
- Cadiac Cycle, Heart Sound, ECG, HypertensionDocument110 pagesCadiac Cycle, Heart Sound, ECG, HypertensionNilesh100% (1)
- Electrical Conduction in The HeartDocument35 pagesElectrical Conduction in The HeartNormasnizam Mohd NoorNo ratings yet
- The Circulatory System P2Document17 pagesThe Circulatory System P2Kristal CampbellNo ratings yet
- IGCSE Biology Transport in Animals NotesDocument62 pagesIGCSE Biology Transport in Animals NotesSir AhmedNo ratings yet
- Cardiovascular System: More Than Just The HeartDocument34 pagesCardiovascular System: More Than Just The HearteliseudesafateNo ratings yet
- WK 1& 2 LectureDocument149 pagesWK 1& 2 LectureElma SekikorolevuNo ratings yet
- Ila College of Health Kuje: Cardiovascular SystemDocument24 pagesIla College of Health Kuje: Cardiovascular SystemDaniel DendaNo ratings yet
- The Cardiovascular System: A. KabweDocument117 pagesThe Cardiovascular System: A. KabwePeter ChipatelaNo ratings yet
- Anatomy of The HeartDocument28 pagesAnatomy of The HeartHerman DjawaNo ratings yet
- Cardiovascular System: Dr. Mohanad R. AlwanDocument46 pagesCardiovascular System: Dr. Mohanad R. Alwanmohanad11No ratings yet
- Heart and CirculationDocument63 pagesHeart and CirculationNuraina SakinaNo ratings yet
- 1 Heart Anatomy and FunctionDocument38 pages1 Heart Anatomy and Functionsyanita dwi nanda Sulistyani putriNo ratings yet
- The HeartDocument65 pagesThe HeartMichael SamaniegoNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Nutrition and Diet TherapyDocument16 pagesNutrition and Diet TherapyMary Ann SacramentoNo ratings yet
- Med Surg Peri OperativeDocument18 pagesMed Surg Peri OperativeMary Ann SacramentoNo ratings yet
- Health AsseDocument128 pagesHealth AsseMary Ann SacramentoNo ratings yet
- Blood Vessels and CirculationDocument11 pagesBlood Vessels and CirculationMary Ann SacramentoNo ratings yet
- Reflection PaperDocument1 pageReflection PaperMary Ann SacramentoNo ratings yet
- Finals ReviewerDocument3 pagesFinals ReviewerMary Ann SacramentoNo ratings yet
- Patient InformationDocument1 pagePatient InformationMary Ann SacramentoNo ratings yet
- Reflection PaperDocument2 pagesReflection PaperMary Ann SacramentoNo ratings yet
- Kardex 001Document2 pagesKardex 001Mary Ann SacramentoNo ratings yet
- Doctors OrderDocument1 pageDoctors OrderMary Ann SacramentoNo ratings yet
- CHN Final TopicsDocument52 pagesCHN Final TopicsMary Ann SacramentoNo ratings yet
- Bureau of HospitalsDocument1 pageBureau of HospitalsMary Ann SacramentoNo ratings yet