
Week 41-SCI PDF
Week 41-SCI PDF
You might also like
- NASM-CPT Study Guide: Domain 1: Basic and Applied Sciences andDocument49 pagesNASM-CPT Study Guide: Domain 1: Basic and Applied Sciences andsonia100% (3)
- Essentials of Rubins Pathology Sixth None Edition Ebook PDFDocument61 pagesEssentials of Rubins Pathology Sixth None Edition Ebook PDFronald.allison470100% (54)
- NASM-CPT6 Exam Study GuideDocument52 pagesNASM-CPT6 Exam Study Guidedw3541100% (11)
- Sistem Saraf 2: Ida Ayu Eka Widiastuti Bagian Fisiologi FK UnramDocument63 pagesSistem Saraf 2: Ida Ayu Eka Widiastuti Bagian Fisiologi FK UnramUpuUt Putrhie MinchuuetNo ratings yet
- Reflex DR Arpana HazarikaDocument126 pagesReflex DR Arpana HazarikaDorin Pathak100% (1)
- Motor SystemDocument116 pagesMotor SystemKhalid AlhemyariNo ratings yet
- 3 Types of Muscular SystemDocument4 pages3 Types of Muscular SystemRojan V Min KookNo ratings yet
- 035 Motor System Spinal MechanismDocument6 pages035 Motor System Spinal MechanismZeyad AmrNo ratings yet
- Disorders of The Motor System 2Document22 pagesDisorders of The Motor System 2Adel AliNo ratings yet
- AnaKines NotesDocument3 pagesAnaKines NotesLorenzSantosHernandezNo ratings yet
- Nervous SystemDocument13 pagesNervous SystemanyaNo ratings yet
- Neuroanatomy and Physiology of The Masticatory System: MAJ Joseph Lowe October 15, 2010Document76 pagesNeuroanatomy and Physiology of The Masticatory System: MAJ Joseph Lowe October 15, 2010joeylowetylerNo ratings yet
- Coordination of Movement-Lecture Notes 20201Document47 pagesCoordination of Movement-Lecture Notes 20201Zobayer AhmedNo ratings yet
- Genral Motor Function, SC and Muscle SpindlesDocument41 pagesGenral Motor Function, SC and Muscle SpindlesnoufNo ratings yet
- Systems Neuroscience Nov. 12, 2019Document37 pagesSystems Neuroscience Nov. 12, 2019TrajceNo ratings yet
- Postural ReflexesDocument25 pagesPostural ReflexesGksNo ratings yet
- Presentation 1Document27 pagesPresentation 1Junaisah P. PangaponNo ratings yet
- 15 Peripheral Nervous InjuryDocument8 pages15 Peripheral Nervous Injury楊畯凱No ratings yet
- Apex - Motor-ReflexesDocument72 pagesApex - Motor-ReflexesDill MuloshiNo ratings yet
- Reflexes, Cardiac and Smooth Muscles - PhysiologyDocument35 pagesReflexes, Cardiac and Smooth Muscles - Physiologyworldwide handsomeNo ratings yet
- Muscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Document9 pagesMuscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Rishbha TikuNo ratings yet
- MonosynaptocDocument24 pagesMonosynaptocSaad IsmailNo ratings yet
- Material Arco ReflejoDocument3 pagesMaterial Arco ReflejoV PrNo ratings yet
- Activitiy No. 12 - Human ReflexesDocument17 pagesActivitiy No. 12 - Human ReflexesTrix ThursdayNo ratings yet
- Psych ReviewerDocument20 pagesPsych ReviewerEllen Joyce P. CarnajeNo ratings yet
- Lecture - 6 - Spinal Reflexes - Source MaterialDocument19 pagesLecture - 6 - Spinal Reflexes - Source MaterialAmr KasemNo ratings yet
- CogBio - Lecture 11 - Motor System - Student - PDTDocument22 pagesCogBio - Lecture 11 - Motor System - Student - PDTsofiaNo ratings yet
- Jingying T.A. Department of PhysiologyDocument26 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Motor PathwaysDocument21 pagesMotor PathwaysSharan MurugaboopathyNo ratings yet
- Apps Functional Anatomy Lecture 3Document11 pagesApps Functional Anatomy Lecture 3joshNo ratings yet
- Lecture Notes Introduction To Nervous SystemDocument8 pagesLecture Notes Introduction To Nervous SystemKirstie Goc-ongNo ratings yet
- Reflex ActionDocument26 pagesReflex ActionMudassar RoomiNo ratings yet
- Nesc 2471-Dec 1Document7 pagesNesc 2471-Dec 1kamalleryNo ratings yet
- 4 - Motor SystemDocument20 pages4 - Motor SystemAliNo ratings yet
- Chapter 8 - Control of MovementDocument6 pagesChapter 8 - Control of MovementManilyn DacoNo ratings yet
- Lecture 13: Motor Control: Psychology 110: Biological PsychologyDocument32 pagesLecture 13: Motor Control: Psychology 110: Biological Psychologyamyle37No ratings yet
- Muscle Tone - Spinal RefelxesDocument17 pagesMuscle Tone - Spinal RefelxesLaw YouNo ratings yet
- Reflex ActionDocument22 pagesReflex Actionapi-3710331100% (2)
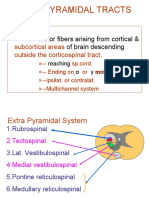
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Bio Psychology Lecture Notes CH 8Document5 pagesBio Psychology Lecture Notes CH 8Generic_PersonaNo ratings yet
- Physio Psy Module 8Document4 pagesPhysio Psy Module 8Kier Elizalde VistalNo ratings yet
- Exercise 19: Gross Anatomy of The BrainDocument5 pagesExercise 19: Gross Anatomy of The Brainbcastle1No ratings yet
- Anatomy and Physiology GMCDocument15 pagesAnatomy and Physiology GMCsamantha tanoNo ratings yet
- Report FR 9Document68 pagesReport FR 9Lance CarandangNo ratings yet
- Reflex MovementDocument24 pagesReflex MovementMuqeet76No ratings yet
- Chapter 2Document35 pagesChapter 2Amiey SehokNo ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- Essentials Strength Training Conditioning National Strength and Conditioning Association Third Edition PDF Free 1 656 26Document1 pageEssentials Strength Training Conditioning National Strength and Conditioning Association Third Edition PDF Free 1 656 26LR SantanaNo ratings yet
- (Oct 1) NERVOUS-SYSTEMDocument5 pages(Oct 1) NERVOUS-SYSTEMBea GualbertoNo ratings yet
- ReflexDocument26 pagesReflexr74k8zgg8rNo ratings yet
- CNS Notes Part 2Document14 pagesCNS Notes Part 2SudharshanNo ratings yet
- Central Nervous System: The Spinal CordDocument30 pagesCentral Nervous System: The Spinal CordRO OMNo ratings yet
- Physiology NotesDocument6 pagesPhysiology NotesGizem OsmanogluNo ratings yet
- Organization, Neurons, Basic Functions of Synapses, and NeurotransmittersDocument3 pagesOrganization, Neurons, Basic Functions of Synapses, and Neurotransmitters22 - Fernandez, Lyza Mae D.No ratings yet
- Nervous SystemDocument2 pagesNervous SystemShanel Aubrey AglibutNo ratings yet
- Medsurg Neuro AnatpathoDocument28 pagesMedsurg Neuro Anatpathoj UNo ratings yet
- MovementDocument6 pagesMovementRaven SandaganNo ratings yet
- Physiology For AnesthesiaDocument115 pagesPhysiology For AnesthesiaBahredin AbdellaNo ratings yet
- Design Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachFrom EverandDesign Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachNo ratings yet
- Bioactivity study of modified curcumin loaded polymeric nanoparticlesFrom EverandBioactivity study of modified curcumin loaded polymeric nanoparticlesNo ratings yet
- Per Devt Lesson 5&6Document6 pagesPer Devt Lesson 5&6rheyNo ratings yet
- Chapter 12 12.6 and 12.7Document16 pagesChapter 12 12.6 and 12.7Omkara HiteshNo ratings yet
- Development Milestones in ChildrenDocument69 pagesDevelopment Milestones in Childrenainzahir94No ratings yet
- MRI Lumbar Spine Without ContrastDocument2 pagesMRI Lumbar Spine Without ContrastMarco VincentiNo ratings yet
- Midterm Exam Mabio213 CMBDocument3 pagesMidterm Exam Mabio213 CMBManuel Paulo AcogidoNo ratings yet
- Cornea-Anatomy and PhysiologyDocument10 pagesCornea-Anatomy and PhysiologyMido KimoNo ratings yet
- Atlas of Ear Diseases of The Dog and Cat - 2012 - Paterson - IndexDocument6 pagesAtlas of Ear Diseases of The Dog and Cat - 2012 - Paterson - Indexnabal22No ratings yet
- Neurological Basis of Behavior Final ProjectDocument11 pagesNeurological Basis of Behavior Final ProjectArzoo NaeemNo ratings yet
- Headache HarrisonDocument21 pagesHeadache HarrisonJega PandianNo ratings yet
- THE Endocrine System: 10th GradeDocument19 pagesTHE Endocrine System: 10th GradeKyle OrlanesNo ratings yet
- The Newborn Care: Fcnlxa - St. Luke's College of NursingDocument10 pagesThe Newborn Care: Fcnlxa - St. Luke's College of NursingFrancine LaxaNo ratings yet
- Muscular SystemDocument11 pagesMuscular SystemGerarld Agbon100% (1)
- Ang Crocs 2Document59 pagesAng Crocs 2MarufNo ratings yet
- 15 Greek and Latin DoubletsDocument12 pages15 Greek and Latin DoubletsKush Kesharwani100% (1)
- MCQ On ErythropoiesisDocument6 pagesMCQ On ErythropoiesisIrekton GGNo ratings yet
- Here Is My Project ReportDocument14 pagesHere Is My Project ReportAsha PandeyNo ratings yet
- Chapter 16 The Endocrine System Chapter OutlineDocument23 pagesChapter 16 The Endocrine System Chapter OutlineMartina MicicNo ratings yet
- Reflexes ChapterDocument9 pagesReflexes ChapterVamsi KrishnaNo ratings yet
- Digeorge Orelha MediaDocument7 pagesDigeorge Orelha MediaGian BarbosaNo ratings yet
- Cancer-3 (HSS 2305) - F2022 (PowerPoint PDFDocument65 pagesCancer-3 (HSS 2305) - F2022 (PowerPoint PDFzahra.lalani14No ratings yet
- Pemf FrequenciesDocument13 pagesPemf FrequenciescumbredinNo ratings yet
- CXX - Neurosurgery NSDocument5 pagesCXX - Neurosurgery NSFarah FarahNo ratings yet
- Eye Docs PediatricsDocument133 pagesEye Docs PediatricsMuneeb ShahzadNo ratings yet
- OMFS by Manohar Sir GenezensDocument53 pagesOMFS by Manohar Sir GenezensAmrutha KasinaNo ratings yet
- Psychiatric Aspects of Liver DiseaseDocument8 pagesPsychiatric Aspects of Liver DiseaseBrian AsayasNo ratings yet
- Skeletal SystemDocument4 pagesSkeletal SystemChatterley OlanoNo ratings yet
- McMinn's Concise Human Anatomy 2nd EdDocument289 pagesMcMinn's Concise Human Anatomy 2nd Edica ssNo ratings yet
- Fibrous Dysplasia - Radiology Reference Article - RadiopaediaDocument18 pagesFibrous Dysplasia - Radiology Reference Article - RadiopaediaManuelGonzalezGaitanoNo ratings yet
- Fact Sheet Painful Peripheral NeuropathyDocument6 pagesFact Sheet Painful Peripheral Neuropathyasdar fajrinNo ratings yet
























































































Download as pdf or txt
You might also like
- NASM-CPT Study Guide: Domain 1: Basic and Applied Sciences andDocument49 pagesNASM-CPT Study Guide: Domain 1: Basic and Applied Sciences andsonia100% (3)
- Essentials of Rubins Pathology Sixth None Edition Ebook PDFDocument61 pagesEssentials of Rubins Pathology Sixth None Edition Ebook PDFronald.allison470100% (54)
- NASM-CPT6 Exam Study GuideDocument52 pagesNASM-CPT6 Exam Study Guidedw3541100% (11)
- Sistem Saraf 2: Ida Ayu Eka Widiastuti Bagian Fisiologi FK UnramDocument63 pagesSistem Saraf 2: Ida Ayu Eka Widiastuti Bagian Fisiologi FK UnramUpuUt Putrhie MinchuuetNo ratings yet
- Reflex DR Arpana HazarikaDocument126 pagesReflex DR Arpana HazarikaDorin Pathak100% (1)
- Motor SystemDocument116 pagesMotor SystemKhalid AlhemyariNo ratings yet
- 3 Types of Muscular SystemDocument4 pages3 Types of Muscular SystemRojan V Min KookNo ratings yet
- 035 Motor System Spinal MechanismDocument6 pages035 Motor System Spinal MechanismZeyad AmrNo ratings yet
- Disorders of The Motor System 2Document22 pagesDisorders of The Motor System 2Adel AliNo ratings yet
- AnaKines NotesDocument3 pagesAnaKines NotesLorenzSantosHernandezNo ratings yet
- Nervous SystemDocument13 pagesNervous SystemanyaNo ratings yet
- Neuroanatomy and Physiology of The Masticatory System: MAJ Joseph Lowe October 15, 2010Document76 pagesNeuroanatomy and Physiology of The Masticatory System: MAJ Joseph Lowe October 15, 2010joeylowetylerNo ratings yet
- Coordination of Movement-Lecture Notes 20201Document47 pagesCoordination of Movement-Lecture Notes 20201Zobayer AhmedNo ratings yet
- Genral Motor Function, SC and Muscle SpindlesDocument41 pagesGenral Motor Function, SC and Muscle SpindlesnoufNo ratings yet
- Systems Neuroscience Nov. 12, 2019Document37 pagesSystems Neuroscience Nov. 12, 2019TrajceNo ratings yet
- Postural ReflexesDocument25 pagesPostural ReflexesGksNo ratings yet
- Presentation 1Document27 pagesPresentation 1Junaisah P. PangaponNo ratings yet
- 15 Peripheral Nervous InjuryDocument8 pages15 Peripheral Nervous Injury楊畯凱No ratings yet
- Apex - Motor-ReflexesDocument72 pagesApex - Motor-ReflexesDill MuloshiNo ratings yet
- Reflexes, Cardiac and Smooth Muscles - PhysiologyDocument35 pagesReflexes, Cardiac and Smooth Muscles - Physiologyworldwide handsomeNo ratings yet
- Muscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Document9 pagesMuscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Rishbha TikuNo ratings yet
- MonosynaptocDocument24 pagesMonosynaptocSaad IsmailNo ratings yet
- Material Arco ReflejoDocument3 pagesMaterial Arco ReflejoV PrNo ratings yet
- Activitiy No. 12 - Human ReflexesDocument17 pagesActivitiy No. 12 - Human ReflexesTrix ThursdayNo ratings yet
- Psych ReviewerDocument20 pagesPsych ReviewerEllen Joyce P. CarnajeNo ratings yet
- Lecture - 6 - Spinal Reflexes - Source MaterialDocument19 pagesLecture - 6 - Spinal Reflexes - Source MaterialAmr KasemNo ratings yet
- CogBio - Lecture 11 - Motor System - Student - PDTDocument22 pagesCogBio - Lecture 11 - Motor System - Student - PDTsofiaNo ratings yet
- Jingying T.A. Department of PhysiologyDocument26 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Motor PathwaysDocument21 pagesMotor PathwaysSharan MurugaboopathyNo ratings yet
- Apps Functional Anatomy Lecture 3Document11 pagesApps Functional Anatomy Lecture 3joshNo ratings yet
- Lecture Notes Introduction To Nervous SystemDocument8 pagesLecture Notes Introduction To Nervous SystemKirstie Goc-ongNo ratings yet
- Reflex ActionDocument26 pagesReflex ActionMudassar RoomiNo ratings yet
- Nesc 2471-Dec 1Document7 pagesNesc 2471-Dec 1kamalleryNo ratings yet
- 4 - Motor SystemDocument20 pages4 - Motor SystemAliNo ratings yet
- Chapter 8 - Control of MovementDocument6 pagesChapter 8 - Control of MovementManilyn DacoNo ratings yet
- Lecture 13: Motor Control: Psychology 110: Biological PsychologyDocument32 pagesLecture 13: Motor Control: Psychology 110: Biological Psychologyamyle37No ratings yet
- Muscle Tone - Spinal RefelxesDocument17 pagesMuscle Tone - Spinal RefelxesLaw YouNo ratings yet
- Reflex ActionDocument22 pagesReflex Actionapi-3710331100% (2)
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Bio Psychology Lecture Notes CH 8Document5 pagesBio Psychology Lecture Notes CH 8Generic_PersonaNo ratings yet
- Physio Psy Module 8Document4 pagesPhysio Psy Module 8Kier Elizalde VistalNo ratings yet
- Exercise 19: Gross Anatomy of The BrainDocument5 pagesExercise 19: Gross Anatomy of The Brainbcastle1No ratings yet
- Anatomy and Physiology GMCDocument15 pagesAnatomy and Physiology GMCsamantha tanoNo ratings yet
- Report FR 9Document68 pagesReport FR 9Lance CarandangNo ratings yet
- Reflex MovementDocument24 pagesReflex MovementMuqeet76No ratings yet
- Chapter 2Document35 pagesChapter 2Amiey SehokNo ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- Essentials Strength Training Conditioning National Strength and Conditioning Association Third Edition PDF Free 1 656 26Document1 pageEssentials Strength Training Conditioning National Strength and Conditioning Association Third Edition PDF Free 1 656 26LR SantanaNo ratings yet
- (Oct 1) NERVOUS-SYSTEMDocument5 pages(Oct 1) NERVOUS-SYSTEMBea GualbertoNo ratings yet
- ReflexDocument26 pagesReflexr74k8zgg8rNo ratings yet
- CNS Notes Part 2Document14 pagesCNS Notes Part 2SudharshanNo ratings yet
- Central Nervous System: The Spinal CordDocument30 pagesCentral Nervous System: The Spinal CordRO OMNo ratings yet
- Physiology NotesDocument6 pagesPhysiology NotesGizem OsmanogluNo ratings yet
- Organization, Neurons, Basic Functions of Synapses, and NeurotransmittersDocument3 pagesOrganization, Neurons, Basic Functions of Synapses, and Neurotransmitters22 - Fernandez, Lyza Mae D.No ratings yet
- Nervous SystemDocument2 pagesNervous SystemShanel Aubrey AglibutNo ratings yet
- Medsurg Neuro AnatpathoDocument28 pagesMedsurg Neuro Anatpathoj UNo ratings yet
- MovementDocument6 pagesMovementRaven SandaganNo ratings yet
- Physiology For AnesthesiaDocument115 pagesPhysiology For AnesthesiaBahredin AbdellaNo ratings yet
- Design Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachFrom EverandDesign Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachNo ratings yet
- Bioactivity study of modified curcumin loaded polymeric nanoparticlesFrom EverandBioactivity study of modified curcumin loaded polymeric nanoparticlesNo ratings yet
- Per Devt Lesson 5&6Document6 pagesPer Devt Lesson 5&6rheyNo ratings yet
- Chapter 12 12.6 and 12.7Document16 pagesChapter 12 12.6 and 12.7Omkara HiteshNo ratings yet
- Development Milestones in ChildrenDocument69 pagesDevelopment Milestones in Childrenainzahir94No ratings yet
- MRI Lumbar Spine Without ContrastDocument2 pagesMRI Lumbar Spine Without ContrastMarco VincentiNo ratings yet
- Midterm Exam Mabio213 CMBDocument3 pagesMidterm Exam Mabio213 CMBManuel Paulo AcogidoNo ratings yet
- Cornea-Anatomy and PhysiologyDocument10 pagesCornea-Anatomy and PhysiologyMido KimoNo ratings yet
- Atlas of Ear Diseases of The Dog and Cat - 2012 - Paterson - IndexDocument6 pagesAtlas of Ear Diseases of The Dog and Cat - 2012 - Paterson - Indexnabal22No ratings yet
- Neurological Basis of Behavior Final ProjectDocument11 pagesNeurological Basis of Behavior Final ProjectArzoo NaeemNo ratings yet
- Headache HarrisonDocument21 pagesHeadache HarrisonJega PandianNo ratings yet
- THE Endocrine System: 10th GradeDocument19 pagesTHE Endocrine System: 10th GradeKyle OrlanesNo ratings yet
- The Newborn Care: Fcnlxa - St. Luke's College of NursingDocument10 pagesThe Newborn Care: Fcnlxa - St. Luke's College of NursingFrancine LaxaNo ratings yet
- Muscular SystemDocument11 pagesMuscular SystemGerarld Agbon100% (1)
- Ang Crocs 2Document59 pagesAng Crocs 2MarufNo ratings yet
- 15 Greek and Latin DoubletsDocument12 pages15 Greek and Latin DoubletsKush Kesharwani100% (1)
- MCQ On ErythropoiesisDocument6 pagesMCQ On ErythropoiesisIrekton GGNo ratings yet
- Here Is My Project ReportDocument14 pagesHere Is My Project ReportAsha PandeyNo ratings yet
- Chapter 16 The Endocrine System Chapter OutlineDocument23 pagesChapter 16 The Endocrine System Chapter OutlineMartina MicicNo ratings yet
- Reflexes ChapterDocument9 pagesReflexes ChapterVamsi KrishnaNo ratings yet
- Digeorge Orelha MediaDocument7 pagesDigeorge Orelha MediaGian BarbosaNo ratings yet
- Cancer-3 (HSS 2305) - F2022 (PowerPoint PDFDocument65 pagesCancer-3 (HSS 2305) - F2022 (PowerPoint PDFzahra.lalani14No ratings yet
- Pemf FrequenciesDocument13 pagesPemf FrequenciescumbredinNo ratings yet
- CXX - Neurosurgery NSDocument5 pagesCXX - Neurosurgery NSFarah FarahNo ratings yet
- Eye Docs PediatricsDocument133 pagesEye Docs PediatricsMuneeb ShahzadNo ratings yet
- OMFS by Manohar Sir GenezensDocument53 pagesOMFS by Manohar Sir GenezensAmrutha KasinaNo ratings yet
- Psychiatric Aspects of Liver DiseaseDocument8 pagesPsychiatric Aspects of Liver DiseaseBrian AsayasNo ratings yet
- Skeletal SystemDocument4 pagesSkeletal SystemChatterley OlanoNo ratings yet
- McMinn's Concise Human Anatomy 2nd EdDocument289 pagesMcMinn's Concise Human Anatomy 2nd Edica ssNo ratings yet
- Fibrous Dysplasia - Radiology Reference Article - RadiopaediaDocument18 pagesFibrous Dysplasia - Radiology Reference Article - RadiopaediaManuelGonzalezGaitanoNo ratings yet
- Fact Sheet Painful Peripheral NeuropathyDocument6 pagesFact Sheet Painful Peripheral Neuropathyasdar fajrinNo ratings yet