
Collins1 5
Collins1 5
You might also like
- Strovac Prospect EnglishDocument6 pagesStrovac Prospect EnglishSorin Rusu75% (4)
- ASCO-SEP Sixth EditionDocument1,434 pagesASCO-SEP Sixth Editionshona nag100% (3)
- The Fundamentals of CaregivingDocument23 pagesThe Fundamentals of CaregivingRaisa Gravador100% (2)
- Agwaga - Flobel Final Work-1Document49 pagesAgwaga - Flobel Final Work-1davidtitangohNo ratings yet
- Knowledge and Attitude Towards Pregnancy Induced Hypertension Among Pregnant Women Attending Antenatal at Kampala International University Teaching HospitalDocument71 pagesKnowledge and Attitude Towards Pregnancy Induced Hypertension Among Pregnant Women Attending Antenatal at Kampala International University Teaching HospitalBALUKU YOSIAH0% (1)
- Best Practice Guideline - Color-Coded Syringe Labeling of AnesthesDocument44 pagesBest Practice Guideline - Color-Coded Syringe Labeling of AnesthesAdira AyuNo ratings yet
- Chellah Final Research (2) EditedDocument56 pagesChellah Final Research (2) EditedCredible Technology ComplexNo ratings yet
- Mburu - Evaluation of The Clinical Learning ExperiencesDocument88 pagesMburu - Evaluation of The Clinical Learning ExperiencesMutiat Muhammed FunmilolaNo ratings yet
- Kwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFDocument93 pagesKwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFNoraNo ratings yet
- Kerbina Michael Ndomba ProposalDocument35 pagesKerbina Michael Ndomba ProposalNyagawa GodkNo ratings yet
- Root Canal TreatmentDocument24 pagesRoot Canal TreatmentNamutala NangoyiNo ratings yet
- Research On Breast Self ExaminationDocument46 pagesResearch On Breast Self ExaminationDISNEY CYBERNo ratings yet
- Joseline Proposal Finale (RepairedDocument22 pagesJoseline Proposal Finale (RepairedMwebaza JoshuaNo ratings yet
- Alice Research (Final)Document57 pagesAlice Research (Final)Timothy MakoriNo ratings yet
- Final Research Project 2022 Richard SakalaDocument40 pagesFinal Research Project 2022 Richard SakalaRichard SakalaNo ratings yet
- Biology ResearchDocument25 pagesBiology ResearchGELANA DAMESANo ratings yet
- JEDIDA PROJECT TYPING COMPLETE FinalDocument33 pagesJEDIDA PROJECT TYPING COMPLETE FinalBernard MbeviNo ratings yet
- Imende John Modified RESEARCHDocument45 pagesImende John Modified RESEARCHFAN PAGE CYBERNo ratings yet
- Chinenye, Nwankwo Mercy PHD PH, 2018.CORRECTEDDocument221 pagesChinenye, Nwankwo Mercy PHD PH, 2018.CORRECTEDtanmai nooluNo ratings yet
- Study To Determine Awareness On Self Breast Examination Among Women of Reproductive AgeDocument47 pagesStudy To Determine Awareness On Self Breast Examination Among Women of Reproductive Agealvinouma27No ratings yet
- Effect of Nutrition Education...Document123 pagesEffect of Nutrition Education...KeneniNo ratings yet
- Shawa ThesisDocument103 pagesShawa ThesisAdamNo ratings yet
- Elyne Osodo Research ProposalDocument29 pagesElyne Osodo Research Proposalken osodoNo ratings yet
- PRELIMSDocument10 pagesPRELIMSUmar Farouq Mohammed GalibNo ratings yet
- Kimuyu - Factors Associated With Adherence To AntihypertensiveDocument76 pagesKimuyu - Factors Associated With Adherence To AntihypertensiveJOHN MUTUNENo ratings yet
- Kiragu - Maternal Knowledge and Practice of Porridge Preparation and Storage in The HomeDocument58 pagesKiragu - Maternal Knowledge and Practice of Porridge Preparation and Storage in The HomeAngel GustasianaNo ratings yet
- Gwamaka SamsonDocument73 pagesGwamaka SamsonSaami MalikNo ratings yet
- Flavia Research ProjectDocument42 pagesFlavia Research Projectjohn mwambuNo ratings yet
- Research Proposal-ERICK J CHILAMULADocument28 pagesResearch Proposal-ERICK J CHILAMULAErick JohnNo ratings yet
- Maternity Healthcare For Patients With Gestational DiabetesDocument59 pagesMaternity Healthcare For Patients With Gestational DiabetesManish MahajanNo ratings yet
- Malaria and Bacterial Co-InfectionsDocument94 pagesMalaria and Bacterial Co-InfectionsStephanie AndersonNo ratings yet
- Pregnant Women's Experiences With Gastrointestinal Discomforts and Strategies They Use To CopeDocument167 pagesPregnant Women's Experiences With Gastrointestinal Discomforts and Strategies They Use To Copekamaljit kaurNo ratings yet
- Kibua - Childcare Practices and Nutritional Status of Children Under Five Years Old in Southland Informal Settlement Nairobi CountyDocument116 pagesKibua - Childcare Practices and Nutritional Status of Children Under Five Years Old in Southland Informal Settlement Nairobi CountymaryNo ratings yet
- Food Handling Hygiene and Sanitation Practices in The Child-Car PDFDocument271 pagesFood Handling Hygiene and Sanitation Practices in The Child-Car PDFLance Giello DuzonNo ratings yet
- Shadrack Muma ThesisDocument74 pagesShadrack Muma ThesisJune BellNo ratings yet
- Claris Final ResearchDocument42 pagesClaris Final Researcholiver wekesaNo ratings yet
- Final Thesis Otieno Churchill OchiengDocument102 pagesFinal Thesis Otieno Churchill OchiengOtieno Churchill OchiengNo ratings yet
- Fredrick Ogumbo's Post Defence Thesis Final Binding Copy V PDFDocument63 pagesFredrick Ogumbo's Post Defence Thesis Final Binding Copy V PDFloliweduduNo ratings yet
- Ansila Mbunda ProposalDocument34 pagesAnsila Mbunda ProposalNyagawa GodkNo ratings yet
- Proposal B. INGGRISDocument17 pagesProposal B. INGGRISsyafiraazlyn01No ratings yet
- The Diffusion of Telehealth: System-Level Conditions For Successful Adoption by Danika TynesDocument159 pagesThe Diffusion of Telehealth: System-Level Conditions For Successful Adoption by Danika TynesDanika TynesNo ratings yet
- RESEARCHDocument62 pagesRESEARCHAbdulbasit DamilolaNo ratings yet
- FINAL COPY DorotthyDocument184 pagesFINAL COPY Dorotthypk9459285No ratings yet
- Effects of BPCRDocument87 pagesEffects of BPCRRajaNo ratings yet
- PeggyDocument144 pagesPeggyWomayi SamsonNo ratings yet
- Improving The Quality of Decentralization in Ugfanda: The Unfinished BusinessDocument13 pagesImproving The Quality of Decentralization in Ugfanda: The Unfinished Businessagri sonicNo ratings yet
- Abortion in Kiambu County.Document30 pagesAbortion in Kiambu County.Joshua Marissah NaftaliNo ratings yet
- Project CompleteDocument57 pagesProject CompleteMWANGINo ratings yet
- Factors Contributing To High Occurances of Malaria in Children Under Five Years at Bukulula Health Centre Iv in Kalungu DistrictDocument53 pagesFactors Contributing To High Occurances of Malaria in Children Under Five Years at Bukulula Health Centre Iv in Kalungu Districtarthurvikings44No ratings yet
- Ndyabagye Samson Research ReportDocument56 pagesNdyabagye Samson Research ReportAYO NELSONNo ratings yet
- Work On Prvalence StudiesDocument87 pagesWork On Prvalence Studieschelsea pasiahNo ratings yet
- Adeliana Joseph KJDocument29 pagesAdeliana Joseph KJNyagawa GodkNo ratings yet
- Zainab K. Barrie Oct. 2023Document66 pagesZainab K. Barrie Oct. 2023Zainab k BarrieNo ratings yet
- Manya ThesisDocument87 pagesManya ThesisDesalegn Dereje100% (1)
- Research Proposal and Thesis. 24,2Document29 pagesResearch Proposal and Thesis. 24,2Hillary MutugiNo ratings yet
- Factors Influencing Patients Willingness To Participate in Their Nursing Care A Study at The Nsawam Government HospitalDocument99 pagesFactors Influencing Patients Willingness To Participate in Their Nursing Care A Study at The Nsawam Government HospitalEugene AsanteNo ratings yet
- Biwott PROJECT COMPLETE-1Document57 pagesBiwott PROJECT COMPLETE-1MWANGINo ratings yet
- Erick ReportDocument29 pagesErick ReportErick JohnNo ratings yet
- KNOWLEDGE AND ALTITUDE ON THE USE OF INTRAUTERINE COPPER DEVICE IUD AMONG WOMEN ATTENDING MCHFP CLINIC IN EMBU LEVEL 5 HOSPITAL Maureen CompleteDocument37 pagesKNOWLEDGE AND ALTITUDE ON THE USE OF INTRAUTERINE COPPER DEVICE IUD AMONG WOMEN ATTENDING MCHFP CLINIC IN EMBU LEVEL 5 HOSPITAL Maureen CompleteTWIN SISTERSNo ratings yet
- Kenya Medical Training CollegeDocument39 pagesKenya Medical Training CollegeTWIN SISTERSNo ratings yet
- Conroy2018 PHDDocument262 pagesConroy2018 PHDogunwoleisrael1No ratings yet
- Medical School for Everyone: Grand Rounds Cases (Transcript)From EverandMedical School for Everyone: Grand Rounds Cases (Transcript)Rating: 4.5 out of 5 stars4.5/5 (2)
- Uncovering Student Ideas in Life Science, Volume 1: 25 New Formative Assessment ProbesFrom EverandUncovering Student Ideas in Life Science, Volume 1: 25 New Formative Assessment ProbesNo ratings yet
- Charles Addo (Motivational Essay)Document7 pagesCharles Addo (Motivational Essay)Kwablah TettehNo ratings yet
- Effective Presentation SkillsDocument13 pagesEffective Presentation SkillsKwablah TettehNo ratings yet
- How To Resolve Conflicts in MarriageDocument27 pagesHow To Resolve Conflicts in MarriageKwablah TettehNo ratings yet
- BiographyDocument8 pagesBiographyKwablah TettehNo ratings yet
- Project ProposalDocument4 pagesProject ProposalAngel Faith TirolNo ratings yet
- Does Social Class Affect Your Mental Health - PPTX 1Document16 pagesDoes Social Class Affect Your Mental Health - PPTX 1karah13No ratings yet
- SanaDocument2 pagesSanaYaseen RehmaniNo ratings yet
- Testosterone Therapy Fact SheetDocument2 pagesTestosterone Therapy Fact SheetJonathan CastroNo ratings yet
- Readiness LevelDocument10 pagesReadiness LevelsrpattabbiramanNo ratings yet
- Hospital Monitoring, Setting and Training For Home NIVDocument4 pagesHospital Monitoring, Setting and Training For Home NIVPaoly PalmaNo ratings yet
- CB 5 Review Test 2 Answer KeyDocument2 pagesCB 5 Review Test 2 Answer KeyKeluarga SuksesNo ratings yet
- NURSING CARE PLAN FOR CROHN'sDocument2 pagesNURSING CARE PLAN FOR CROHN'sMuhyeeSalaIdjadNo ratings yet
- Influenza in Brazil: Surveillance Pathways: Regional ReviewDocument11 pagesInfluenza in Brazil: Surveillance Pathways: Regional ReviewThaís Nunes dos AnjosNo ratings yet
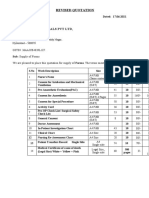
- Brungi Hospital QuotationDocument2 pagesBrungi Hospital QuotationPurchase PNo ratings yet
- Mission 2Document6 pagesMission 2kailash chand atalNo ratings yet
- Reporte de The Boston Consulting Group Sobre El PerúDocument44 pagesReporte de The Boston Consulting Group Sobre El PerúAlejandro Castro BackusNo ratings yet
- Asuhan Kebidanan Ibu Bersalin Pada Ny. T G P A Hamil 41 Minggu Dengan Induksi Atas Indikasi Postdate Di VK Rsud SurakartaDocument11 pagesAsuhan Kebidanan Ibu Bersalin Pada Ny. T G P A Hamil 41 Minggu Dengan Induksi Atas Indikasi Postdate Di VK Rsud SurakartaLevi aotNo ratings yet
- Chew National Exam Past QuestionsDocument4 pagesChew National Exam Past QuestionsMuhammad Mahmood100% (3)
- CodeofEthics ANA 2010Document198 pagesCodeofEthics ANA 2010Oluz WangiNo ratings yet
- Mba 1 in PDFDocument41 pagesMba 1 in PDFtheshoeslover1No ratings yet
- Lecture 6 PharmacyDocument31 pagesLecture 6 PharmacykkumarNo ratings yet
- Final Asthma EssayDocument12 pagesFinal Asthma Essayapi-609379126No ratings yet
- Dental Management of Handicapped ChildrenDocument18 pagesDental Management of Handicapped ChildrenDrBhawna AroraNo ratings yet
- Ictm Hospital Information System (Week 10)Document4 pagesIctm Hospital Information System (Week 10)Ray Anne Rose MadlaNo ratings yet
- H. Clinical Laboratory Laws (Technical Standards)Document15 pagesH. Clinical Laboratory Laws (Technical Standards)Armie Joy ManingatNo ratings yet
- NURS FPX 6416 Assessment 2 Technology Needs Assessment Summary and Implementation PlanDocument4 pagesNURS FPX 6416 Assessment 2 Technology Needs Assessment Summary and Implementation PlanCarolyn HarkerNo ratings yet
- PT Pis: Deskripsi Barang Harga SatuanDocument42 pagesPT Pis: Deskripsi Barang Harga SatuanAndi MufidahNo ratings yet
- Time For A Change?: 1. Consider Likes and DislikesDocument2 pagesTime For A Change?: 1. Consider Likes and DislikesEMILY LAVERGNENo ratings yet
- 1 PBDocument7 pages1 PBAriadne OliveiraNo ratings yet
- Medication Errors in AnaesthesiaDocument49 pagesMedication Errors in AnaesthesiaVithal Dhulkhed100% (1)
- CG3 - Administration of Medicine GuidelinesDocument7 pagesCG3 - Administration of Medicine GuidelinesFarcasanu Liana GeorgianaNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- Strovac Prospect EnglishDocument6 pagesStrovac Prospect EnglishSorin Rusu75% (4)
- ASCO-SEP Sixth EditionDocument1,434 pagesASCO-SEP Sixth Editionshona nag100% (3)
- The Fundamentals of CaregivingDocument23 pagesThe Fundamentals of CaregivingRaisa Gravador100% (2)
- Agwaga - Flobel Final Work-1Document49 pagesAgwaga - Flobel Final Work-1davidtitangohNo ratings yet
- Knowledge and Attitude Towards Pregnancy Induced Hypertension Among Pregnant Women Attending Antenatal at Kampala International University Teaching HospitalDocument71 pagesKnowledge and Attitude Towards Pregnancy Induced Hypertension Among Pregnant Women Attending Antenatal at Kampala International University Teaching HospitalBALUKU YOSIAH0% (1)
- Best Practice Guideline - Color-Coded Syringe Labeling of AnesthesDocument44 pagesBest Practice Guideline - Color-Coded Syringe Labeling of AnesthesAdira AyuNo ratings yet
- Chellah Final Research (2) EditedDocument56 pagesChellah Final Research (2) EditedCredible Technology ComplexNo ratings yet
- Mburu - Evaluation of The Clinical Learning ExperiencesDocument88 pagesMburu - Evaluation of The Clinical Learning ExperiencesMutiat Muhammed FunmilolaNo ratings yet
- Kwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFDocument93 pagesKwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFNoraNo ratings yet
- Kerbina Michael Ndomba ProposalDocument35 pagesKerbina Michael Ndomba ProposalNyagawa GodkNo ratings yet
- Root Canal TreatmentDocument24 pagesRoot Canal TreatmentNamutala NangoyiNo ratings yet
- Research On Breast Self ExaminationDocument46 pagesResearch On Breast Self ExaminationDISNEY CYBERNo ratings yet
- Joseline Proposal Finale (RepairedDocument22 pagesJoseline Proposal Finale (RepairedMwebaza JoshuaNo ratings yet
- Alice Research (Final)Document57 pagesAlice Research (Final)Timothy MakoriNo ratings yet
- Final Research Project 2022 Richard SakalaDocument40 pagesFinal Research Project 2022 Richard SakalaRichard SakalaNo ratings yet
- Biology ResearchDocument25 pagesBiology ResearchGELANA DAMESANo ratings yet
- JEDIDA PROJECT TYPING COMPLETE FinalDocument33 pagesJEDIDA PROJECT TYPING COMPLETE FinalBernard MbeviNo ratings yet
- Imende John Modified RESEARCHDocument45 pagesImende John Modified RESEARCHFAN PAGE CYBERNo ratings yet
- Chinenye, Nwankwo Mercy PHD PH, 2018.CORRECTEDDocument221 pagesChinenye, Nwankwo Mercy PHD PH, 2018.CORRECTEDtanmai nooluNo ratings yet
- Study To Determine Awareness On Self Breast Examination Among Women of Reproductive AgeDocument47 pagesStudy To Determine Awareness On Self Breast Examination Among Women of Reproductive Agealvinouma27No ratings yet
- Effect of Nutrition Education...Document123 pagesEffect of Nutrition Education...KeneniNo ratings yet
- Shawa ThesisDocument103 pagesShawa ThesisAdamNo ratings yet
- Elyne Osodo Research ProposalDocument29 pagesElyne Osodo Research Proposalken osodoNo ratings yet
- PRELIMSDocument10 pagesPRELIMSUmar Farouq Mohammed GalibNo ratings yet
- Kimuyu - Factors Associated With Adherence To AntihypertensiveDocument76 pagesKimuyu - Factors Associated With Adherence To AntihypertensiveJOHN MUTUNENo ratings yet
- Kiragu - Maternal Knowledge and Practice of Porridge Preparation and Storage in The HomeDocument58 pagesKiragu - Maternal Knowledge and Practice of Porridge Preparation and Storage in The HomeAngel GustasianaNo ratings yet
- Gwamaka SamsonDocument73 pagesGwamaka SamsonSaami MalikNo ratings yet
- Flavia Research ProjectDocument42 pagesFlavia Research Projectjohn mwambuNo ratings yet
- Research Proposal-ERICK J CHILAMULADocument28 pagesResearch Proposal-ERICK J CHILAMULAErick JohnNo ratings yet
- Maternity Healthcare For Patients With Gestational DiabetesDocument59 pagesMaternity Healthcare For Patients With Gestational DiabetesManish MahajanNo ratings yet
- Malaria and Bacterial Co-InfectionsDocument94 pagesMalaria and Bacterial Co-InfectionsStephanie AndersonNo ratings yet
- Pregnant Women's Experiences With Gastrointestinal Discomforts and Strategies They Use To CopeDocument167 pagesPregnant Women's Experiences With Gastrointestinal Discomforts and Strategies They Use To Copekamaljit kaurNo ratings yet
- Kibua - Childcare Practices and Nutritional Status of Children Under Five Years Old in Southland Informal Settlement Nairobi CountyDocument116 pagesKibua - Childcare Practices and Nutritional Status of Children Under Five Years Old in Southland Informal Settlement Nairobi CountymaryNo ratings yet
- Food Handling Hygiene and Sanitation Practices in The Child-Car PDFDocument271 pagesFood Handling Hygiene and Sanitation Practices in The Child-Car PDFLance Giello DuzonNo ratings yet
- Shadrack Muma ThesisDocument74 pagesShadrack Muma ThesisJune BellNo ratings yet
- Claris Final ResearchDocument42 pagesClaris Final Researcholiver wekesaNo ratings yet
- Final Thesis Otieno Churchill OchiengDocument102 pagesFinal Thesis Otieno Churchill OchiengOtieno Churchill OchiengNo ratings yet
- Fredrick Ogumbo's Post Defence Thesis Final Binding Copy V PDFDocument63 pagesFredrick Ogumbo's Post Defence Thesis Final Binding Copy V PDFloliweduduNo ratings yet
- Ansila Mbunda ProposalDocument34 pagesAnsila Mbunda ProposalNyagawa GodkNo ratings yet
- Proposal B. INGGRISDocument17 pagesProposal B. INGGRISsyafiraazlyn01No ratings yet
- The Diffusion of Telehealth: System-Level Conditions For Successful Adoption by Danika TynesDocument159 pagesThe Diffusion of Telehealth: System-Level Conditions For Successful Adoption by Danika TynesDanika TynesNo ratings yet
- RESEARCHDocument62 pagesRESEARCHAbdulbasit DamilolaNo ratings yet
- FINAL COPY DorotthyDocument184 pagesFINAL COPY Dorotthypk9459285No ratings yet
- Effects of BPCRDocument87 pagesEffects of BPCRRajaNo ratings yet
- PeggyDocument144 pagesPeggyWomayi SamsonNo ratings yet
- Improving The Quality of Decentralization in Ugfanda: The Unfinished BusinessDocument13 pagesImproving The Quality of Decentralization in Ugfanda: The Unfinished Businessagri sonicNo ratings yet
- Abortion in Kiambu County.Document30 pagesAbortion in Kiambu County.Joshua Marissah NaftaliNo ratings yet
- Project CompleteDocument57 pagesProject CompleteMWANGINo ratings yet
- Factors Contributing To High Occurances of Malaria in Children Under Five Years at Bukulula Health Centre Iv in Kalungu DistrictDocument53 pagesFactors Contributing To High Occurances of Malaria in Children Under Five Years at Bukulula Health Centre Iv in Kalungu Districtarthurvikings44No ratings yet
- Ndyabagye Samson Research ReportDocument56 pagesNdyabagye Samson Research ReportAYO NELSONNo ratings yet
- Work On Prvalence StudiesDocument87 pagesWork On Prvalence Studieschelsea pasiahNo ratings yet
- Adeliana Joseph KJDocument29 pagesAdeliana Joseph KJNyagawa GodkNo ratings yet
- Zainab K. Barrie Oct. 2023Document66 pagesZainab K. Barrie Oct. 2023Zainab k BarrieNo ratings yet
- Manya ThesisDocument87 pagesManya ThesisDesalegn Dereje100% (1)
- Research Proposal and Thesis. 24,2Document29 pagesResearch Proposal and Thesis. 24,2Hillary MutugiNo ratings yet
- Factors Influencing Patients Willingness To Participate in Their Nursing Care A Study at The Nsawam Government HospitalDocument99 pagesFactors Influencing Patients Willingness To Participate in Their Nursing Care A Study at The Nsawam Government HospitalEugene AsanteNo ratings yet
- Biwott PROJECT COMPLETE-1Document57 pagesBiwott PROJECT COMPLETE-1MWANGINo ratings yet
- Erick ReportDocument29 pagesErick ReportErick JohnNo ratings yet
- KNOWLEDGE AND ALTITUDE ON THE USE OF INTRAUTERINE COPPER DEVICE IUD AMONG WOMEN ATTENDING MCHFP CLINIC IN EMBU LEVEL 5 HOSPITAL Maureen CompleteDocument37 pagesKNOWLEDGE AND ALTITUDE ON THE USE OF INTRAUTERINE COPPER DEVICE IUD AMONG WOMEN ATTENDING MCHFP CLINIC IN EMBU LEVEL 5 HOSPITAL Maureen CompleteTWIN SISTERSNo ratings yet
- Kenya Medical Training CollegeDocument39 pagesKenya Medical Training CollegeTWIN SISTERSNo ratings yet
- Conroy2018 PHDDocument262 pagesConroy2018 PHDogunwoleisrael1No ratings yet
- Medical School for Everyone: Grand Rounds Cases (Transcript)From EverandMedical School for Everyone: Grand Rounds Cases (Transcript)Rating: 4.5 out of 5 stars4.5/5 (2)
- Uncovering Student Ideas in Life Science, Volume 1: 25 New Formative Assessment ProbesFrom EverandUncovering Student Ideas in Life Science, Volume 1: 25 New Formative Assessment ProbesNo ratings yet
- Charles Addo (Motivational Essay)Document7 pagesCharles Addo (Motivational Essay)Kwablah TettehNo ratings yet
- Effective Presentation SkillsDocument13 pagesEffective Presentation SkillsKwablah TettehNo ratings yet
- How To Resolve Conflicts in MarriageDocument27 pagesHow To Resolve Conflicts in MarriageKwablah TettehNo ratings yet
- BiographyDocument8 pagesBiographyKwablah TettehNo ratings yet
- Project ProposalDocument4 pagesProject ProposalAngel Faith TirolNo ratings yet
- Does Social Class Affect Your Mental Health - PPTX 1Document16 pagesDoes Social Class Affect Your Mental Health - PPTX 1karah13No ratings yet
- SanaDocument2 pagesSanaYaseen RehmaniNo ratings yet
- Testosterone Therapy Fact SheetDocument2 pagesTestosterone Therapy Fact SheetJonathan CastroNo ratings yet
- Readiness LevelDocument10 pagesReadiness LevelsrpattabbiramanNo ratings yet
- Hospital Monitoring, Setting and Training For Home NIVDocument4 pagesHospital Monitoring, Setting and Training For Home NIVPaoly PalmaNo ratings yet
- CB 5 Review Test 2 Answer KeyDocument2 pagesCB 5 Review Test 2 Answer KeyKeluarga SuksesNo ratings yet
- NURSING CARE PLAN FOR CROHN'sDocument2 pagesNURSING CARE PLAN FOR CROHN'sMuhyeeSalaIdjadNo ratings yet
- Influenza in Brazil: Surveillance Pathways: Regional ReviewDocument11 pagesInfluenza in Brazil: Surveillance Pathways: Regional ReviewThaís Nunes dos AnjosNo ratings yet
- Brungi Hospital QuotationDocument2 pagesBrungi Hospital QuotationPurchase PNo ratings yet
- Mission 2Document6 pagesMission 2kailash chand atalNo ratings yet
- Reporte de The Boston Consulting Group Sobre El PerúDocument44 pagesReporte de The Boston Consulting Group Sobre El PerúAlejandro Castro BackusNo ratings yet
- Asuhan Kebidanan Ibu Bersalin Pada Ny. T G P A Hamil 41 Minggu Dengan Induksi Atas Indikasi Postdate Di VK Rsud SurakartaDocument11 pagesAsuhan Kebidanan Ibu Bersalin Pada Ny. T G P A Hamil 41 Minggu Dengan Induksi Atas Indikasi Postdate Di VK Rsud SurakartaLevi aotNo ratings yet
- Chew National Exam Past QuestionsDocument4 pagesChew National Exam Past QuestionsMuhammad Mahmood100% (3)
- CodeofEthics ANA 2010Document198 pagesCodeofEthics ANA 2010Oluz WangiNo ratings yet
- Mba 1 in PDFDocument41 pagesMba 1 in PDFtheshoeslover1No ratings yet
- Lecture 6 PharmacyDocument31 pagesLecture 6 PharmacykkumarNo ratings yet
- Final Asthma EssayDocument12 pagesFinal Asthma Essayapi-609379126No ratings yet
- Dental Management of Handicapped ChildrenDocument18 pagesDental Management of Handicapped ChildrenDrBhawna AroraNo ratings yet
- Ictm Hospital Information System (Week 10)Document4 pagesIctm Hospital Information System (Week 10)Ray Anne Rose MadlaNo ratings yet
- H. Clinical Laboratory Laws (Technical Standards)Document15 pagesH. Clinical Laboratory Laws (Technical Standards)Armie Joy ManingatNo ratings yet
- NURS FPX 6416 Assessment 2 Technology Needs Assessment Summary and Implementation PlanDocument4 pagesNURS FPX 6416 Assessment 2 Technology Needs Assessment Summary and Implementation PlanCarolyn HarkerNo ratings yet
- PT Pis: Deskripsi Barang Harga SatuanDocument42 pagesPT Pis: Deskripsi Barang Harga SatuanAndi MufidahNo ratings yet
- Time For A Change?: 1. Consider Likes and DislikesDocument2 pagesTime For A Change?: 1. Consider Likes and DislikesEMILY LAVERGNENo ratings yet
- 1 PBDocument7 pages1 PBAriadne OliveiraNo ratings yet
- Medication Errors in AnaesthesiaDocument49 pagesMedication Errors in AnaesthesiaVithal Dhulkhed100% (1)
- CG3 - Administration of Medicine GuidelinesDocument7 pagesCG3 - Administration of Medicine GuidelinesFarcasanu Liana GeorgianaNo ratings yet