Download as pdf or txt
You might also like
- Case Study, Chapter 42, Management of Patients With Musculoskeletal TraumaDocument2 pagesCase Study, Chapter 42, Management of Patients With Musculoskeletal TraumaAhmad BaolayyanNo ratings yet
- Uterine Atony: Cudanin, Regine R. Kimaykimay, Angeline PDocument31 pagesUterine Atony: Cudanin, Regine R. Kimaykimay, Angeline PregNo ratings yet
- Assessment Nursing Diagnosis Goal/ Objective Intervention EvaluationDocument1 pageAssessment Nursing Diagnosis Goal/ Objective Intervention Evaluationjezreel ibarraNo ratings yet
- Health Teaching Plan For Newborn ScreeningDocument4 pagesHealth Teaching Plan For Newborn ScreeningPrincess Pauline AbrasaldoNo ratings yet
- Calculation of DietsDocument5 pagesCalculation of DietsAEROSE JILLIAN PADILLANo ratings yet
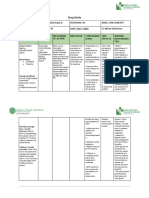
- Drug Study PDFDocument14 pagesDrug Study PDFsretirado02No ratings yet
- Ophthalmia NeonatorumDocument5 pagesOphthalmia NeonatorumYhanna UlfianiNo ratings yet
- Problems With The 4ps of LaborDocument10 pagesProblems With The 4ps of LaborhoohooNo ratings yet
- 01 Chapter Anti InfectiveDocument90 pages01 Chapter Anti InfectiveMSKCNo ratings yet
- NCP Draft - Ectopic PregnancyDocument7 pagesNCP Draft - Ectopic PregnancyD CNo ratings yet
- Ectopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Document10 pagesEctopic Pregnancy NCP (Vizconde, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNo ratings yet
- Post PartumDocument22 pagesPost PartumShaira Mae Yante RomeroNo ratings yet
- MCN Final ExamDocument39 pagesMCN Final ExamAshley RegisNo ratings yet
- SDL - 4.pdf AnotherDocument3 pagesSDL - 4.pdf AnotherJose Troy NgoaNo ratings yet
- OB Ward Exposure Prepared By: Group G and Group HDocument10 pagesOB Ward Exposure Prepared By: Group G and Group HJannah Marie A. DimaporoNo ratings yet
- Hyperthermia: A Nursing Care Plan Presented To Maria Catherine Belarma, RN, MNDocument6 pagesHyperthermia: A Nursing Care Plan Presented To Maria Catherine Belarma, RN, MNJanelle NarcisoNo ratings yet
- Ra - 7846 - An Act Requiring Compulsory ImmunizationDocument1 pageRa - 7846 - An Act Requiring Compulsory ImmunizationAt Day's WardNo ratings yet
- Nrg203: Care of Mother, Child, and Adolescent: (StudentDocument6 pagesNrg203: Care of Mother, Child, and Adolescent: (Studentmikhaela sencilNo ratings yet
- Ru Ward ClassDocument12 pagesRu Ward ClassAmal MUTIANo ratings yet
- Newborn Journal PDFDocument8 pagesNewborn Journal PDFRose Ann ManalastasNo ratings yet
- NCM 109 MCN Semifinals Gestational ConditionsDocument6 pagesNCM 109 MCN Semifinals Gestational ConditionsQUEZON, BRITNEY KIM E.No ratings yet
- Uterine AtonyDocument4 pagesUterine AtonyKathleen Grace ManiagoNo ratings yet
- Drug Study: Brokenshire College Madapo, Davao CityDocument1 pageDrug Study: Brokenshire College Madapo, Davao CityHera Pamela Buelis BatoyNo ratings yet
- Unang Yakap Reflection EssayDocument3 pagesUnang Yakap Reflection EssayAnna ClarisaNo ratings yet
- Drug StudyDocument30 pagesDrug StudytonnifritzcutamoraNo ratings yet
- The Expanded Program On ImmunizationDocument4 pagesThe Expanded Program On Immunizationapi-3745792100% (3)
- Public Health Nurse Nursing ProceduresDocument9 pagesPublic Health Nurse Nursing ProcedureskzbreakerrNo ratings yet
- Case Study Group 2 Chapter 21Document4 pagesCase Study Group 2 Chapter 21Arnold ZamoroNo ratings yet
- What Is Diphtheria?Document2 pagesWhat Is Diphtheria?Luna WhiteNo ratings yet
- Guided Answers For NCM 109 Oral RevalidaDocument6 pagesGuided Answers For NCM 109 Oral RevalidaBenedict Reyes, Jr.No ratings yet
- And Vaginal Bleeding (In Ruptured Ectopic Pregnancy)Document9 pagesAnd Vaginal Bleeding (In Ruptured Ectopic Pregnancy)Clareen JuanicoNo ratings yet
- Meconium Aspiration Syndrome: DR Bob KlajoDocument17 pagesMeconium Aspiration Syndrome: DR Bob KlajoBob John100% (1)
- A. Dystocia: Problems With PowerDocument48 pagesA. Dystocia: Problems With PowerPauline GarciaNo ratings yet
- PoliomyelitisDocument4 pagesPoliomyelitisGerard Adad Misa100% (1)
- OXYTOCINDocument2 pagesOXYTOCINPang ProjectNo ratings yet
- Module 2Document11 pagesModule 2mirai desuNo ratings yet
- Drug-Study HydrocortisoneDocument4 pagesDrug-Study HydrocortisoneChristian Neil PonceNo ratings yet
- The 7 Immunizable Diseases AreDocument2 pagesThe 7 Immunizable Diseases Areclarheena100% (1)
- Journal Gadar Choking-Managing The Risk of Choking GuidelinesDocument18 pagesJournal Gadar Choking-Managing The Risk of Choking GuidelinesnurulNo ratings yet
- FNCPDocument14 pagesFNCPhelloaNo ratings yet
- 2.0 Community-Health-Survey-11aDocument8 pages2.0 Community-Health-Survey-11aCassey CuregNo ratings yet
- FNCP SampleDocument1 pageFNCP SampleAngela YbañezNo ratings yet
- Neonatal HyperbilirubinemiaDocument22 pagesNeonatal HyperbilirubinemiaAnkur WadheraNo ratings yet
- Stages of Labor Nursing Intervention: First StageDocument3 pagesStages of Labor Nursing Intervention: First StageJhanniel IreneaNo ratings yet
- Summary of Nursing Care of A Family With A ToddlerDocument3 pagesSummary of Nursing Care of A Family With A ToddlerKarly Alissa TarubalNo ratings yet
- Anti Tetanus Serum IDocument2 pagesAnti Tetanus Serum IRobby EffendyNo ratings yet
- Nurses NotesDocument2 pagesNurses NotesSVPSNo ratings yet
- Administration of Pneumococcal VaccineDocument24 pagesAdministration of Pneumococcal VaccineJay AdamzNo ratings yet
- BAIAE in Pregnancy.Document6 pagesBAIAE in Pregnancy.Mark Arthur MartinezNo ratings yet
- CATAINA, Maria Elizabeth D. - Case-scenario-DRDocument3 pagesCATAINA, Maria Elizabeth D. - Case-scenario-DRMarielle CatainaNo ratings yet
- Midterm CHNDocument12 pagesMidterm CHNTine SabaulanNo ratings yet
- Pathophy NCADocument1 pagePathophy NCAKaren ValdezNo ratings yet
- Impacts of Gmo'S On Genetically Modified Organisms Produced by Philippine ResearchersDocument3 pagesImpacts of Gmo'S On Genetically Modified Organisms Produced by Philippine ResearchersIrish Cheska EspinosaNo ratings yet
- Spontaneous AbortionDocument17 pagesSpontaneous Abortionanon_985338331No ratings yet
- Artificial Family Planning Methods Artificial Family Planning MethodsDocument33 pagesArtificial Family Planning Methods Artificial Family Planning MethodsJullienne Ysabelle AngNo ratings yet
- Performance Task 1Document4 pagesPerformance Task 1Casas, Jo-an Pauline A.No ratings yet
- College of Nursing: Ramon Magsaysay Memorial Medical Center, IncDocument1 pageCollege of Nursing: Ramon Magsaysay Memorial Medical Center, IncTERRENCE ANTHONY ANTONIONo ratings yet
- Ob Topic 3 - Multiple Pregnancy - NCPDocument2 pagesOb Topic 3 - Multiple Pregnancy - NCPThelly MargalloNo ratings yet
- Unit 6 Educational ApplicationsDocument10 pagesUnit 6 Educational ApplicationsBea Bianca CruzNo ratings yet
- The Organization of ShipDocument2 pagesThe Organization of ShipAmran HalimNo ratings yet
- Series & Parallel PumpsDocument48 pagesSeries & Parallel PumpsMoh AmmNo ratings yet
- Standard Operating Procedure: Planned Preventive MaintenanceDocument6 pagesStandard Operating Procedure: Planned Preventive MaintenanceMaryanthony NamyaloNo ratings yet
- TR2231 AVEVA Plant CAD Model Requirements Ver4Document29 pagesTR2231 AVEVA Plant CAD Model Requirements Ver4ASIMNo ratings yet
- Hampton Inn 5.20 2021 Public PacketDocument49 pagesHampton Inn 5.20 2021 Public PacketArielle BreenNo ratings yet
- DILO SF6 Catalogue 2021 ENDocument214 pagesDILO SF6 Catalogue 2021 ENBadraa BatorgilNo ratings yet
- Iveco EUROCARGO RANGEDocument3 pagesIveco EUROCARGO RANGEChe VarianNo ratings yet
- Creativity and InnovationDocument25 pagesCreativity and InnovationHarshaNo ratings yet
- 9 Level Hell DescriptionDocument2 pages9 Level Hell DescriptionRonald PachecoNo ratings yet
- Osha UthmDocument19 pagesOsha UthmWan Muhammad Faiz Bin Mohd RoslanNo ratings yet
- 预习内容:Chapter 3 Solving Radical EquationsDocument15 pages预习内容:Chapter 3 Solving Radical EquationsSolo YehNo ratings yet
- StorageTek Tape Libraries Entry-Level and Midrange Help Desk Support ConsultantDocument36 pagesStorageTek Tape Libraries Entry-Level and Midrange Help Desk Support ConsultantAngel Lacerna CórdovaNo ratings yet
- Fracture CrurisDocument44 pagesFracture CrurisAnonymous turPUJtErNo ratings yet
- Instruction Manual Pygmy Current Meter Model Oss-Pc1: Hyquest Solutions Pty LTDDocument17 pagesInstruction Manual Pygmy Current Meter Model Oss-Pc1: Hyquest Solutions Pty LTDTomás Londoño GarcíaNo ratings yet
- Man of Sorrows PDFDocument4 pagesMan of Sorrows PDFjoao.beckNo ratings yet
- C149-14 Standard Test Method For Thermal Shock Resistance of Glass ContainersDocument3 pagesC149-14 Standard Test Method For Thermal Shock Resistance of Glass ContainersAhmed AlzubaidiNo ratings yet
- Guidelines Current List Updated March 2019Document9 pagesGuidelines Current List Updated March 2019MehrdadNo ratings yet
- Eaton Handheld DiagnosticsDocument15 pagesEaton Handheld DiagnosticsEboni DanielsNo ratings yet
- Resource Tracking Scenario For SAP Transportation Management PDFDocument30 pagesResource Tracking Scenario For SAP Transportation Management PDFsaptmNo ratings yet
- 04 BuyLog2017 Safety Switches July-DSDocument37 pages04 BuyLog2017 Safety Switches July-DSMohamedAbdElrhmanNo ratings yet
- Light Dependant ResisterDocument10 pagesLight Dependant ResisterAyush PattnaikNo ratings yet
- Plant Guide MaldivaDocument34 pagesPlant Guide MaldivaDaisy100% (1)
- Experiment 1 Solubility of Organic CompoundsDocument5 pagesExperiment 1 Solubility of Organic CompoundsKirstin Blaire MagdadaroNo ratings yet
- Effects Temp On PropsDocument5 pagesEffects Temp On Propsdina gunasekeraNo ratings yet
- Reservation List As of June 27Document104 pagesReservation List As of June 27Francis DedumoNo ratings yet
- 4.3 Bone TissueDocument80 pages4.3 Bone TissueManjunathNo ratings yet
- Module 8 Neo BehaviorismDocument11 pagesModule 8 Neo BehaviorismDenyseNo ratings yet
- CHEM 112.1 - Exer 5 NewDocument7 pagesCHEM 112.1 - Exer 5 NewGerry Mark GubantesNo ratings yet
- New Process For Production of Trah Ydro UranDocument9 pagesNew Process For Production of Trah Ydro UranGreten TreutelNo ratings yet
- The Real ChristDocument185 pagesThe Real ChristDuncan HeasterNo ratings yet