Download as pdf or txt
You might also like
- Ambu Sleepmate Poster PDFDocument1 pageAmbu Sleepmate Poster PDFMinh Triết LêNo ratings yet
- Self Declaration For Registered Pharmacist: Annexure BDocument1 pageSelf Declaration For Registered Pharmacist: Annexure BRathod SirNo ratings yet
- Week 6 Assignment: Creating MeasuresDocument7 pagesWeek 6 Assignment: Creating MeasuresDrNo ratings yet
- Instruments To Measure Patient Experience of Health Care Quality in Hospitals: A Systematic Review ProtocolDocument8 pagesInstruments To Measure Patient Experience of Health Care Quality in Hospitals: A Systematic Review ProtocolLastriNo ratings yet
- JETIR2302568Document45 pagesJETIR2302568gundlapalli.2023No ratings yet
- Instruments To Measure Patient Experience of Healthcare Quality in Hospitals: A Systematic ReviewDocument21 pagesInstruments To Measure Patient Experience of Healthcare Quality in Hospitals: A Systematic ReviewVĩ Vũ NgọcNo ratings yet
- Nurse's Experience Working 12-Hour Shift in A Tertiary Level Hospital in Qatar: A Mixed Method StudyDocument12 pagesNurse's Experience Working 12-Hour Shift in A Tertiary Level Hospital in Qatar: A Mixed Method Studybejoy1987No ratings yet
- Burnout and Work Privacy ConflictDocument9 pagesBurnout and Work Privacy Conflictritauni042002No ratings yet
- Effect of Appointment System On Waiting Time of PatientsDocument49 pagesEffect of Appointment System On Waiting Time of PatientsPelumi Adebayo100% (1)
- In Total With Result 1Document65 pagesIn Total With Result 1arshad khanNo ratings yet
- Designing An Appointment System For An OutpatientDocument9 pagesDesigning An Appointment System For An OutpatientDAD SHOTSNo ratings yet
- 2019 Article 4685Document13 pages2019 Article 4685kaniNo ratings yet
- Effect of Prescription Waiting Time On Patient Satisfaction Mediated by Service Quality of Pharmacy Unit in Public Hospital in Bandung CityDocument6 pagesEffect of Prescription Waiting Time On Patient Satisfaction Mediated by Service Quality of Pharmacy Unit in Public Hospital in Bandung CityElfis WahyuniNo ratings yet
- Indry Prof CyruzDocument5 pagesIndry Prof CyruzPatrick LukitoNo ratings yet
- Empathy and Burnout in Medical StaffDocument13 pagesEmpathy and Burnout in Medical StaffIWANNAWIWANINo ratings yet
- Patient Satisfaction at Tertiary Level Healthcare Services in Greece: Inpatient Vs Outpatient Healthcare Services AssessmentDocument12 pagesPatient Satisfaction at Tertiary Level Healthcare Services in Greece: Inpatient Vs Outpatient Healthcare Services AssessmentSelfa YunitaNo ratings yet
- Patients' Waiting Time: Indices For Measuring Hospital EffectivenessDocument18 pagesPatients' Waiting Time: Indices For Measuring Hospital Effectivenessmr kevinNo ratings yet
- Wait Times Ip June 2012Document5 pagesWait Times Ip June 2012MarloNo ratings yet
- Assessing Needs-Based Supply of Physicians - A Criteria-Led Methodological Review of International Studies in High-Resource SettingsDocument19 pagesAssessing Needs-Based Supply of Physicians - A Criteria-Led Methodological Review of International Studies in High-Resource SettingsPatri BarberNo ratings yet
- Osteoarthritis Physical Activity Care Pathway (OA-PCP) : Results of A Feasibility TrialDocument11 pagesOsteoarthritis Physical Activity Care Pathway (OA-PCP) : Results of A Feasibility TrialrahmarahmatNo ratings yet
- The Evaluation of Outpatient Quality Services in Physiotherapy in The Teaching Health Centers of Shahid Beheshti University Based On Servqual ToolsDocument8 pagesThe Evaluation of Outpatient Quality Services in Physiotherapy in The Teaching Health Centers of Shahid Beheshti University Based On Servqual Toolspt.mahmoudNo ratings yet
- A Study On Waiting Time of The OPD Patient in A Multispecialty HospitalDocument6 pagesA Study On Waiting Time of The OPD Patient in A Multispecialty HospitalIJRASETPublicationsNo ratings yet
- s12912 022 00990 3Document11 pagess12912 022 00990 3ibrahim salimNo ratings yet
- Blue Card WordDocument5 pagesBlue Card WordDash WaniNo ratings yet
- ChineDocument11 pagesChineapouakone apouakoneNo ratings yet
- Managing Patient Expectations at Emergency Department TriageDocument15 pagesManaging Patient Expectations at Emergency Department TriageHans GrobakNo ratings yet
- Effectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee OsteoarthritisDocument17 pagesEffectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee Osteoarthritisyago.pessoaNo ratings yet
- Organizational Factors Affecting Length of Stay in The Emergency DepartmentDocument7 pagesOrganizational Factors Affecting Length of Stay in The Emergency DepartmentZULKIFLI POMALANGONo ratings yet
- International Journal of Health Sciences and ResearchDocument8 pagesInternational Journal of Health Sciences and ResearchNur Mutmainnah RahmanNo ratings yet
- Patient' Satisfaction and Quality of Healthcare: Case of Hospitals in Ho Chi Minh CityDocument16 pagesPatient' Satisfaction and Quality of Healthcare: Case of Hospitals in Ho Chi Minh CityPSAKU International Journal of Interdisciplinary ResearchNo ratings yet
- s13063 019 3444 yDocument12 pagess13063 019 3444 yAlessandra BendoNo ratings yet
- Patient's Satisfaction With Nursing Care Provided in Selected Areas of Tertiary Care Hospital 1Document13 pagesPatient's Satisfaction With Nursing Care Provided in Selected Areas of Tertiary Care Hospital 1Anonymous CuWlCKxXkENo ratings yet
- The Relationship Between Waiting Time and Patient Satisfaction in The Outpatient of Public Hospital in BanjarbaruDocument7 pagesThe Relationship Between Waiting Time and Patient Satisfaction in The Outpatient of Public Hospital in BanjarbaruWijayadi SuyonoNo ratings yet
- Patient SatifactionDocument9 pagesPatient SatifactionAndrew CharlesNo ratings yet
- Rs 3Document8 pagesRs 3kgarg1be21No ratings yet
- Shubha MukherjeeDocument37 pagesShubha Mukherjeeshivamray877No ratings yet
- The Effect of Delegation of Therapy To Allied Health AssistedDocument16 pagesThe Effect of Delegation of Therapy To Allied Health AssistedAquafinaNo ratings yet
- 1136 4024 1 PBDocument7 pages1136 4024 1 PBTanish gogwalNo ratings yet
- A Qualitative System Dynamics Model For Efects of Workplace Violence and Clinician Burnout On Agitation Management in The Emergency DepartmentDocument13 pagesA Qualitative System Dynamics Model For Efects of Workplace Violence and Clinician Burnout On Agitation Management in The Emergency Departmentmargi13No ratings yet
- Impact of IADocument14 pagesImpact of IAMichieru5No ratings yet
- Exposé: Title of The ThesisDocument10 pagesExposé: Title of The Thesiscb67No ratings yet
- s12913 022 08783 9Document23 pagess12913 022 08783 9Shuai ShaoNo ratings yet
- Work-Related Medical RehabilitDocument12 pagesWork-Related Medical RehabilitMonicawindyNo ratings yet
- Using Simulation-Based Training During Hospital Relocation: A Controlled Intervention StudyDocument10 pagesUsing Simulation-Based Training During Hospital Relocation: A Controlled Intervention StudyLucas InacioNo ratings yet
- Patient Centredness and QualityDocument7 pagesPatient Centredness and QualityAntonelle BeharryNo ratings yet
- Managing Patient Expectations at Emergency Department Triage PDFDocument15 pagesManaging Patient Expectations at Emergency Department Triage PDFCaesar CeblonkNo ratings yet
- A Preliminary Study On Applying Holistic Health Care Model On Medical Education Behavioral Intention: A Theoretical Perspective of Planned BehaviorDocument7 pagesA Preliminary Study On Applying Holistic Health Care Model On Medical Education Behavioral Intention: A Theoretical Perspective of Planned BehaviorJean o LeraNo ratings yet
- Patient Satisfaction: A Study in General and Private Wards of A Multispecialty HospitalDocument15 pagesPatient Satisfaction: A Study in General and Private Wards of A Multispecialty HospitalAr AmirNo ratings yet
- s12913-023-10405-xDocument14 pagess12913-023-10405-xYENER CRISTYELL VALLE ARANDANo ratings yet
- Felicidad Ocupacional en Enfermeras de ChinaDocument9 pagesFelicidad Ocupacional en Enfermeras de ChinaDenali QCNo ratings yet
- Simulation-Based Evaluation of Operating Room Management PoliciesDocument13 pagesSimulation-Based Evaluation of Operating Room Management Policiessriyanto ibsNo ratings yet
- Investigating The Healthcare Pathway Through Patients ' Experience and Profiles: Implications For Breast Cancer Healthcare ProvidersDocument11 pagesInvestigating The Healthcare Pathway Through Patients ' Experience and Profiles: Implications For Breast Cancer Healthcare ProvidersAbba HawiiNo ratings yet
- This Content Downloaded From 197.251.215.100 On Tue, 14 Mar 2023 04:45:30 UTCDocument7 pagesThis Content Downloaded From 197.251.215.100 On Tue, 14 Mar 2023 04:45:30 UTCMichael AkortsuNo ratings yet
- The Transdiagnostic Intervention For Sleep and CirDocument16 pagesThe Transdiagnostic Intervention For Sleep and CirSimonia CoutinhoNo ratings yet
- Jurnal PRBDocument5 pagesJurnal PRBJoanne AngelinaNo ratings yet
- Chapter 2Document7 pagesChapter 2Aliyu SalisuNo ratings yet
- s13033 018 0217 ZDocument7 pagess13033 018 0217 ZtemesgenNo ratings yet
- Application of Queuing Theory To Optimize Waiting-Time in Hospital OperationsDocument21 pagesApplication of Queuing Theory To Optimize Waiting-Time in Hospital OperationsAdrianaNo ratings yet
- Application of Queuing Theory To Optimize Waiting-Time in Hospital OperationsDocument21 pagesApplication of Queuing Theory To Optimize Waiting-Time in Hospital OperationsAdrianaNo ratings yet
- Customer Satisfaction With Clinical Laboratory SerdfgafDocument23 pagesCustomer Satisfaction With Clinical Laboratory SerdfgafcathialphaNo ratings yet
- Textbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionFrom EverandTextbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionNo ratings yet
- Strategies to Explore Ways to Improve Efficiency While Reducing Health Care CostsFrom EverandStrategies to Explore Ways to Improve Efficiency While Reducing Health Care CostsNo ratings yet
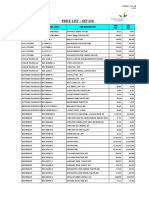
- Pharma Items - Pricelist - Nov 2021Document12 pagesPharma Items - Pricelist - Nov 2021habat albarakah-phgNo ratings yet
- Sleep PositionDocument2 pagesSleep PositionHazirah MustapaNo ratings yet
- Skims Medical College & HospitalDocument5 pagesSkims Medical College & HospitalAaQib BhatNo ratings yet
- Lab Report 14570260 20230930054510 230930 174713Document2 pagesLab Report 14570260 20230930054510 230930 174713Muhammad Zayan AliNo ratings yet
- DDB Board Resolution No. 4, S 2007-Operation Private EyeDocument3 pagesDDB Board Resolution No. 4, S 2007-Operation Private EyeCrizalde de DiosNo ratings yet
- MB AED7000 AED7000 Plus Technical Specifications BrochureDocument4 pagesMB AED7000 AED7000 Plus Technical Specifications BrochureCobin ServicioNo ratings yet
- Review: Ocular Toxoplasmosis II: Clinical Features, Pathology and ManagementDocument14 pagesReview: Ocular Toxoplasmosis II: Clinical Features, Pathology and Managementhidrisdmnk_747467972No ratings yet
- Ozlex Tea ADocument3 pagesOzlex Tea AbiancaNo ratings yet
- OPT Plus Form 1A - WT 4 AgeDocument2 pagesOPT Plus Form 1A - WT 4 Agebhagzc khuyaNo ratings yet
- Arab HealthDocument6 pagesArab HealthZETTYNo ratings yet
- Heart Attack Risk Assessment ModelDocument13 pagesHeart Attack Risk Assessment ModelmbowejNo ratings yet
- Accuracy of Firstbeat Bodyguard 2 Beat-To-Beat Heart Rate MonitorDocument3 pagesAccuracy of Firstbeat Bodyguard 2 Beat-To-Beat Heart Rate Monitorbabin tNo ratings yet
- Urinary System Regulation of Fluid BalanceDocument8 pagesUrinary System Regulation of Fluid BalanceQuỳnh NguyễnNo ratings yet
- 8-Article Text-9-1-10-20180905Document6 pages8-Article Text-9-1-10-20180905MahaTri YudhaputraNo ratings yet
- Orthodontics ReviewerDocument20 pagesOrthodontics ReviewerJAMIE E. EULLARANNo ratings yet
- Post Insertion Phase.Document33 pagesPost Insertion Phase.Khan MksksNo ratings yet
- Relatoriu Kazu CopdDocument11 pagesRelatoriu Kazu CopdMario KapeNo ratings yet
- SSH Usulan Baru 2021 - SeptemberDocument15 pagesSSH Usulan Baru 2021 - SeptemberM Alfredo AhwanNo ratings yet
- LSFD ExamDocument4 pagesLSFD ExamPlayNo ratings yet
- Nursing Documentation1Document3 pagesNursing Documentation1Paskuman DinkesNo ratings yet
- Science and Technology WritingDocument14 pagesScience and Technology WritingMary Ann AysonNo ratings yet
- English Homeopathy CatalogueDocument28 pagesEnglish Homeopathy CatalogueWasek SarkerNo ratings yet
- Medication Transcription Practice Sheet1 Updated 2015 (4) - 1Document3 pagesMedication Transcription Practice Sheet1 Updated 2015 (4) - 1MikeNo ratings yet
- Fitomelatonina e ErvasDocument6 pagesFitomelatonina e ErvasCybelle LiraNo ratings yet
- Anti-Human GlobulinDocument7 pagesAnti-Human GlobulinDominic EmerencianaNo ratings yet
- Handling Hewan UjiDocument36 pagesHandling Hewan UjiSyahna AprilianiNo ratings yet
- HemodialysisDocument19 pagesHemodialysisDonita Meña LaroyaNo ratings yet
- Professional Regulation Commission Manila Veterinarians MARCH 1, 2 AND 3, 2023Document14 pagesProfessional Regulation Commission Manila Veterinarians MARCH 1, 2 AND 3, 2023Giecel Marie SerranoNo ratings yet