Download as pdf or txt
You might also like
- Damon Workbook-1 PDFDocument142 pagesDamon Workbook-1 PDFIrina Purwaningrum100% (7)
- 1000 Mcqs - Prosthodontics Plus March&September McqsDocument32 pages1000 Mcqs - Prosthodontics Plus March&September Mcqsdr angad69% (42)
- Modern Treatment Planning Approach Facing A Failure of Conventional Treatment. Part I: Analysis of Treatment OptionsDocument11 pagesModern Treatment Planning Approach Facing A Failure of Conventional Treatment. Part I: Analysis of Treatment OptionscdoskarNo ratings yet
- ButeykoDocument49 pagesButeykoivica_put100% (1)
- Temporary Skeletal Anchorage Devices A Guide To Design and Evidence-Based SolutionDocument238 pagesTemporary Skeletal Anchorage Devices A Guide To Design and Evidence-Based SolutionkuzakutuzaNo ratings yet
- Additive Manufacturing Techniques in Prosthodontics Where Do We Currently Stand A Critical ReviewDocument11 pagesAdditive Manufacturing Techniques in Prosthodontics Where Do We Currently Stand A Critical ReviewAlex BurdeNo ratings yet
- Mouth Breathing: Adverse Effects On Facial Growth, Health, Academics, and BehaviorDocument8 pagesMouth Breathing: Adverse Effects On Facial Growth, Health, Academics, and BehaviorlogoioanninaNo ratings yet
- The Influence of Snoring Mouth Breathing and Apnoea On Facial Morphology in Late Childhood A Three Dimensional StudyDocument9 pagesThe Influence of Snoring Mouth Breathing and Apnoea On Facial Morphology in Late Childhood A Three Dimensional StudyArockia Berlin SoniaNo ratings yet
- Craniofacial Growth Variations in Nasal-Breathing, Oral-Breathing, and Tracheotomized ChildrenDocument7 pagesCraniofacial Growth Variations in Nasal-Breathing, Oral-Breathing, and Tracheotomized Childrenj.cit28No ratings yet
- Breathing - Oral HealthDocument1 pageBreathing - Oral HealthMihai SemeniucNo ratings yet
- "Camouflage Treatment in Adenoid Facies: Long Face Syndrome"-A Case Report. - Orthodontic Cyber JouDocument11 pages"Camouflage Treatment in Adenoid Facies: Long Face Syndrome"-A Case Report. - Orthodontic Cyber Joudrrajesh27100% (1)
- Chapter 7 Deep Sedation For Pediatric PatientsDocument14 pagesChapter 7 Deep Sedation For Pediatric PatientsAhmad AbrorNo ratings yet
- Athering: Rochester, New YorkDocument5 pagesAthering: Rochester, New YorkGILBERTO AGUDELO JIMENEZNo ratings yet
- Chin CupDocument1 pageChin CupFourthMolar.comNo ratings yet
- 2014 Sharma Age Changes of Jaws and Soft Tissue Profile HighlightedDocument8 pages2014 Sharma Age Changes of Jaws and Soft Tissue Profile HighlightedHabeeb AL-AbsiNo ratings yet
- The Influence of Snoring Mouth BMJ Open 2015 Al AliDocument10 pagesThe Influence of Snoring Mouth BMJ Open 2015 Al AliAidaLimaNo ratings yet
- Maxillary ExpansionDocument6 pagesMaxillary ExpansionRosa Natalia Muente RojasNo ratings yet
- HHS Public Access: Effects of Chin-Up Posture On The Sequence of Swallowing EventsDocument30 pagesHHS Public Access: Effects of Chin-Up Posture On The Sequence of Swallowing EventsMarcia SantanaNo ratings yet
- Interaction Between Otorhinolaryngology and Orthodontics - Correlation Between The Nasopharyngeal Airway and The Craniofacial ComplexDocument8 pagesInteraction Between Otorhinolaryngology and Orthodontics - Correlation Between The Nasopharyngeal Airway and The Craniofacial ComplexGarciaNo ratings yet
- Neral ConsiderationsDocument13 pagesNeral ConsiderationsNga NguyễnNo ratings yet
- Correction of Ant Openbite Very Important PaperDocument18 pagesCorrection of Ant Openbite Very Important PaperMahdi ZakeriNo ratings yet
- Cephalometric Evaluation of Facial Pattern and Hyoid Bone Position in Children With Obstructive Sleep Apnea SyndromeDocument4 pagesCephalometric Evaluation of Facial Pattern and Hyoid Bone Position in Children With Obstructive Sleep Apnea SyndromeCEBDOF BRASILNo ratings yet
- The Role of Mouth Breathing On Dentition DevelopmeDocument5 pagesThe Role of Mouth Breathing On Dentition DevelopmeSaraNo ratings yet
- Airway ManegementDocument15 pagesAirway ManegementAnonymous HKl3Q6RbtNo ratings yet
- Udall, J (2007) Infant Feeding - Initiation, Problems, Approaches .Document26 pagesUdall, J (2007) Infant Feeding - Initiation, Problems, Approaches .Carla Francisca Rojas MerelloNo ratings yet
- Obstructive Sleep Apnea Syndrome in The Pediatric Age: The Role of The DentistDocument6 pagesObstructive Sleep Apnea Syndrome in The Pediatric Age: The Role of The DentistNadira NurinNo ratings yet
- Craniofacial and Upper Airway Morphology inDocument14 pagesCraniofacial and Upper Airway Morphology inkerminkNo ratings yet
- Laryngopharyngealreflux Diseaseinchildren: Naren N. Venkatesan,, Harold S. Pine,, Michael UnderbrinkDocument14 pagesLaryngopharyngealreflux Diseaseinchildren: Naren N. Venkatesan,, Harold S. Pine,, Michael UnderbrinkCindy Julia AmandaNo ratings yet
- B Peltomaki+2007+EurJOrthod+29+426-29Document4 pagesB Peltomaki+2007+EurJOrthod+29+426-29Edson HoribeNo ratings yet
- Relationships of Vertical Facial Pattern, Natural Head Position and Craniocervical Posture in Young Chinese ChildrenDocument8 pagesRelationships of Vertical Facial Pattern, Natural Head Position and Craniocervical Posture in Young Chinese ChildrenambersNo ratings yet
- Ucar 2011Document9 pagesUcar 2011dinaka samarathungaNo ratings yet
- Mouth Breathing Reduces Oral Function in AdolescenceDocument8 pagesMouth Breathing Reduces Oral Function in AdolescenceYasmin AfifahNo ratings yet
- Diagnosis and Management of Pediatric DysphagiaDocument9 pagesDiagnosis and Management of Pediatric DysphagiaHERNAN DANIEL RODRIGUEZ HERRERANo ratings yet
- Adenoid Hypertrophy FixDocument7 pagesAdenoid Hypertrophy FixWidi Yuli HariantoNo ratings yet
- Prevalence of Malocclusion Patterns in Mouth Breathing Children Compared To Nasal Breathing Children - A Systematic ReviewDocument11 pagesPrevalence of Malocclusion Patterns in Mouth Breathing Children Compared To Nasal Breathing Children - A Systematic ReviewhabeebNo ratings yet
- Anterior Open Bite Correction by Le Fort I or Bilateral Sagittal Split OsteotomyDocument18 pagesAnterior Open Bite Correction by Le Fort I or Bilateral Sagittal Split Osteotomyloren camila Daza GomezNo ratings yet
- The Effect of Mode of Breathing On Craniofacial Growth - RevisitedDocument4 pagesThe Effect of Mode of Breathing On Craniofacial Growth - RevisitedAya ElsayedNo ratings yet
- Desordenes de Alimentacion y DeglucionDocument10 pagesDesordenes de Alimentacion y DeglucionSOLEDAD CONTRERASNo ratings yet
- Allergy Asthma Proc 2006 p240Document4 pagesAllergy Asthma Proc 2006 p240Meilina Elin WardhaniNo ratings yet
- Perioperative Considerations in The Management of Pediatric Surgical PatientsDocument13 pagesPerioperative Considerations in The Management of Pediatric Surgical PatientsFanny Ari SandyNo ratings yet
- Positioning Improves The Oral and Pharyngeal Swallowing Function in Children With Cerebral PalsyDocument4 pagesPositioning Improves The Oral and Pharyngeal Swallowing Function in Children With Cerebral PalsySwathi GeethaNo ratings yet
- Bmri2021 5550267Document13 pagesBmri2021 5550267Shahid ShaikhNo ratings yet
- Developmental Changes of Laryngeal Dimensions in Unparalyzed, Sedated ChildrenDocument5 pagesDevelopmental Changes of Laryngeal Dimensions in Unparalyzed, Sedated ChildrenHugo LopezNo ratings yet
- Prevalence of Malocclusion in Children With Sleep Disordered BreathingDocument4 pagesPrevalence of Malocclusion in Children With Sleep Disordered BreathingMu'taz ArmanNo ratings yet
- Author's Response YmodDocument2 pagesAuthor's Response YmodMadan VermaNo ratings yet
- Infosino2002 PDFDocument20 pagesInfosino2002 PDFYosset Emilet Rodrìguez CalderònNo ratings yet
- Dysphagia Resp Swallowing Coordination Lecture NotesDocument2 pagesDysphagia Resp Swallowing Coordination Lecture NotesTaylor AckermanNo ratings yet
- HendersonDocument5 pagesHendersonErsya MuslihNo ratings yet
- MiofuncionalDocument9 pagesMiofuncionalKaterine TrillosNo ratings yet
- Facial Soft TisuesDocument6 pagesFacial Soft TisuesMoni Garcia SantosNo ratings yet
- Oral Dysfunction As A Cause of MalocclusionDocument6 pagesOral Dysfunction As A Cause of MalocclusionJULIA SANFURGO VILLARROELNo ratings yet
- Management of The Difficult Pediatric AirwayDocument9 pagesManagement of The Difficult Pediatric AirwayinescubertaNo ratings yet
- Fiber-Optic Endoscopic Evaluation of Swallowing To Assess Swallowing Outcomes As A Function of Head Position in A Normal PopulationDocument6 pagesFiber-Optic Endoscopic Evaluation of Swallowing To Assess Swallowing Outcomes As A Function of Head Position in A Normal PopulationflorensiaNo ratings yet
- LPR Disease in ChildrenDocument14 pagesLPR Disease in ChildrenChrishadi RachmawanNo ratings yet
- Pierre Robin Sequence - Manifestation and Case ReportDocument9 pagesPierre Robin Sequence - Manifestation and Case ReportAgustin guette oliverosNo ratings yet
- Pediatric Sedation Pearls: Presedation Airway Assessment Joshua Nagler, MD Children's Hospital, Boston, MADocument11 pagesPediatric Sedation Pearls: Presedation Airway Assessment Joshua Nagler, MD Children's Hospital, Boston, MAPSD12345No ratings yet
- Association Between Oral Habits, Mouth BreathingDocument9 pagesAssociation Between Oral Habits, Mouth BreathingdewiayuNo ratings yet
- PAPER (ENG) - (Shanahan T., Logemann J., Et Al., 1992 USA) Chin-Down Posture Effect On Aspiration in Dysphagic PatientsDocument5 pagesPAPER (ENG) - (Shanahan T., Logemann J., Et Al., 1992 USA) Chin-Down Posture Effect On Aspiration in Dysphagic PatientsAldo Hip NaranjoNo ratings yet
- Breathing Mode Influence in Craniofacial DevelopmentDocument5 pagesBreathing Mode Influence in Craniofacial DevelopmentAya ElsayedNo ratings yet
- Duaa DuaaDocument27 pagesDuaa DuaaDoaa TahseenNo ratings yet
- Nss 10 271Document16 pagesNss 10 271杨钦杰No ratings yet
- Laryngomalacia and Swallowing Function in ChildrenDocument7 pagesLaryngomalacia and Swallowing Function in ChildrenmelaniaNo ratings yet
- Synosis Finl JDocument7 pagesSynosis Finl JPrasanna MarandiNo ratings yet
- Relationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Young Chinese ChildrenDocument7 pagesRelationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Young Chinese ChildrenTanya HernandezNo ratings yet
- Adenoids and Diseased Tonsils: Their Effect on General IntelligenceFrom EverandAdenoids and Diseased Tonsils: Their Effect on General IntelligenceNo ratings yet
- Microcephalic Osteodyplastic Primordial Dwarfism Type II, Case Report With Unique Oral Findingd and A New Mutation in The Pericentrin GeneDocument8 pagesMicrocephalic Osteodyplastic Primordial Dwarfism Type II, Case Report With Unique Oral Findingd and A New Mutation in The Pericentrin GeneFran GidiNo ratings yet
- R ChairsideGuideDocument2 pagesR ChairsideGuideFran GidiNo ratings yet
- Management of Dental Emergencies in Children and Adolescents - 2019 - Neuhaus PDFDocument296 pagesManagement of Dental Emergencies in Children and Adolescents - 2019 - Neuhaus PDFFran GidiNo ratings yet
- Management of Odontogenic Infection in Paediatric Patients: A Retrospective Clinical StudyDocument10 pagesManagement of Odontogenic Infection in Paediatric Patients: A Retrospective Clinical StudyFran GidiNo ratings yet
- 8.review Meenu Mary PaulDocument10 pages8.review Meenu Mary PaulNICULAE SIMONANo ratings yet
- AIA Group Dental PPO Plus Dental List - July 2016Document10 pagesAIA Group Dental PPO Plus Dental List - July 2016akkakarania100% (1)
- MDS CQ Non Service Phase2 College Wise AllotmentsDocument17 pagesMDS CQ Non Service Phase2 College Wise Allotmentssssrao575No ratings yet
- Fluid Control & Soft Tissue Management in FPDDocument63 pagesFluid Control & Soft Tissue Management in FPDvestaenid50% (2)
- LM Arte Brochure enDocument16 pagesLM Arte Brochure enaurummaangxinchenNo ratings yet
- FrankelDocument8 pagesFrankeldavid torresNo ratings yet
- Al Mamzar Health Center2022241794Document48 pagesAl Mamzar Health Center2022241794rajeshrajbhavanNo ratings yet
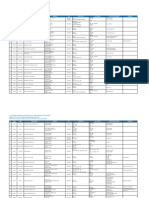
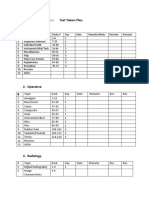
- NBDE PART 2::::::::::::::::::: Test Takers Plan 1. EndodonticsDocument6 pagesNBDE PART 2::::::::::::::::::: Test Takers Plan 1. EndodonticsEmma LiamNo ratings yet
- Ortho MfaDocument120 pagesOrtho Mfasudssharma512No ratings yet
- Comm DentDocument47 pagesComm DentEunice Joy MallariNo ratings yet
- Clasificacion Horizontal Del Reborde - FlattenedDocument28 pagesClasificacion Horizontal Del Reborde - FlattenedJuan Carlos Montañez BenavidesNo ratings yet
- Orto Paro 2Document6 pagesOrto Paro 2adk eijfNo ratings yet
- HEALTH 6 - Q1 - Mod3Document19 pagesHEALTH 6 - Q1 - Mod3FernandoNo ratings yet
- Flexible Denture Base Material A Viable AlternativDocument5 pagesFlexible Denture Base Material A Viable AlternativRaluca ChisciucNo ratings yet
- English AJODO 2004Document3 pagesEnglish AJODO 2004Diego Andres Hincapie HerreraNo ratings yet
- L1 Periodontal Flaps (2) Last L9Document50 pagesL1 Periodontal Flaps (2) Last L9Haneen Al-HajjNo ratings yet
- Extractions in OrthodonticsDocument6 pagesExtractions in OrthodonticsZubair AhmedNo ratings yet
- Caries Case Study FinalDocument17 pagesCaries Case Study Finalapi-548943155No ratings yet
- Gothic Arch Tracing - RainaDocument99 pagesGothic Arch Tracing - RainaGoutham Sunil100% (4)
- Impacted Canine: Presented By: Dr. Ahmed Shihab Supervised By: Dr. SarahDocument34 pagesImpacted Canine: Presented By: Dr. Ahmed Shihab Supervised By: Dr. SarahAhmed ShihabNo ratings yet
- Jcda 2021 AiDocument8 pagesJcda 2021 AiSherienNo ratings yet
- Atypical Odontalgia Current Knowledge and Implications For Diagnosis and ManagementDocument5 pagesAtypical Odontalgia Current Knowledge and Implications For Diagnosis and ManagementIma ShofyaNo ratings yet
- 3A Teeth Questions PDFDocument10 pages3A Teeth Questions PDFYee MeiNo ratings yet
- Oral Anatomy and Physiology (Review Center)Document13 pagesOral Anatomy and Physiology (Review Center)yellow rangerNo ratings yet
- Orthodontic Treatment of Severe Crowding Malocclusion With Extraction of PremolarsDocument4 pagesOrthodontic Treatment of Severe Crowding Malocclusion With Extraction of Premolarsyuni madjidNo ratings yet