
Adobe Scan 07 May 2023 PDF
Adobe Scan 07 May 2023 PDF
You might also like
- Expanded Dengue Syndrome: Zukmianty SuaibDocument45 pagesExpanded Dengue Syndrome: Zukmianty SuaibclaraNo ratings yet
- Teks MC For English WeekDocument2 pagesTeks MC For English WeekYoNz AliaTi89% (19)
- Tugas Akhir Bedah Saraf Akhir 11-18 Maret 2019Document16 pagesTugas Akhir Bedah Saraf Akhir 11-18 Maret 2019Rinna'Cannabis Extremebalanceputih Part IINo ratings yet
- Mapping Aqsha 3 Senin, 14 Maret 2022Document3 pagesMapping Aqsha 3 Senin, 14 Maret 2022Satrya DitaNo ratings yet
- Pedia NotesDocument4 pagesPedia NotesDana CastroNo ratings yet
- Jepretan Layar 2021-01-27 Pada 21.01.47Document13 pagesJepretan Layar 2021-01-27 Pada 21.01.47nadyaNo ratings yet
- Date 02/jun/2023 09:05AM 20/mar/23 10:15AM 12/jan/23 02:47PM 12/nov/22 08:55AM 15/jul/21 02:18PM Unit Bio Ref IntervalDocument9 pagesDate 02/jun/2023 09:05AM 20/mar/23 10:15AM 12/jan/23 02:47PM 12/nov/22 08:55AM 15/jul/21 02:18PM Unit Bio Ref IntervalRemit DadhwalNo ratings yet
- Bo PrathibaDocument4 pagesBo PrathibaKunal GowdaNo ratings yet
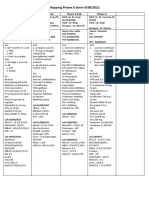
- Mapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Document2 pagesMapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Rina SyafritaNo ratings yet
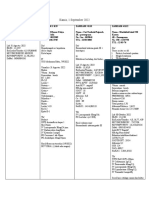
- Maping Pinere 1, Jum'at 24 September 2021: TH THDocument2 pagesMaping Pinere 1, Jum'at 24 September 2021: TH THRina SyafritaNo ratings yet
- Revisi Askep DMDocument29 pagesRevisi Askep DMSyerliNo ratings yet
- Bo KoteappaDocument3 pagesBo KoteappaDr. D RNo ratings yet
- Case PresentationDocument40 pagesCase PresentationLaxman Lucky'sNo ratings yet
- Comments: S27 - Sonwar (Srinagar) CCDocument3 pagesComments: S27 - Sonwar (Srinagar) CCPervaz AhmadNo ratings yet
- DC ReskiDocument27 pagesDC ReskiHardiyanti HermanNo ratings yet
- Laporan Jaga Perina Selasa Malam EditDocument15 pagesLaporan Jaga Perina Selasa Malam EditmuhammadrikiNo ratings yet
- CBD Madya GastroDocument38 pagesCBD Madya GastroNurina yupiNo ratings yet
- Drug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingDocument12 pagesDrug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingBhoomika PandeyNo ratings yet
- Concept MapDocument15 pagesConcept Mapapi-495456666No ratings yet
- Morning Report Sunday Morning, March 8th 2020: Syt/Slr/Sth/SwiDocument25 pagesMorning Report Sunday Morning, March 8th 2020: Syt/Slr/Sth/SwimuhammadrikiNo ratings yet
- CC 2 Okt Hcu NeoDocument26 pagesCC 2 Okt Hcu NeolatifahNo ratings yet
- Complex Care Concept MapDocument11 pagesComplex Care Concept Mapapi-662433822No ratings yet
- Aqsha 2 (Penyakit Dalam Pria) Hari / Tanggal: Sabtu, 12 Oktober 2019 Dokter Jaga: Dr. Hans/ Dr. Muchsin Dokter Muda: Asti/LisaDocument7 pagesAqsha 2 (Penyakit Dalam Pria) Hari / Tanggal: Sabtu, 12 Oktober 2019 Dokter Jaga: Dr. Hans/ Dr. Muchsin Dokter Muda: Asti/LisaAsti Sauna MentariNo ratings yet
- Sept 4, 2015Document8 pagesSept 4, 2015Deity CelleNo ratings yet
- Hayu 7Document20 pagesHayu 7abdimoh926No ratings yet
- A Case Report On Multisystemic Inflammatory Syndrome - Children How The Diagnosis and Treatment Could Be ChallengingDocument5 pagesA Case Report On Multisystemic Inflammatory Syndrome - Children How The Diagnosis and Treatment Could Be ChallengingIJAR JOURNALNo ratings yet
- Surgery PortDocument5 pagesSurgery Portabenezer g/kirstosNo ratings yet
- Mappimg Kamar 1 Dan 5Document4 pagesMappimg Kamar 1 Dan 5Satrya DitaNo ratings yet
- DM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S VenkataseshanDocument50 pagesDM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S Venkataseshanvishal sidanaNo ratings yet
- Mortality U5 MDocument17 pagesMortality U5 MAvian CamelotNo ratings yet
- Emergency Room Record: Doctor'S Order SheetDocument10 pagesEmergency Room Record: Doctor'S Order SheetAngelo MadjosNo ratings yet
- April 2017Document21 pagesApril 2017drpinnakavamsiNo ratings yet
- MR Nuryatim FixDocument12 pagesMR Nuryatim FixtiarapolarisiriuzNo ratings yet
- Ana Case Study Copy 2Document25 pagesAna Case Study Copy 2AmirNo ratings yet
- Uk007 2223 006609Document3 pagesUk007 2223 006609Arpit KumarNo ratings yet
- RTRH Med AbstractDocument2 pagesRTRH Med Abstractsunako nakaharaNo ratings yet
- Case 6Document7 pagesCase 6Angel MayNo ratings yet
- Rahmatia Efusi PleuraDocument14 pagesRahmatia Efusi PleuraJuli2022 Semnol-SemsaNo ratings yet
- Morbidity Meeting CT Icu (1) (1) - 2 3Document33 pagesMorbidity Meeting CT Icu (1) (1) - 2 3evaNo ratings yet
- Discharge Summary Patient's ProfilesDocument5 pagesDischarge Summary Patient's ProfilesAnonymous nSGpLONo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- Clinical Conference 21 August 2022: Eria (New Case)Document16 pagesClinical Conference 21 August 2022: Eria (New Case)mujahidah nursinNo ratings yet
- Ward Report 6th August BQDocument7 pagesWard Report 6th August BQAfkar30No ratings yet
- AQSA 3 - Senin 19 Juli 2021Document12 pagesAQSA 3 - Senin 19 Juli 2021Dezha DetiroNo ratings yet
- Parade Fiona - 11-07-22 (2) OlnDocument32 pagesParade Fiona - 11-07-22 (2) OlndarafujiNo ratings yet
- Coass: 1. Firman 2. Lambert 3. Komang 4. Liliana 5. Desy: Consultant: Dr. Tommy, SP - BSDocument9 pagesCoass: 1. Firman 2. Lambert 3. Komang 4. Liliana 5. Desy: Consultant: Dr. Tommy, SP - BSLily HestiNo ratings yet
- Teleconference 12 Maret 2019 FixDocument9 pagesTeleconference 12 Maret 2019 Fixchrisvivani ruatakureiNo ratings yet
- MAPPINGDocument2 pagesMAPPINGPratiwi ARHNo ratings yet
- AQSHA 2, 15 Juli '19Document6 pagesAQSHA 2, 15 Juli '19Hiya Ulfi MuniraNo ratings yet
- Mapping DR Irma 10-12-2022Document1 pageMapping DR Irma 10-12-2022nina purnamasariNo ratings yet
- Case Study Neonatal SepsisDocument22 pagesCase Study Neonatal Sepsisaishah shamsudinNo ratings yet
- Meningitis AND Marasmus: Presented By: Clarisa Monica Widya MargaretDocument41 pagesMeningitis AND Marasmus: Presented By: Clarisa Monica Widya MargaretwidyamsNo ratings yet
- Case Study For OligohydramniosDocument8 pagesCase Study For OligohydramniosKinjal Vasava100% (1)
- Mapping GEH 1 9 22Document3 pagesMapping GEH 1 9 22naufalNo ratings yet
- OK Cito Jaga Pagi 13 Oktober 2023Document7 pagesOK Cito Jaga Pagi 13 Oktober 2023rezaanestesiasusantoNo ratings yet
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- JEJARING DR - Rahma, DR - Dewi, DR - Herry 10-10-2021Document1 pageJEJARING DR - Rahma, DR - Dewi, DR - Herry 10-10-2021nina purnamasariNo ratings yet
- Severe Plasmodium Falciparum Malaria Complicated by Acute Myocarditis (Case Report)Document4 pagesSevere Plasmodium Falciparum Malaria Complicated by Acute Myocarditis (Case Report)IJAR JOURNALNo ratings yet
- Case StudyDocument46 pagesCase StudysarikaNo ratings yet
- Mapping New Aqsa 3 Sabtu 23 Oktober 2021Document6 pagesMapping New Aqsa 3 Sabtu 23 Oktober 2021Muhammed GhaziNo ratings yet
- Alternative Assessment - Conference N InterviewsDocument11 pagesAlternative Assessment - Conference N InterviewsWan Nur AmalinaNo ratings yet
- Item AnalysisDocument3 pagesItem AnalysisWan Nur AmalinaNo ratings yet
- Number 6Document2 pagesNumber 6Wan Nur AmalinaNo ratings yet
- Questionnaire Draft Mytnb Version 9Document11 pagesQuestionnaire Draft Mytnb Version 9Wan Nur AmalinaNo ratings yet
- Abg PunyaaaaaDocument1 pageAbg PunyaaaaaWan Nur AmalinaNo ratings yet
- Cefr Course Lesson Plan SpeakingDocument2 pagesCefr Course Lesson Plan SpeakingWan Nur AmalinaNo ratings yet
- Coaching ProgramDocument1 pageCoaching ProgramWan Nur AmalinaNo ratings yet
































































Download as pdf or txt
You might also like
- Expanded Dengue Syndrome: Zukmianty SuaibDocument45 pagesExpanded Dengue Syndrome: Zukmianty SuaibclaraNo ratings yet
- Teks MC For English WeekDocument2 pagesTeks MC For English WeekYoNz AliaTi89% (19)
- Tugas Akhir Bedah Saraf Akhir 11-18 Maret 2019Document16 pagesTugas Akhir Bedah Saraf Akhir 11-18 Maret 2019Rinna'Cannabis Extremebalanceputih Part IINo ratings yet
- Mapping Aqsha 3 Senin, 14 Maret 2022Document3 pagesMapping Aqsha 3 Senin, 14 Maret 2022Satrya DitaNo ratings yet
- Pedia NotesDocument4 pagesPedia NotesDana CastroNo ratings yet
- Jepretan Layar 2021-01-27 Pada 21.01.47Document13 pagesJepretan Layar 2021-01-27 Pada 21.01.47nadyaNo ratings yet
- Date 02/jun/2023 09:05AM 20/mar/23 10:15AM 12/jan/23 02:47PM 12/nov/22 08:55AM 15/jul/21 02:18PM Unit Bio Ref IntervalDocument9 pagesDate 02/jun/2023 09:05AM 20/mar/23 10:15AM 12/jan/23 02:47PM 12/nov/22 08:55AM 15/jul/21 02:18PM Unit Bio Ref IntervalRemit DadhwalNo ratings yet
- Bo PrathibaDocument4 pagesBo PrathibaKunal GowdaNo ratings yet
- Mapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Document2 pagesMapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Rina SyafritaNo ratings yet
- Maping Pinere 1, Jum'at 24 September 2021: TH THDocument2 pagesMaping Pinere 1, Jum'at 24 September 2021: TH THRina SyafritaNo ratings yet
- Revisi Askep DMDocument29 pagesRevisi Askep DMSyerliNo ratings yet
- Bo KoteappaDocument3 pagesBo KoteappaDr. D RNo ratings yet
- Case PresentationDocument40 pagesCase PresentationLaxman Lucky'sNo ratings yet
- Comments: S27 - Sonwar (Srinagar) CCDocument3 pagesComments: S27 - Sonwar (Srinagar) CCPervaz AhmadNo ratings yet
- DC ReskiDocument27 pagesDC ReskiHardiyanti HermanNo ratings yet
- Laporan Jaga Perina Selasa Malam EditDocument15 pagesLaporan Jaga Perina Selasa Malam EditmuhammadrikiNo ratings yet
- CBD Madya GastroDocument38 pagesCBD Madya GastroNurina yupiNo ratings yet
- Drug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingDocument12 pagesDrug Presentation ON Inj. Teicoplanin: St. Stephen'S Hospital College of NursingBhoomika PandeyNo ratings yet
- Concept MapDocument15 pagesConcept Mapapi-495456666No ratings yet
- Morning Report Sunday Morning, March 8th 2020: Syt/Slr/Sth/SwiDocument25 pagesMorning Report Sunday Morning, March 8th 2020: Syt/Slr/Sth/SwimuhammadrikiNo ratings yet
- CC 2 Okt Hcu NeoDocument26 pagesCC 2 Okt Hcu NeolatifahNo ratings yet
- Complex Care Concept MapDocument11 pagesComplex Care Concept Mapapi-662433822No ratings yet
- Aqsha 2 (Penyakit Dalam Pria) Hari / Tanggal: Sabtu, 12 Oktober 2019 Dokter Jaga: Dr. Hans/ Dr. Muchsin Dokter Muda: Asti/LisaDocument7 pagesAqsha 2 (Penyakit Dalam Pria) Hari / Tanggal: Sabtu, 12 Oktober 2019 Dokter Jaga: Dr. Hans/ Dr. Muchsin Dokter Muda: Asti/LisaAsti Sauna MentariNo ratings yet
- Sept 4, 2015Document8 pagesSept 4, 2015Deity CelleNo ratings yet
- Hayu 7Document20 pagesHayu 7abdimoh926No ratings yet
- A Case Report On Multisystemic Inflammatory Syndrome - Children How The Diagnosis and Treatment Could Be ChallengingDocument5 pagesA Case Report On Multisystemic Inflammatory Syndrome - Children How The Diagnosis and Treatment Could Be ChallengingIJAR JOURNALNo ratings yet
- Surgery PortDocument5 pagesSurgery Portabenezer g/kirstosNo ratings yet
- Mappimg Kamar 1 Dan 5Document4 pagesMappimg Kamar 1 Dan 5Satrya DitaNo ratings yet
- DM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S VenkataseshanDocument50 pagesDM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S Venkataseshanvishal sidanaNo ratings yet
- Mortality U5 MDocument17 pagesMortality U5 MAvian CamelotNo ratings yet
- Emergency Room Record: Doctor'S Order SheetDocument10 pagesEmergency Room Record: Doctor'S Order SheetAngelo MadjosNo ratings yet
- April 2017Document21 pagesApril 2017drpinnakavamsiNo ratings yet
- MR Nuryatim FixDocument12 pagesMR Nuryatim FixtiarapolarisiriuzNo ratings yet
- Ana Case Study Copy 2Document25 pagesAna Case Study Copy 2AmirNo ratings yet
- Uk007 2223 006609Document3 pagesUk007 2223 006609Arpit KumarNo ratings yet
- RTRH Med AbstractDocument2 pagesRTRH Med Abstractsunako nakaharaNo ratings yet
- Case 6Document7 pagesCase 6Angel MayNo ratings yet
- Rahmatia Efusi PleuraDocument14 pagesRahmatia Efusi PleuraJuli2022 Semnol-SemsaNo ratings yet
- Morbidity Meeting CT Icu (1) (1) - 2 3Document33 pagesMorbidity Meeting CT Icu (1) (1) - 2 3evaNo ratings yet
- Discharge Summary Patient's ProfilesDocument5 pagesDischarge Summary Patient's ProfilesAnonymous nSGpLONo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- Clinical Conference 21 August 2022: Eria (New Case)Document16 pagesClinical Conference 21 August 2022: Eria (New Case)mujahidah nursinNo ratings yet
- Ward Report 6th August BQDocument7 pagesWard Report 6th August BQAfkar30No ratings yet
- AQSA 3 - Senin 19 Juli 2021Document12 pagesAQSA 3 - Senin 19 Juli 2021Dezha DetiroNo ratings yet
- Parade Fiona - 11-07-22 (2) OlnDocument32 pagesParade Fiona - 11-07-22 (2) OlndarafujiNo ratings yet
- Coass: 1. Firman 2. Lambert 3. Komang 4. Liliana 5. Desy: Consultant: Dr. Tommy, SP - BSDocument9 pagesCoass: 1. Firman 2. Lambert 3. Komang 4. Liliana 5. Desy: Consultant: Dr. Tommy, SP - BSLily HestiNo ratings yet
- Teleconference 12 Maret 2019 FixDocument9 pagesTeleconference 12 Maret 2019 Fixchrisvivani ruatakureiNo ratings yet
- MAPPINGDocument2 pagesMAPPINGPratiwi ARHNo ratings yet
- AQSHA 2, 15 Juli '19Document6 pagesAQSHA 2, 15 Juli '19Hiya Ulfi MuniraNo ratings yet
- Mapping DR Irma 10-12-2022Document1 pageMapping DR Irma 10-12-2022nina purnamasariNo ratings yet
- Case Study Neonatal SepsisDocument22 pagesCase Study Neonatal Sepsisaishah shamsudinNo ratings yet
- Meningitis AND Marasmus: Presented By: Clarisa Monica Widya MargaretDocument41 pagesMeningitis AND Marasmus: Presented By: Clarisa Monica Widya MargaretwidyamsNo ratings yet
- Case Study For OligohydramniosDocument8 pagesCase Study For OligohydramniosKinjal Vasava100% (1)
- Mapping GEH 1 9 22Document3 pagesMapping GEH 1 9 22naufalNo ratings yet
- OK Cito Jaga Pagi 13 Oktober 2023Document7 pagesOK Cito Jaga Pagi 13 Oktober 2023rezaanestesiasusantoNo ratings yet
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- JEJARING DR - Rahma, DR - Dewi, DR - Herry 10-10-2021Document1 pageJEJARING DR - Rahma, DR - Dewi, DR - Herry 10-10-2021nina purnamasariNo ratings yet
- Severe Plasmodium Falciparum Malaria Complicated by Acute Myocarditis (Case Report)Document4 pagesSevere Plasmodium Falciparum Malaria Complicated by Acute Myocarditis (Case Report)IJAR JOURNALNo ratings yet
- Case StudyDocument46 pagesCase StudysarikaNo ratings yet
- Mapping New Aqsa 3 Sabtu 23 Oktober 2021Document6 pagesMapping New Aqsa 3 Sabtu 23 Oktober 2021Muhammed GhaziNo ratings yet
- Alternative Assessment - Conference N InterviewsDocument11 pagesAlternative Assessment - Conference N InterviewsWan Nur AmalinaNo ratings yet
- Item AnalysisDocument3 pagesItem AnalysisWan Nur AmalinaNo ratings yet
- Number 6Document2 pagesNumber 6Wan Nur AmalinaNo ratings yet
- Questionnaire Draft Mytnb Version 9Document11 pagesQuestionnaire Draft Mytnb Version 9Wan Nur AmalinaNo ratings yet
- Abg PunyaaaaaDocument1 pageAbg PunyaaaaaWan Nur AmalinaNo ratings yet
- Cefr Course Lesson Plan SpeakingDocument2 pagesCefr Course Lesson Plan SpeakingWan Nur AmalinaNo ratings yet
- Coaching ProgramDocument1 pageCoaching ProgramWan Nur AmalinaNo ratings yet