Download as docx, pdf, or txt
You might also like
- Gordon's 11 Functional Health Patterns AssessmentDocument2 pagesGordon's 11 Functional Health Patterns Assessmentmtuckrn84% (37)
- Obsessive-Compulsive Disorder (OCD) Screening ToolDocument2 pagesObsessive-Compulsive Disorder (OCD) Screening ToolManiya Dianne ReyesNo ratings yet
- 4100XPB 4198 Grupo Mexico CananDocument758 pages4100XPB 4198 Grupo Mexico CananWalissonNo ratings yet
- Wifi Jammer: Winter Semester 2020-21 Analog Circuits Ece 2028Document10 pagesWifi Jammer: Winter Semester 2020-21 Analog Circuits Ece 2028Sathwik YadalamNo ratings yet
- Dast20 PDFDocument3 pagesDast20 PDFMarchnuelNo ratings yet
- Short Long Geriatric Depression Scale GDSDocument2 pagesShort Long Geriatric Depression Scale GDSRose WidantiNo ratings yet
- Gordon S 11 Functional Hhhhhealth Patterns AssessmentDocument2 pagesGordon S 11 Functional Hhhhhealth Patterns AssessmentMark Pabalan100% (2)
- Hydraulic Axial Piston Eaton Vickers PVB Pump: - Basic CharacteristicsDocument13 pagesHydraulic Axial Piston Eaton Vickers PVB Pump: - Basic Characteristicsjose alberto olvera gomezNo ratings yet
- Carbon Footprint of Organic FertilizerDocument5 pagesCarbon Footprint of Organic FertilizerSteve Savage100% (6)
- Questionnaire 2Document19 pagesQuestionnaire 2Inayat KhanNo ratings yet
- DocumentDocument1 pageDocumentkennnnnnyroseNo ratings yet
- Questionnaire (F)Document4 pagesQuestionnaire (F)alley_ingreens86No ratings yet
- Health and Wellbeing Questionnaire: 1. GenderDocument6 pagesHealth and Wellbeing Questionnaire: 1. GenderesthermadNo ratings yet
- Gordon Interview QuestionsDocument2 pagesGordon Interview QuestionskennnnnnyroseNo ratings yet
- Biographical Data 1Document7 pagesBiographical Data 1Maddi AlonzoNo ratings yet
- Clinical Interview AdultDocument12 pagesClinical Interview AdultPrince Arora100% (1)
- GDS 4 & GDS 15 EnglishDocument4 pagesGDS 4 & GDS 15 EnglishyenaxoNo ratings yet
- Self AssessmentDocument2 pagesSelf Assessmentcheatingw995No ratings yet
- QuestionnaireDocument1 pageQuestionnaireOmer Abdul SattarNo ratings yet
- Psychiatry (1) 1Document26 pagesPsychiatry (1) 1esmatNo ratings yet
- FHP Guide QuestionsDocument1 pageFHP Guide QuestionsKit Alizon BarredoNo ratings yet
- GordonsDocument7 pagesGordonsDawn EncarnacionNo ratings yet
- Individual Therapy QuestionDocument6 pagesIndividual Therapy Questionshrey.thapa123No ratings yet
- Assess Any Aggravating or Relieving FactorsDocument5 pagesAssess Any Aggravating or Relieving Factorsbread genieNo ratings yet
- Clinics 6 GuideDocument31 pagesClinics 6 GuideAllysa Marie CotandaNo ratings yet
- Teen CounselingDocument4 pagesTeen Counselingshrey.thapa123No ratings yet
- Taking My Vitamins: Nutritional MetabolicDocument5 pagesTaking My Vitamins: Nutritional MetabolicRichie VilaNo ratings yet
- Psychological Test BatteriesDocument23 pagesPsychological Test BatteriesMinagaFathmaSonnayaNo ratings yet
- Health QuestionnaireDocument2 pagesHealth QuestionnaireSarahNo ratings yet
- Health Question Air ReDocument2 pagesHealth Question Air ReVithun RajNo ratings yet
- Speaking Practice With PicturesDocument22 pagesSpeaking Practice With PicturesLiaNo ratings yet
- Survey File On DrugDocument2 pagesSurvey File On Drugkavita rajputNo ratings yet
- Geriatric Client Profiling ToolDocument3 pagesGeriatric Client Profiling ToolJihad U. ShariefNo ratings yet
- Synopsis of Clinical Diagnostic Interview QuestionsDocument2 pagesSynopsis of Clinical Diagnostic Interview QuestionsRoxanne ForbesNo ratings yet
- Sample Barrier Analysis QuestionnaireDocument5 pagesSample Barrier Analysis QuestionnairedrsgNo ratings yet
- Psychology 3.06 Agesand StagesDocument4 pagesPsychology 3.06 Agesand StagessarabatacheNo ratings yet
- DoneiguessDocument12 pagesDoneiguessJOHN ROIENo ratings yet
- Cancer Screening QuestionnaireDocument3 pagesCancer Screening QuestionnaireakashniranjaneNo ratings yet
- Geriatric Depression Scale (Short Form) : Joanna Padiaon MAY 10, 2020Document2 pagesGeriatric Depression Scale (Short Form) : Joanna Padiaon MAY 10, 2020Jess RitumaltaNo ratings yet
- Dokumen - Tips Gordons 11 Functional Health Patterns AssessmentDocument2 pagesDokumen - Tips Gordons 11 Functional Health Patterns AssessmentLucky Dela cruzNo ratings yet
- Depression ChecklistDocument2 pagesDepression ChecklistWaseem QureshiNo ratings yet
- Gordon'sDocument4 pagesGordon'sJetch DyNo ratings yet
- Speaking Nastya EngDocument5 pagesSpeaking Nastya EngNatalyNo ratings yet
- Interview FormDocument4 pagesInterview FormMark Jheran AlvarezNo ratings yet
- Gordong English VersionDocument11 pagesGordong English VersionCassey Faith UtaydeNo ratings yet
- Lewis Questionnaire 1Document2 pagesLewis Questionnaire 1Ezie Lewis AmobiNo ratings yet
- DAST FormDocument1 pageDAST FormКонстантин КрахмалевNo ratings yet
- Clinical Assessment Questionnare 1Document13 pagesClinical Assessment Questionnare 1Iris FuedanNo ratings yet
- Gordon S 11 Functional Health Patterns AssessmentDocument2 pagesGordon S 11 Functional Health Patterns AssessmentSunny ChengNo ratings yet
- Adult Case HistoryDocument16 pagesAdult Case HistoryLaiba AttiqueNo ratings yet
- Gordon's 11 Functional Health PatternsDocument5 pagesGordon's 11 Functional Health PatternsHanah TobiasNo ratings yet
- 11 Gordon's Functional Health PatternDocument2 pages11 Gordon's Functional Health Patternrichelleambrocio054No ratings yet
- Simple Screening Instrument For Substance Abuse: Appendix C-Provider Forms, Measures, and ToolsDocument1 pageSimple Screening Instrument For Substance Abuse: Appendix C-Provider Forms, Measures, and ToolsAmel EzNo ratings yet
- Be Kind To Your Mind: Stress Coping Strategies For Grade 10 StudentsDocument11 pagesBe Kind To Your Mind: Stress Coping Strategies For Grade 10 StudentsMark Byncent Mejorada BayugaNo ratings yet
- Clinical Diagnostic InterviewDocument3 pagesClinical Diagnostic InterviewLolea AlinNo ratings yet
- Stress QuestionnaireDocument1 pageStress QuestionnairejesrellcanasNo ratings yet
- Family PlanningDocument3 pagesFamily PlanningKristyan DeybNo ratings yet
- Survey Questionnaire For GBV Victims and Concerned StakeholdersDocument20 pagesSurvey Questionnaire For GBV Victims and Concerned StakeholdersPaola Ciarra ValenciaNo ratings yet
- Assessment For Duty 2Document19 pagesAssessment For Duty 2Kim TangoNo ratings yet
- Code Blue Group-Psychiatry History FormatDocument10 pagesCode Blue Group-Psychiatry History FormatsakariyeNo ratings yet
- DAST Questionnaire - DRUG ABUSEDocument1 pageDAST Questionnaire - DRUG ABUSErichieerishiNo ratings yet
- Questionnaire On Stress - Part 1Document2 pagesQuestionnaire On Stress - Part 1khushi agarwalNo ratings yet
- The Fix for Cravings: One(S) That Didn’t Work, and Now One Which WorksFrom EverandThe Fix for Cravings: One(S) That Didn’t Work, and Now One Which WorksNo ratings yet
- Market and Financial RisksDocument5 pagesMarket and Financial RisksTimothy NdegeNo ratings yet
- Lecture 5-1 TripAssignmentInClassDocument3 pagesLecture 5-1 TripAssignmentInClassTimothy NdegeNo ratings yet
- Effective Project Resource Acquisition For Small and Medium Scale Construction Projects... (1-24)Document12 pagesEffective Project Resource Acquisition For Small and Medium Scale Construction Projects... (1-24)Timothy NdegeNo ratings yet
- Lecture 5-1 MSADocument1 pageLecture 5-1 MSATimothy NdegeNo ratings yet
- Muscular Triangles of The NeckDocument3 pagesMuscular Triangles of The NeckSam TagardaNo ratings yet
- SPE 13932 Wettability Part2 AndersonDocument17 pagesSPE 13932 Wettability Part2 AndersonSergio EduardoNo ratings yet
- PROJECT On Tea LeavesDocument15 pagesPROJECT On Tea LeavesBharat Singh83% (6)
- Anesthesia Machine Aeonmed GLORY PLUSDocument2 pagesAnesthesia Machine Aeonmed GLORY PLUSousmane100% (4)
- 555-Timer AStable and MonostableDocument13 pages555-Timer AStable and MonostableenzuekNo ratings yet
- Msds-Of M 220-Eng - 43-29357Document13 pagesMsds-Of M 220-Eng - 43-29357Lennier SaezNo ratings yet
- Silvestres Grupo 5Document39 pagesSilvestres Grupo 5Juliana DiazNo ratings yet
- Phason FHC1D User ManualDocument16 pagesPhason FHC1D User Manuale-ComfortUSANo ratings yet
- Discard ManagementDocument9 pagesDiscard ManagementDevvrath SinghNo ratings yet
- John White Videos of Spooky2 InterfaceDocument24 pagesJohn White Videos of Spooky2 InterfaceTimothy M HallNo ratings yet
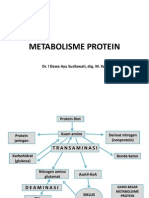
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Ebook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFDocument67 pagesEbook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFrobert.davidson233100% (31)
- Parental/Guardian Permission and Liability Waiver Name of Student BirthDocument2 pagesParental/Guardian Permission and Liability Waiver Name of Student BirthlifeteenministryNo ratings yet
- Stress and Coping Strategies Among Distance Education Students at The University of Cape Coast, GhanaDocument15 pagesStress and Coping Strategies Among Distance Education Students at The University of Cape Coast, GhanaReign EvansNo ratings yet
- Grade 12 LM Physical Science 1 Module4Document21 pagesGrade 12 LM Physical Science 1 Module4ladyheart ۦۦNo ratings yet
- Autoconceito ShavelsonDocument15 pagesAutoconceito ShavelsonJuliana SchwarzNo ratings yet
- To, The Medical Superintendent, Services Hospital LahoreDocument1 pageTo, The Medical Superintendent, Services Hospital LahoreAfraz AliNo ratings yet
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
- The AwakeningDocument4 pagesThe AwakeningRIMMA DATILESNo ratings yet
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- Barron's Bigbook Special WordDocument123 pagesBarron's Bigbook Special WordArif Al MamunNo ratings yet
- Altitude, Cloud Cover and LatitudeDocument64 pagesAltitude, Cloud Cover and LatitudeIsarra AmsaluNo ratings yet
- Weekly Report ExampleDocument3 pagesWeekly Report Examplewawan setiawanNo ratings yet
- 15 Proven Recipes To Most Desirable & Delicious Ice Creams.Document19 pages15 Proven Recipes To Most Desirable & Delicious Ice Creams.viaindiankitchenNo ratings yet
- BWT - HandbookDocument16 pagesBWT - HandbookDarko DuiloNo ratings yet