
Medical Waiver (Updated) PDF
Medical Waiver (Updated) PDF
You might also like
- NCDC-2 Physical Health Inventory Form A4Document6 pagesNCDC-2 Physical Health Inventory Form A4knock medinaNo ratings yet
- Inss 4Document2 pagesInss 4api-2582064670% (1)
- Health Assessment FormDocument3 pagesHealth Assessment FormDarlen RabanoNo ratings yet
- FIELDTRIPMEDICALRELEASEDocument1 pageFIELDTRIPMEDICALRELEASETakuma OkadaNo ratings yet
- NEW OB RISK NICU CASE STUDY FORMAT For 2nd YearDocument16 pagesNEW OB RISK NICU CASE STUDY FORMAT For 2nd YearDrex CuritanaNo ratings yet
- Marietta City Schools' Athletic Physical, Insurance, and Consent FormDocument6 pagesMarietta City Schools' Athletic Physical, Insurance, and Consent FormPatavious SorrellNo ratings yet
- FORM Health HistoryDocument2 pagesFORM Health HistoryxxxhbkxxxNo ratings yet
- MedicalHistory PDFDocument1 pageMedicalHistory PDFGanesh NNo ratings yet
- Health Profile - Southeast Missouri State University: Please Note The FollowingDocument1 pageHealth Profile - Southeast Missouri State University: Please Note The FollowingQuynh Lam LeNo ratings yet
- NYSSO Medical FormDocument1 pageNYSSO Medical Formmamirori1No ratings yet
- Consent FormsDocument2 pagesConsent FormsKristeline MedelNo ratings yet
- CDC Data Collection Long FormDocument13 pagesCDC Data Collection Long FormBanzai Health Private LimitedNo ratings yet
- Medical Report - InglêsDocument1 pageMedical Report - InglêsthaismarquesntNo ratings yet
- (IL) FMLA Certification Form Employee Condition Beatriz RuizDocument5 pages(IL) FMLA Certification Form Employee Condition Beatriz RuizBeatriz RuizNo ratings yet
- New Patient RegistrationDocument2 pagesNew Patient Registrationnaveenmi2100% (1)
- Child BioDocument3 pagesChild BioPammNo ratings yet
- Leetaloo Pediatric Therapy: General InformationDocument7 pagesLeetaloo Pediatric Therapy: General InformationrabiyaNo ratings yet
- Physical FormDocument2 pagesPhysical Formapi-670925736No ratings yet
- Medical Information and Treatment ReleaseDocument3 pagesMedical Information and Treatment Releasedianesimard85No ratings yet
- BSN 3A Group 8 Research ToolDocument8 pagesBSN 3A Group 8 Research ToolChirber MalgapuNo ratings yet
- Pediatric Neurological History and PhysicalDocument7 pagesPediatric Neurological History and PhysicalPaiin KiillerNo ratings yet
- Physical Form ADocument4 pagesPhysical Form Aapi-3958058100% (1)
- Fitness Aziz AlhaidariDocument2 pagesFitness Aziz Alhaidariabdulaziz saif ali mansoorNo ratings yet
- Parental Consent Form: To Whom It May ConcernDocument4 pagesParental Consent Form: To Whom It May ConcernNorman PolilinNo ratings yet
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- 2008SportsPhys FormDocument2 pages2008SportsPhys FormbbruntNo ratings yet
- Medical History FormDocument2 pagesMedical History Formnnma0127No ratings yet
- 130 Physicians-Report 7-21-2023Document2 pages130 Physicians-Report 7-21-2023medisnadaNo ratings yet
- Consent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024Document4 pagesConsent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024sage.ebony.meadowNo ratings yet
- Clearance For Safe Exercise Participation: I. Health HistoryDocument3 pagesClearance For Safe Exercise Participation: I. Health HistoryejjohnsoNo ratings yet
- Confidential Parent Occupational Physical Therapy 01 15Document7 pagesConfidential Parent Occupational Physical Therapy 01 15Giselle Pezoa WattsonNo ratings yet
- Form A: Use This Form For Initial Physical ExamDocument4 pagesForm A: Use This Form For Initial Physical ExamLisa WillardsonNo ratings yet
- Athletic Physical and Consent FormsDocument4 pagesAthletic Physical and Consent FormsJohnny TuNo ratings yet
- KHP Activity Class Par-QDocument2 pagesKHP Activity Class Par-Qapi-741759851No ratings yet
- Medical+Form InglesDocument1 pageMedical+Form Inglescidaparecida141977No ratings yet
- Baltimore Medical ReleaseDocument3 pagesBaltimore Medical ReleaseDanielNo ratings yet
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiNo ratings yet
- FORM B - Physical - STUDENTDocument4 pagesFORM B - Physical - STUDENTJane PNo ratings yet
- School Medical FormDocument2 pagesSchool Medical FormKendy SalvadorNo ratings yet
- Child Intake2017Document5 pagesChild Intake2017api-358418536No ratings yet
- PHILPLANS Health Statement Form 1Document1 pagePHILPLANS Health Statement Form 1romelgregoriotorresNo ratings yet
- St. George AppDocument9 pagesSt. George AppFutureDDSNo ratings yet
- Physical Exam FormDocument1 pagePhysical Exam FormEthan AtchleyNo ratings yet
- Personal Training Health History QuestionaireDocument4 pagesPersonal Training Health History QuestionaireJamie StaggNo ratings yet
- DOAC QuestionnaireDocument2 pagesDOAC QuestionnaireMuniba NasimNo ratings yet
- Health Assessment FormDocument3 pagesHealth Assessment FormtumilidNo ratings yet
- Parents Consent 2023Document2 pagesParents Consent 2023danosoprince39No ratings yet
- TUE - WADA Version 2016-EnDocument4 pagesTUE - WADA Version 2016-EnYannick MOSSUSNo ratings yet
- Child & Adolescent Intake QuestionnaireDocument15 pagesChild & Adolescent Intake QuestionnaireSadar Psychological and Sports Center100% (2)
- Catholic Faith: Clinical Worksheet: Nursing Process Care PlanDocument18 pagesCatholic Faith: Clinical Worksheet: Nursing Process Care Planmuhammad adilNo ratings yet
- Health FormDocument3 pagesHealth Formkylaclowy jimenezNo ratings yet
- Camper Health History Form: American Academy of Pediatrics Council On School Health, & Association of Camp NursesDocument4 pagesCamper Health History Form: American Academy of Pediatrics Council On School Health, & Association of Camp Nurses414chandraNo ratings yet
- Student Athlete ParticipationDocument4 pagesStudent Athlete Participationlhmiles2No ratings yet
- Prelim Exam Hope 2 I. Choose The Correct Answer From The Box - Right in On The Space ProvidedDocument2 pagesPrelim Exam Hope 2 I. Choose The Correct Answer From The Box - Right in On The Space ProvidedCync KlayNo ratings yet
- RYERSONDocument2 pagesRYERSONJeremey Julian PonrajahNo ratings yet
- NHH (Preggy-Michelle Alindato)Document7 pagesNHH (Preggy-Michelle Alindato)Kate MarianoNo ratings yet
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimNo ratings yet
- Form WH-380-F Asistence MjekesoreDocument3 pagesForm WH-380-F Asistence MjekesoreshpkvirageNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Cataract Surgery - : After The ProcedureDocument16 pagesCataract Surgery - : After The ProcedureAmandeep Singh GandhiNo ratings yet
- Genetics 101 + ExercisesDocument36 pagesGenetics 101 + ExercisesSanaa Samko100% (1)
- With Answers No RationaleDocument41 pagesWith Answers No RationaleronnaxNo ratings yet
- Corrosive PoisonsDocument55 pagesCorrosive PoisonsIoana IsarieNo ratings yet
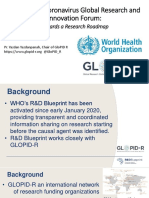
- Global Research and Innovation Forum PresentationDocument122 pagesGlobal Research and Innovation Forum PresentationRazu BhuiyanNo ratings yet
- Belize Medical Fitness CertificateDocument2 pagesBelize Medical Fitness CertificateSea BlackNo ratings yet
- Kawasaki Disease NCPDocument2 pagesKawasaki Disease NCPRay Jhunel Cemine Pascual100% (2)
- Transaction Date: 04/02/2021 01:54 PM (Singapore Time)Document3 pagesTransaction Date: 04/02/2021 01:54 PM (Singapore Time)Putri Agatha C.RNo ratings yet
- Intrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSDocument72 pagesIntrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSapi-3703352No ratings yet
- Health and Healing in Colonial America - EditedDocument5 pagesHealth and Healing in Colonial America - EditedBrian KipkoechNo ratings yet
- Flagellates LabDocument4 pagesFlagellates LabWilliam RamirezNo ratings yet
- Developing My Bleeding Disorders Community Mybdc A Community-Powered Registry To Provide A 360-View of Living With A Bleeding DisorderDocument23 pagesDeveloping My Bleeding Disorders Community Mybdc A Community-Powered Registry To Provide A 360-View of Living With A Bleeding Disorderkalinayak.prasadNo ratings yet
- M14 CT Acupuncture and Traditional Chinese MedicineDocument19 pagesM14 CT Acupuncture and Traditional Chinese MedicinenerdmojoNo ratings yet
- MetamizoleDocument1 pageMetamizoleOliviaNo ratings yet
- Chapter - 2 Microorganisms (Continuation)Document2 pagesChapter - 2 Microorganisms (Continuation)ARSHAD JAMILNo ratings yet
- R01 Revitalife Drip Protocol - UPDATED 9-19-2018Document10 pagesR01 Revitalife Drip Protocol - UPDATED 9-19-2018Eking InNo ratings yet
- COVID Is The-Virus-That-Does-Not-ExistDocument41 pagesCOVID Is The-Virus-That-Does-Not-ExistHansley Templeton Cook100% (2)
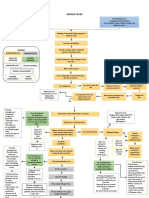
- Concept Map Dengue FeverDocument2 pagesConcept Map Dengue FeverChelsyann FerolinoNo ratings yet
- Pediatric OSCE Pictures: For UndergraduatesDocument70 pagesPediatric OSCE Pictures: For UndergraduatesShehab MhmdNo ratings yet
- Nursing Worksheet Template 1 1Document2 pagesNursing Worksheet Template 1 1api-651287771No ratings yet
- Dr. Muslim N. Saeed Family & Community Medicine Dept. March 14, 2022Document10 pagesDr. Muslim N. Saeed Family & Community Medicine Dept. March 14, 2022hussain AltaherNo ratings yet
- Role and Potential of Modern Ultrasound in Pediatric Abdominal ImagingDocument18 pagesRole and Potential of Modern Ultrasound in Pediatric Abdominal ImagingRafael CamachoNo ratings yet
- Types of MeningitisDocument6 pagesTypes of MeningitisARISNo ratings yet
- Midterm Psych NSG Nclex Test BanksDocument19 pagesMidterm Psych NSG Nclex Test BanksAliza AlyyNo ratings yet
- Management of Common Respiratory Infections in Children in IndiaDocument60 pagesManagement of Common Respiratory Infections in Children in IndiaSukumar SubuNo ratings yet
- Diverticular Disease A Review On Pathophysiology and Recent EvidenceDocument6 pagesDiverticular Disease A Review On Pathophysiology and Recent EvidenceIsabella María GantivarNo ratings yet
- DRUG STUDY OmeprazoleDocument3 pagesDRUG STUDY OmeprazoleCelline Isabelle ReyesNo ratings yet
- Fernandez Doctor - Goya's Mental Illness 1994Document6 pagesFernandez Doctor - Goya's Mental Illness 1994FranciscoNo ratings yet
- EnglishDocument5 pagesEnglishMarthe KateNo ratings yet
- History Taking & MSEDocument25 pagesHistory Taking & MSEMahmoud SalehNo ratings yet























































































Download as pdf or txt
You might also like
- NCDC-2 Physical Health Inventory Form A4Document6 pagesNCDC-2 Physical Health Inventory Form A4knock medinaNo ratings yet
- Inss 4Document2 pagesInss 4api-2582064670% (1)
- Health Assessment FormDocument3 pagesHealth Assessment FormDarlen RabanoNo ratings yet
- FIELDTRIPMEDICALRELEASEDocument1 pageFIELDTRIPMEDICALRELEASETakuma OkadaNo ratings yet
- NEW OB RISK NICU CASE STUDY FORMAT For 2nd YearDocument16 pagesNEW OB RISK NICU CASE STUDY FORMAT For 2nd YearDrex CuritanaNo ratings yet
- Marietta City Schools' Athletic Physical, Insurance, and Consent FormDocument6 pagesMarietta City Schools' Athletic Physical, Insurance, and Consent FormPatavious SorrellNo ratings yet
- FORM Health HistoryDocument2 pagesFORM Health HistoryxxxhbkxxxNo ratings yet
- MedicalHistory PDFDocument1 pageMedicalHistory PDFGanesh NNo ratings yet
- Health Profile - Southeast Missouri State University: Please Note The FollowingDocument1 pageHealth Profile - Southeast Missouri State University: Please Note The FollowingQuynh Lam LeNo ratings yet
- NYSSO Medical FormDocument1 pageNYSSO Medical Formmamirori1No ratings yet
- Consent FormsDocument2 pagesConsent FormsKristeline MedelNo ratings yet
- CDC Data Collection Long FormDocument13 pagesCDC Data Collection Long FormBanzai Health Private LimitedNo ratings yet
- Medical Report - InglêsDocument1 pageMedical Report - InglêsthaismarquesntNo ratings yet
- (IL) FMLA Certification Form Employee Condition Beatriz RuizDocument5 pages(IL) FMLA Certification Form Employee Condition Beatriz RuizBeatriz RuizNo ratings yet
- New Patient RegistrationDocument2 pagesNew Patient Registrationnaveenmi2100% (1)
- Child BioDocument3 pagesChild BioPammNo ratings yet
- Leetaloo Pediatric Therapy: General InformationDocument7 pagesLeetaloo Pediatric Therapy: General InformationrabiyaNo ratings yet
- Physical FormDocument2 pagesPhysical Formapi-670925736No ratings yet
- Medical Information and Treatment ReleaseDocument3 pagesMedical Information and Treatment Releasedianesimard85No ratings yet
- BSN 3A Group 8 Research ToolDocument8 pagesBSN 3A Group 8 Research ToolChirber MalgapuNo ratings yet
- Pediatric Neurological History and PhysicalDocument7 pagesPediatric Neurological History and PhysicalPaiin KiillerNo ratings yet
- Physical Form ADocument4 pagesPhysical Form Aapi-3958058100% (1)
- Fitness Aziz AlhaidariDocument2 pagesFitness Aziz Alhaidariabdulaziz saif ali mansoorNo ratings yet
- Parental Consent Form: To Whom It May ConcernDocument4 pagesParental Consent Form: To Whom It May ConcernNorman PolilinNo ratings yet
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- 2008SportsPhys FormDocument2 pages2008SportsPhys FormbbruntNo ratings yet
- Medical History FormDocument2 pagesMedical History Formnnma0127No ratings yet
- 130 Physicians-Report 7-21-2023Document2 pages130 Physicians-Report 7-21-2023medisnadaNo ratings yet
- Consent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024Document4 pagesConsent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024sage.ebony.meadowNo ratings yet
- Clearance For Safe Exercise Participation: I. Health HistoryDocument3 pagesClearance For Safe Exercise Participation: I. Health HistoryejjohnsoNo ratings yet
- Confidential Parent Occupational Physical Therapy 01 15Document7 pagesConfidential Parent Occupational Physical Therapy 01 15Giselle Pezoa WattsonNo ratings yet
- Form A: Use This Form For Initial Physical ExamDocument4 pagesForm A: Use This Form For Initial Physical ExamLisa WillardsonNo ratings yet
- Athletic Physical and Consent FormsDocument4 pagesAthletic Physical and Consent FormsJohnny TuNo ratings yet
- KHP Activity Class Par-QDocument2 pagesKHP Activity Class Par-Qapi-741759851No ratings yet
- Medical+Form InglesDocument1 pageMedical+Form Inglescidaparecida141977No ratings yet
- Baltimore Medical ReleaseDocument3 pagesBaltimore Medical ReleaseDanielNo ratings yet
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiNo ratings yet
- FORM B - Physical - STUDENTDocument4 pagesFORM B - Physical - STUDENTJane PNo ratings yet
- School Medical FormDocument2 pagesSchool Medical FormKendy SalvadorNo ratings yet
- Child Intake2017Document5 pagesChild Intake2017api-358418536No ratings yet
- PHILPLANS Health Statement Form 1Document1 pagePHILPLANS Health Statement Form 1romelgregoriotorresNo ratings yet
- St. George AppDocument9 pagesSt. George AppFutureDDSNo ratings yet
- Physical Exam FormDocument1 pagePhysical Exam FormEthan AtchleyNo ratings yet
- Personal Training Health History QuestionaireDocument4 pagesPersonal Training Health History QuestionaireJamie StaggNo ratings yet
- DOAC QuestionnaireDocument2 pagesDOAC QuestionnaireMuniba NasimNo ratings yet
- Health Assessment FormDocument3 pagesHealth Assessment FormtumilidNo ratings yet
- Parents Consent 2023Document2 pagesParents Consent 2023danosoprince39No ratings yet
- TUE - WADA Version 2016-EnDocument4 pagesTUE - WADA Version 2016-EnYannick MOSSUSNo ratings yet
- Child & Adolescent Intake QuestionnaireDocument15 pagesChild & Adolescent Intake QuestionnaireSadar Psychological and Sports Center100% (2)
- Catholic Faith: Clinical Worksheet: Nursing Process Care PlanDocument18 pagesCatholic Faith: Clinical Worksheet: Nursing Process Care Planmuhammad adilNo ratings yet
- Health FormDocument3 pagesHealth Formkylaclowy jimenezNo ratings yet
- Camper Health History Form: American Academy of Pediatrics Council On School Health, & Association of Camp NursesDocument4 pagesCamper Health History Form: American Academy of Pediatrics Council On School Health, & Association of Camp Nurses414chandraNo ratings yet
- Student Athlete ParticipationDocument4 pagesStudent Athlete Participationlhmiles2No ratings yet
- Prelim Exam Hope 2 I. Choose The Correct Answer From The Box - Right in On The Space ProvidedDocument2 pagesPrelim Exam Hope 2 I. Choose The Correct Answer From The Box - Right in On The Space ProvidedCync KlayNo ratings yet
- RYERSONDocument2 pagesRYERSONJeremey Julian PonrajahNo ratings yet
- NHH (Preggy-Michelle Alindato)Document7 pagesNHH (Preggy-Michelle Alindato)Kate MarianoNo ratings yet
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimNo ratings yet
- Form WH-380-F Asistence MjekesoreDocument3 pagesForm WH-380-F Asistence MjekesoreshpkvirageNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Cataract Surgery - : After The ProcedureDocument16 pagesCataract Surgery - : After The ProcedureAmandeep Singh GandhiNo ratings yet
- Genetics 101 + ExercisesDocument36 pagesGenetics 101 + ExercisesSanaa Samko100% (1)
- With Answers No RationaleDocument41 pagesWith Answers No RationaleronnaxNo ratings yet
- Corrosive PoisonsDocument55 pagesCorrosive PoisonsIoana IsarieNo ratings yet
- Global Research and Innovation Forum PresentationDocument122 pagesGlobal Research and Innovation Forum PresentationRazu BhuiyanNo ratings yet
- Belize Medical Fitness CertificateDocument2 pagesBelize Medical Fitness CertificateSea BlackNo ratings yet
- Kawasaki Disease NCPDocument2 pagesKawasaki Disease NCPRay Jhunel Cemine Pascual100% (2)
- Transaction Date: 04/02/2021 01:54 PM (Singapore Time)Document3 pagesTransaction Date: 04/02/2021 01:54 PM (Singapore Time)Putri Agatha C.RNo ratings yet
- Intrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSDocument72 pagesIntrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSapi-3703352No ratings yet
- Health and Healing in Colonial America - EditedDocument5 pagesHealth and Healing in Colonial America - EditedBrian KipkoechNo ratings yet
- Flagellates LabDocument4 pagesFlagellates LabWilliam RamirezNo ratings yet
- Developing My Bleeding Disorders Community Mybdc A Community-Powered Registry To Provide A 360-View of Living With A Bleeding DisorderDocument23 pagesDeveloping My Bleeding Disorders Community Mybdc A Community-Powered Registry To Provide A 360-View of Living With A Bleeding Disorderkalinayak.prasadNo ratings yet
- M14 CT Acupuncture and Traditional Chinese MedicineDocument19 pagesM14 CT Acupuncture and Traditional Chinese MedicinenerdmojoNo ratings yet
- MetamizoleDocument1 pageMetamizoleOliviaNo ratings yet
- Chapter - 2 Microorganisms (Continuation)Document2 pagesChapter - 2 Microorganisms (Continuation)ARSHAD JAMILNo ratings yet
- R01 Revitalife Drip Protocol - UPDATED 9-19-2018Document10 pagesR01 Revitalife Drip Protocol - UPDATED 9-19-2018Eking InNo ratings yet
- COVID Is The-Virus-That-Does-Not-ExistDocument41 pagesCOVID Is The-Virus-That-Does-Not-ExistHansley Templeton Cook100% (2)
- Concept Map Dengue FeverDocument2 pagesConcept Map Dengue FeverChelsyann FerolinoNo ratings yet
- Pediatric OSCE Pictures: For UndergraduatesDocument70 pagesPediatric OSCE Pictures: For UndergraduatesShehab MhmdNo ratings yet
- Nursing Worksheet Template 1 1Document2 pagesNursing Worksheet Template 1 1api-651287771No ratings yet
- Dr. Muslim N. Saeed Family & Community Medicine Dept. March 14, 2022Document10 pagesDr. Muslim N. Saeed Family & Community Medicine Dept. March 14, 2022hussain AltaherNo ratings yet
- Role and Potential of Modern Ultrasound in Pediatric Abdominal ImagingDocument18 pagesRole and Potential of Modern Ultrasound in Pediatric Abdominal ImagingRafael CamachoNo ratings yet
- Types of MeningitisDocument6 pagesTypes of MeningitisARISNo ratings yet
- Midterm Psych NSG Nclex Test BanksDocument19 pagesMidterm Psych NSG Nclex Test BanksAliza AlyyNo ratings yet
- Management of Common Respiratory Infections in Children in IndiaDocument60 pagesManagement of Common Respiratory Infections in Children in IndiaSukumar SubuNo ratings yet
- Diverticular Disease A Review On Pathophysiology and Recent EvidenceDocument6 pagesDiverticular Disease A Review On Pathophysiology and Recent EvidenceIsabella María GantivarNo ratings yet
- DRUG STUDY OmeprazoleDocument3 pagesDRUG STUDY OmeprazoleCelline Isabelle ReyesNo ratings yet
- Fernandez Doctor - Goya's Mental Illness 1994Document6 pagesFernandez Doctor - Goya's Mental Illness 1994FranciscoNo ratings yet
- EnglishDocument5 pagesEnglishMarthe KateNo ratings yet
- History Taking & MSEDocument25 pagesHistory Taking & MSEMahmoud SalehNo ratings yet