Download as docx, pdf, or txt
You might also like
- F F F F: Downloaded From Manuals Search EngineDocument2 pagesF F F F: Downloaded From Manuals Search EngineZsolt KántorNo ratings yet
- HysterectomyDocument5 pagesHysterectomysapana shah100% (1)
- HysterectomyDocument3 pagesHysterectomyRobesito Evangelista ArtiagaNo ratings yet
- Hysterectomy: The American College of Obstetricians and GynecologistsDocument0 pagesHysterectomy: The American College of Obstetricians and Gynecologistsmonir61No ratings yet
- Hysterectomy ReportDocument18 pagesHysterectomy ReportMa. Louise Lovely RosalesNo ratings yet
- HysterectomyDocument5 pagesHysterectomyТанзиля Миндубаева МЛ-209No ratings yet
- Tah Bso MinaDocument3 pagesTah Bso MinaANGELA MAY ACILONo ratings yet
- Q. What Are The Most Common Sites of Endometriosis in The Pelvic Area? A. If We Accept The Theory of Retrograde Menstruation As The Main Cause For The InitiationDocument8 pagesQ. What Are The Most Common Sites of Endometriosis in The Pelvic Area? A. If We Accept The Theory of Retrograde Menstruation As The Main Cause For The InitiationAr YanNo ratings yet
- Q. What Are The Most Common Sites of Endometriosis in The Pelvic Area? A. If We Accept The Theory of Retrograde Menstruation As The Main Cause For The InitiationDocument8 pagesQ. What Are The Most Common Sites of Endometriosis in The Pelvic Area? A. If We Accept The Theory of Retrograde Menstruation As The Main Cause For The InitiationAr YanNo ratings yet
- Hysterectomy: Frequently Asked Questions FAQ008 Special ProceduresDocument4 pagesHysterectomy: Frequently Asked Questions FAQ008 Special ProceduresGrace Noviyanthi SinambelaNo ratings yet
- Uterine Leiomyoma and Benign Ovarian Tumors 24.8.2022 PDFDocument48 pagesUterine Leiomyoma and Benign Ovarian Tumors 24.8.2022 PDFZayNo ratings yet
- What Is TAHbsoDocument2 pagesWhat Is TAHbsomiskidd100% (2)
- Uterine Fibroids: The American College of Obstetricians and GynecologistsDocument4 pagesUterine Fibroids: The American College of Obstetricians and GynecologistsarthoclaseNo ratings yet
- Vaginal HysterectomyDocument5 pagesVaginal Hysterectomysensitivity23No ratings yet
- EndometriosisDocument46 pagesEndometriosisManoj Ranadive0% (1)
- Gynecological Surgery - Sundhed - DKDocument19 pagesGynecological Surgery - Sundhed - DKPavel BerlinschiNo ratings yet
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaadNo ratings yet
- Hysterectomy 160819044047Document36 pagesHysterectomy 160819044047Baljeet KaurNo ratings yet
- Gynaecology Surgery PresentationDocument117 pagesGynaecology Surgery Presentationnorhafizahstoh89No ratings yet
- Ectopic Pregancy: Chena B. CurigDocument35 pagesEctopic Pregancy: Chena B. CurigJaicca Faith Tandih AllasNo ratings yet
- Myoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDocument3 pagesMyoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDiane MargretNo ratings yet
- Benign ConditionsDocument40 pagesBenign ConditionsnoreenfatimamaanNo ratings yet
- Perimenopausal Bleeding and Bleeding After Menopause - ACOGDocument9 pagesPerimenopausal Bleeding and Bleeding After Menopause - ACOGShubhra Ray ChaudhuryNo ratings yet
- Cancer of The UterusDocument5 pagesCancer of The UterusShreyas WalvekarNo ratings yet
- Uterine Fibroids: The American College of Obstetricians and GynecologistsDocument4 pagesUterine Fibroids: The American College of Obstetricians and Gynecologistschristiealexa13No ratings yet
- LaparosDocument3 pagesLaparosBartek MarcysiakNo ratings yet
- JocelynPrieto OBGyneDocument7 pagesJocelynPrieto OBGyneAndrew Joever PrietoNo ratings yet
- Advanced Laparoscopic Hysterectomy SurgeryDocument2 pagesAdvanced Laparoscopic Hysterectomy SurgeryManu GynecologyNo ratings yet
- Dysfunctional Uterine Bleeding Lecture DR Gem AshbyDocument45 pagesDysfunctional Uterine Bleeding Lecture DR Gem AshbyPandawa ObgynNo ratings yet
- Hysterectomy: Frequently Asked Questions FAQ008 Special ProceduresDocument4 pagesHysterectomy: Frequently Asked Questions FAQ008 Special ProceduresIlham HalimNo ratings yet
- Common Gynaecological SurgeriesDocument32 pagesCommon Gynaecological Surgeriessmita.shindeNo ratings yet
- HYSTERECTOMYDocument18 pagesHYSTERECTOMYnaga maniNo ratings yet
- Very Large: IndikasiDocument7 pagesVery Large: IndikasiJennifer JaneNo ratings yet
- Uterine Fibroid-IzzatDocument20 pagesUterine Fibroid-IzzatcopperNo ratings yet
- American ObsgynDocument3 pagesAmerican ObsgynSuci RahmiNo ratings yet
- Nital Disorders and Injuries-1Document43 pagesNital Disorders and Injuries-1qruz Mohamed DiisNo ratings yet
- Ovarian CystDocument19 pagesOvarian CystMuhammad AbeeshNo ratings yet
- Cancer of The CervixDocument14 pagesCancer of The CervixJils SureshNo ratings yet
- Case Report External EndometriosisDocument8 pagesCase Report External Endometriosisvvv LllNo ratings yet
- Cervical Cancer: Santos, Maxime Ella L. Gecera, Alondra KateDocument22 pagesCervical Cancer: Santos, Maxime Ella L. Gecera, Alondra KateLyssaMarieKathryneEgeNo ratings yet
- Tubo Ovarian Abcess (Abses Tuba-Ovari)Document4 pagesTubo Ovarian Abcess (Abses Tuba-Ovari)Muhammad Naqiuddin JalaluddinNo ratings yet
- Benign Neoplasms of The Genital 2Document22 pagesBenign Neoplasms of The Genital 2ugonna nwokeNo ratings yet
- HysterectomyDocument2 pagesHysterectomyJellou MacNo ratings yet
- Low 4Document8 pagesLow 4Jennifer JaneNo ratings yet
- Ovarian CystsDocument29 pagesOvarian Cystspal_pal_palNo ratings yet
- Breast CancerDocument4 pagesBreast CancerNyrhtak17No ratings yet
- Presentation1 Cervical BiopsyDocument14 pagesPresentation1 Cervical BiopsyChanta MaharjanNo ratings yet
- Uterine Fibroids: Frequently Asked Questions FAQ074 Gynecologic ProblemsDocument3 pagesUterine Fibroids: Frequently Asked Questions FAQ074 Gynecologic ProblemsrohitNo ratings yet
- Endometriosis O&g PresentationDocument31 pagesEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- Surgical Uterus Gynecologist Fundus Cervix: Types of HysterectomyDocument3 pagesSurgical Uterus Gynecologist Fundus Cervix: Types of HysterectomyMary Ann LunnayNo ratings yet
- Ectopic Pregnancy: Read MoreDocument15 pagesEctopic Pregnancy: Read MoreVanessa Santos100% (1)
- Explo Lap TahbsoDocument3 pagesExplo Lap TahbsoJustin AlejoNo ratings yet
- TAHBSODocument3 pagesTAHBSOakatzkiNo ratings yet
- Romero 1Document3 pagesRomero 1rochelleNo ratings yet
- Hysterectomy - NHSDocument1 pageHysterectomy - NHSSandhya SriramanNo ratings yet
- Patient Information Sheets Aagl AllDocument14 pagesPatient Information Sheets Aagl AllAmbarNo ratings yet
- hysterectomyDocument13 pageshysterectomyMAYURII MANENo ratings yet
- Obstetric HemorrhageDocument74 pagesObstetric HemorrhageAmir KhanNo ratings yet
- SuegeryDocument3 pagesSuegeryCristian VieriuNo ratings yet
- Hysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- 2022 Brochure Drypoint RaDocument12 pages2022 Brochure Drypoint RaMiszael EspinosaNo ratings yet
- Background of The StudyDocument13 pagesBackground of The Studyjeffrey rodriguezNo ratings yet
- Phason FHC1D User ManualDocument16 pagesPhason FHC1D User Manuale-ComfortUSANo ratings yet
- Early Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionDocument9 pagesEarly Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionNievecillaNeiraNo ratings yet
- This Tongue Is Not My Own Dogtooth and TDocument11 pagesThis Tongue Is Not My Own Dogtooth and TGeorgiana Geo GeoNo ratings yet
- Nanoengineered Silica-Properties PDFDocument18 pagesNanoengineered Silica-Properties PDFkevinNo ratings yet
- The Dutch Water Act in BriefDocument6 pagesThe Dutch Water Act in BriefAmit DipankarNo ratings yet
- Vespa S 125 3V Ie 150 3V Ie UPUTSTVODocument90 pagesVespa S 125 3V Ie 150 3V Ie UPUTSTVOdoughstoneNo ratings yet
- Pentingnya Memelihara Kebersihan Dan Keamanan Lingkungan Secarapartisipatif Demi Meningkatkan Gotong Royong Dan Kualitas Hidup WargaDocument6 pagesPentingnya Memelihara Kebersihan Dan Keamanan Lingkungan Secarapartisipatif Demi Meningkatkan Gotong Royong Dan Kualitas Hidup WargaMey MeyNo ratings yet
- Normal Wash, Pigment Wash, Caustic WashDocument9 pagesNormal Wash, Pigment Wash, Caustic WashTauhidurRChowdhuryNo ratings yet
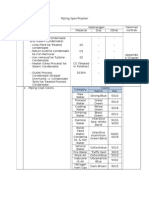
- Piping SpecificationDocument5 pagesPiping SpecificationShandi Hasnul FarizalNo ratings yet
- DR Physique Lean Bulking Series II 2015Document121 pagesDR Physique Lean Bulking Series II 2015Vlad Alexandru50% (2)
- Manual de Mantenimieno Cilindros Redondos Series MMB - HY07 - 1215 - M2 - UKDocument8 pagesManual de Mantenimieno Cilindros Redondos Series MMB - HY07 - 1215 - M2 - UKMiguel Angel LopezNo ratings yet
- Practice Q Answers Chapter 13Document8 pagesPractice Q Answers Chapter 13Benecia odoguNo ratings yet
- Science G7 Q2 LP4Document13 pagesScience G7 Q2 LP4Lovely GuintoNo ratings yet
- Bio-Organic Chem LecturesDocument205 pagesBio-Organic Chem LecturesРаони Мессиас100% (2)
- Screenshot 2021-12-18 at 2.26.56 PMDocument1 pageScreenshot 2021-12-18 at 2.26.56 PMTanya NguyenNo ratings yet
- The Winnipeg Foundation 2014 Annual ReportDocument76 pagesThe Winnipeg Foundation 2014 Annual ReportChrisDcaNo ratings yet
- Laboratory Information Management System: Prepared By: Mariela C. Ronquillo, RMTDocument33 pagesLaboratory Information Management System: Prepared By: Mariela C. Ronquillo, RMTRonel RonquilloNo ratings yet
- MASB7 Construction Contract7Document3 pagesMASB7 Construction Contract7hyraldNo ratings yet
- Trial Salary SlipDocument5 pagesTrial Salary SlipTvs12346No ratings yet
- PLKS321 Unit 8.9 PMDocument56 pagesPLKS321 Unit 8.9 PMmonagomolemo9No ratings yet
- Trane Xb13 Packaged Air Conditioner: Your Profit-AbilityDocument2 pagesTrane Xb13 Packaged Air Conditioner: Your Profit-AbilityJesus CantuNo ratings yet
- Livebook ACBDocument420 pagesLivebook ACBShubhangi JagtapNo ratings yet
- Economics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Document8 pagesEconomics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Yvette LimNo ratings yet
- Astm C 592Document9 pagesAstm C 592hoseinNo ratings yet
- Planning and Facilities: Building StorageDocument31 pagesPlanning and Facilities: Building Storagequsai migdadiNo ratings yet
- S100X220YAJ Panduit Datasheet 5314981Document2 pagesS100X220YAJ Panduit Datasheet 5314981Ilham MaurizaNo ratings yet
- Job Hazard AnalysisDocument1 pageJob Hazard AnalysisZaul tatingNo ratings yet