
ACR TI-RADS in A Nutshell: A Case Report
ACR TI-RADS in A Nutshell: A Case Report
You might also like
- JECFA Monograph 13Document114 pagesJECFA Monograph 13Azucena Alcántara0% (1)
- Char Dham - The Four Holy AbodesDocument19 pagesChar Dham - The Four Holy AbodesNaresh RathorNo ratings yet
- Weekly AssignmentDocument7 pagesWeekly AssignmentBajwa AyeshaNo ratings yet
- AME 204 Spring 2012 Midterm Exam I SolutionDocument6 pagesAME 204 Spring 2012 Midterm Exam I SolutionJack ZhaoNo ratings yet
- Male Reproductive SystemDocument26 pagesMale Reproductive SystemEmmanuelNo ratings yet
- Analysis of Road Traffic CrashDocument75 pagesAnalysis of Road Traffic CrashBrain Yilson EliasNo ratings yet
- Bullying and CiberbullyingDocument9 pagesBullying and CiberbullyingDyNo ratings yet
- Preparedness of Provincial Jails in Handling PDL's Exhibiting Mental Incapacity A Policy PaperDocument8 pagesPreparedness of Provincial Jails in Handling PDL's Exhibiting Mental Incapacity A Policy PaperInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sampel For Ty Bcom 2021Document18 pagesSampel For Ty Bcom 2021Vidhi ChoithaniNo ratings yet
- 08 TheThrustingChannelDocument8 pages08 TheThrustingChannelwerottydesluizNo ratings yet
- RT 204 Midterm Transes (Updated)Document11 pagesRT 204 Midterm Transes (Updated)LouiseNo ratings yet
- Advantage of Modified MRI Protocol For HDocument148 pagesAdvantage of Modified MRI Protocol For HasasakopNo ratings yet
- Auriol IAN 331144 Alarm ClockDocument43 pagesAuriol IAN 331144 Alarm ClockAdela AmbrosimovNo ratings yet
- IDirect SanseraEngg StockTalesDocument13 pagesIDirect SanseraEngg StockTalesbradburywillsNo ratings yet
- IMO2 Theory SolutionsDocument22 pagesIMO2 Theory SolutionsPhạm Trung Quốc AnhNo ratings yet
- ConflictBarometer 2016Document208 pagesConflictBarometer 2016yawarmiNo ratings yet
- SB 639Document6 pagesSB 639FOX8No ratings yet
- Smart Anchor Catalogue Cum Pricelist Final LowresDocument25 pagesSmart Anchor Catalogue Cum Pricelist Final LowresRanveer LatiyalNo ratings yet
- Nylon Carpet. Harrington Catalogue.2022Document41 pagesNylon Carpet. Harrington Catalogue.2022Nikhil Chawla100% (1)
- Paper 8699Document13 pagesPaper 8699IJARSCT JournalNo ratings yet
- Youth Risk Behavior Survey 2021-22Document50 pagesYouth Risk Behavior Survey 2021-22Colleen FarrellNo ratings yet
- DR Mohamed Hadinata Roslan MSCOst Final Thesis - Submission - BackupDocument75 pagesDR Mohamed Hadinata Roslan MSCOst Final Thesis - Submission - BackupHadinata RoslanNo ratings yet
- The Story of Earth An Observational Guide 1627402930Document336 pagesThe Story of Earth An Observational Guide 1627402930ManquecotiaNo ratings yet
- Happiness Slipping Away Unhappy IndiaDocument6 pagesHappiness Slipping Away Unhappy IndiaEditor IJTSRDNo ratings yet
- Experiment No: 02 Experiment Name:: Identification of Dyestuff From Unknown Dyed Sample (Direct Dye)Document3 pagesExperiment No: 02 Experiment Name:: Identification of Dyestuff From Unknown Dyed Sample (Direct Dye)Md. Sazzadul IslamNo ratings yet
- Anatomy of The Male Reproductive SystemDocument17 pagesAnatomy of The Male Reproductive SystemFarhan haiderNo ratings yet
- CH 9 Solution PDFDocument10 pagesCH 9 Solution PDFAndreas ChristoforouNo ratings yet
- Fisa Histologie 2019 2020 MG ENGL Sem IDocument7 pagesFisa Histologie 2019 2020 MG ENGL Sem IUrsu GeorgianaNo ratings yet
- Ceftazidime+Avibactum-2gm +0.5gm InjectionDocument10 pagesCeftazidime+Avibactum-2gm +0.5gm InjectionMd. Abdur RahmanNo ratings yet
- Evsjv 'K M Ru: Iwr÷Vw© Bs WW G-1Document71 pagesEvsjv 'K M Ru: Iwr÷Vw© Bs WW G-1IQBALNo ratings yet
- Namma Kalvi 5th Tamil Ganga Guide Term 1 218604Document90 pagesNamma Kalvi 5th Tamil Ganga Guide Term 1 218604x a m xNo ratings yet
- Sabarre - BSP2G - Module 4 Lesson 2 Check in ActivityDocument10 pagesSabarre - BSP2G - Module 4 Lesson 2 Check in ActivityArwenNo ratings yet
- A Review Paper On Textile Fiber IdentificationDocument11 pagesA Review Paper On Textile Fiber IdentificationMD.MAHABUB ALOM REFAETNo ratings yet
- S. No Questions AnswerDocument1 pageS. No Questions AnswerSourav PilaniaNo ratings yet
- VMS 201 - F51Document4 pagesVMS 201 - F51이연지No ratings yet
- ملصقات السلامة اصدار المؤسسة العامة للتأمينات الاجتماعيةDocument5 pagesملصقات السلامة اصدار المؤسسة العامة للتأمينات الاجتماعيةAshraf EL WardajiNo ratings yet
- POS-Private Car Package Policy: Certificate of Insurance Cum Policy ScheduleDocument3 pagesPOS-Private Car Package Policy: Certificate of Insurance Cum Policy ScheduleBhavya chandraNo ratings yet
- Sagittal Craniosynostosis: Cognitive Development, Behaviour, and Quality of Life in Unoperated ChildrenDocument9 pagesSagittal Craniosynostosis: Cognitive Development, Behaviour, and Quality of Life in Unoperated ChildrenRetno AmbarwatiNo ratings yet
- SampoornSuraksha SchemeDetails14102022190Document1 pageSampoornSuraksha SchemeDetails14102022190Murthy NandulaNo ratings yet
- 2021 Nep - DohDocument44 pages2021 Nep - DohAngel BacaniNo ratings yet
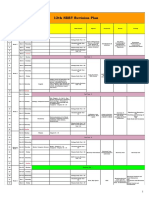
- 12 NEET Revision PlanDocument2 pages12 NEET Revision Planrohith kannanNo ratings yet
- 2023 02 01EatingWellAntioxidantsDocument100 pages2023 02 01EatingWellAntioxidantsCRISTINA ENENo ratings yet
- Cleartrip Flight E-TicketDocument1 pageCleartrip Flight E-TicketpawanNo ratings yet
- C Ovid 19 Treatment GuidelinesDocument356 pagesC Ovid 19 Treatment GuidelinesSebastian LozanoNo ratings yet
- 2021 Medical Catalog-Nanjing Ocean Medical Products Co.,LtdDocument28 pages2021 Medical Catalog-Nanjing Ocean Medical Products Co.,LtdWang BandasackNo ratings yet
- 2016 Autonomy (4+)Document121 pages2016 Autonomy (4+)Rui FélixNo ratings yet
- National Economics UniversityDocument98 pagesNational Economics UniversityNguyễn Hương QuỳnhNo ratings yet
- Economy MIB 2023Document58 pagesEconomy MIB 2023Jas SinNo ratings yet
- Chapter 2 UNIT 1Document19 pagesChapter 2 UNIT 1Ayen LatosaNo ratings yet
- Corporate GovernanceDocument22 pagesCorporate GovernanceBenita BijuNo ratings yet
- Overboss FAQ v8Document4 pagesOverboss FAQ v8Jonatan Ávila CavaNo ratings yet
- NutritionDocument2 pagesNutritionVishu MehtaNo ratings yet
- Chapter 1 Data InterpretationDocument22 pagesChapter 1 Data InterpretationRodrigo100% (1)
- July 2022Document68 pagesJuly 2022DASARI MADHUSUDHANNo ratings yet
- AyuCaRe Vol 1 Issue 1Document52 pagesAyuCaRe Vol 1 Issue 1Priyanka SharmaNo ratings yet
- PHARMA 2 Sir RafDocument1 pagePHARMA 2 Sir Rafshirlenedel cariñoNo ratings yet
- ChandramukhiDocument6 pagesChandramukhiMaple IncNo ratings yet
- 2005 - Us6979776 - Pipe Bundle For Underground InstallationDocument17 pages2005 - Us6979776 - Pipe Bundle For Underground InstallationCường Nguyễn QuốcNo ratings yet
- Exide Life Smart Term EdgeDocument22 pagesExide Life Smart Term EdgeDinesh BokadeNo ratings yet
- Pemeriksaan Penunjang Onkologi Pada MataDocument29 pagesPemeriksaan Penunjang Onkologi Pada MatamazidahzulfaNo ratings yet



























































Download as pdf or txt
You might also like
- JECFA Monograph 13Document114 pagesJECFA Monograph 13Azucena Alcántara0% (1)
- Char Dham - The Four Holy AbodesDocument19 pagesChar Dham - The Four Holy AbodesNaresh RathorNo ratings yet
- Weekly AssignmentDocument7 pagesWeekly AssignmentBajwa AyeshaNo ratings yet
- AME 204 Spring 2012 Midterm Exam I SolutionDocument6 pagesAME 204 Spring 2012 Midterm Exam I SolutionJack ZhaoNo ratings yet
- Male Reproductive SystemDocument26 pagesMale Reproductive SystemEmmanuelNo ratings yet
- Analysis of Road Traffic CrashDocument75 pagesAnalysis of Road Traffic CrashBrain Yilson EliasNo ratings yet
- Bullying and CiberbullyingDocument9 pagesBullying and CiberbullyingDyNo ratings yet
- Preparedness of Provincial Jails in Handling PDL's Exhibiting Mental Incapacity A Policy PaperDocument8 pagesPreparedness of Provincial Jails in Handling PDL's Exhibiting Mental Incapacity A Policy PaperInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sampel For Ty Bcom 2021Document18 pagesSampel For Ty Bcom 2021Vidhi ChoithaniNo ratings yet
- 08 TheThrustingChannelDocument8 pages08 TheThrustingChannelwerottydesluizNo ratings yet
- RT 204 Midterm Transes (Updated)Document11 pagesRT 204 Midterm Transes (Updated)LouiseNo ratings yet
- Advantage of Modified MRI Protocol For HDocument148 pagesAdvantage of Modified MRI Protocol For HasasakopNo ratings yet
- Auriol IAN 331144 Alarm ClockDocument43 pagesAuriol IAN 331144 Alarm ClockAdela AmbrosimovNo ratings yet
- IDirect SanseraEngg StockTalesDocument13 pagesIDirect SanseraEngg StockTalesbradburywillsNo ratings yet
- IMO2 Theory SolutionsDocument22 pagesIMO2 Theory SolutionsPhạm Trung Quốc AnhNo ratings yet
- ConflictBarometer 2016Document208 pagesConflictBarometer 2016yawarmiNo ratings yet
- SB 639Document6 pagesSB 639FOX8No ratings yet
- Smart Anchor Catalogue Cum Pricelist Final LowresDocument25 pagesSmart Anchor Catalogue Cum Pricelist Final LowresRanveer LatiyalNo ratings yet
- Nylon Carpet. Harrington Catalogue.2022Document41 pagesNylon Carpet. Harrington Catalogue.2022Nikhil Chawla100% (1)
- Paper 8699Document13 pagesPaper 8699IJARSCT JournalNo ratings yet
- Youth Risk Behavior Survey 2021-22Document50 pagesYouth Risk Behavior Survey 2021-22Colleen FarrellNo ratings yet
- DR Mohamed Hadinata Roslan MSCOst Final Thesis - Submission - BackupDocument75 pagesDR Mohamed Hadinata Roslan MSCOst Final Thesis - Submission - BackupHadinata RoslanNo ratings yet
- The Story of Earth An Observational Guide 1627402930Document336 pagesThe Story of Earth An Observational Guide 1627402930ManquecotiaNo ratings yet
- Happiness Slipping Away Unhappy IndiaDocument6 pagesHappiness Slipping Away Unhappy IndiaEditor IJTSRDNo ratings yet
- Experiment No: 02 Experiment Name:: Identification of Dyestuff From Unknown Dyed Sample (Direct Dye)Document3 pagesExperiment No: 02 Experiment Name:: Identification of Dyestuff From Unknown Dyed Sample (Direct Dye)Md. Sazzadul IslamNo ratings yet
- Anatomy of The Male Reproductive SystemDocument17 pagesAnatomy of The Male Reproductive SystemFarhan haiderNo ratings yet
- CH 9 Solution PDFDocument10 pagesCH 9 Solution PDFAndreas ChristoforouNo ratings yet
- Fisa Histologie 2019 2020 MG ENGL Sem IDocument7 pagesFisa Histologie 2019 2020 MG ENGL Sem IUrsu GeorgianaNo ratings yet
- Ceftazidime+Avibactum-2gm +0.5gm InjectionDocument10 pagesCeftazidime+Avibactum-2gm +0.5gm InjectionMd. Abdur RahmanNo ratings yet
- Evsjv 'K M Ru: Iwr÷Vw© Bs WW G-1Document71 pagesEvsjv 'K M Ru: Iwr÷Vw© Bs WW G-1IQBALNo ratings yet
- Namma Kalvi 5th Tamil Ganga Guide Term 1 218604Document90 pagesNamma Kalvi 5th Tamil Ganga Guide Term 1 218604x a m xNo ratings yet
- Sabarre - BSP2G - Module 4 Lesson 2 Check in ActivityDocument10 pagesSabarre - BSP2G - Module 4 Lesson 2 Check in ActivityArwenNo ratings yet
- A Review Paper On Textile Fiber IdentificationDocument11 pagesA Review Paper On Textile Fiber IdentificationMD.MAHABUB ALOM REFAETNo ratings yet
- S. No Questions AnswerDocument1 pageS. No Questions AnswerSourav PilaniaNo ratings yet
- VMS 201 - F51Document4 pagesVMS 201 - F51이연지No ratings yet
- ملصقات السلامة اصدار المؤسسة العامة للتأمينات الاجتماعيةDocument5 pagesملصقات السلامة اصدار المؤسسة العامة للتأمينات الاجتماعيةAshraf EL WardajiNo ratings yet
- POS-Private Car Package Policy: Certificate of Insurance Cum Policy ScheduleDocument3 pagesPOS-Private Car Package Policy: Certificate of Insurance Cum Policy ScheduleBhavya chandraNo ratings yet
- Sagittal Craniosynostosis: Cognitive Development, Behaviour, and Quality of Life in Unoperated ChildrenDocument9 pagesSagittal Craniosynostosis: Cognitive Development, Behaviour, and Quality of Life in Unoperated ChildrenRetno AmbarwatiNo ratings yet
- SampoornSuraksha SchemeDetails14102022190Document1 pageSampoornSuraksha SchemeDetails14102022190Murthy NandulaNo ratings yet
- 2021 Nep - DohDocument44 pages2021 Nep - DohAngel BacaniNo ratings yet
- 12 NEET Revision PlanDocument2 pages12 NEET Revision Planrohith kannanNo ratings yet
- 2023 02 01EatingWellAntioxidantsDocument100 pages2023 02 01EatingWellAntioxidantsCRISTINA ENENo ratings yet
- Cleartrip Flight E-TicketDocument1 pageCleartrip Flight E-TicketpawanNo ratings yet
- C Ovid 19 Treatment GuidelinesDocument356 pagesC Ovid 19 Treatment GuidelinesSebastian LozanoNo ratings yet
- 2021 Medical Catalog-Nanjing Ocean Medical Products Co.,LtdDocument28 pages2021 Medical Catalog-Nanjing Ocean Medical Products Co.,LtdWang BandasackNo ratings yet
- 2016 Autonomy (4+)Document121 pages2016 Autonomy (4+)Rui FélixNo ratings yet
- National Economics UniversityDocument98 pagesNational Economics UniversityNguyễn Hương QuỳnhNo ratings yet
- Economy MIB 2023Document58 pagesEconomy MIB 2023Jas SinNo ratings yet
- Chapter 2 UNIT 1Document19 pagesChapter 2 UNIT 1Ayen LatosaNo ratings yet
- Corporate GovernanceDocument22 pagesCorporate GovernanceBenita BijuNo ratings yet
- Overboss FAQ v8Document4 pagesOverboss FAQ v8Jonatan Ávila CavaNo ratings yet
- NutritionDocument2 pagesNutritionVishu MehtaNo ratings yet
- Chapter 1 Data InterpretationDocument22 pagesChapter 1 Data InterpretationRodrigo100% (1)
- July 2022Document68 pagesJuly 2022DASARI MADHUSUDHANNo ratings yet
- AyuCaRe Vol 1 Issue 1Document52 pagesAyuCaRe Vol 1 Issue 1Priyanka SharmaNo ratings yet
- PHARMA 2 Sir RafDocument1 pagePHARMA 2 Sir Rafshirlenedel cariñoNo ratings yet
- ChandramukhiDocument6 pagesChandramukhiMaple IncNo ratings yet
- 2005 - Us6979776 - Pipe Bundle For Underground InstallationDocument17 pages2005 - Us6979776 - Pipe Bundle For Underground InstallationCường Nguyễn QuốcNo ratings yet
- Exide Life Smart Term EdgeDocument22 pagesExide Life Smart Term EdgeDinesh BokadeNo ratings yet
- Pemeriksaan Penunjang Onkologi Pada MataDocument29 pagesPemeriksaan Penunjang Onkologi Pada MatamazidahzulfaNo ratings yet