Download as docx, pdf, or txt
You might also like
- Fluid & Electrolytes Cheat Sheet v3Document1 pageFluid & Electrolytes Cheat Sheet v3faten100% (2)
- Case Study-Congestive Heart FailureDocument71 pagesCase Study-Congestive Heart FailureKentTangcalagan92% (13)
- System Disorder: Renal CalculiDocument1 pageSystem Disorder: Renal CalculiHolly DeckelmanNo ratings yet
- Manicure and PedicureDocument38 pagesManicure and PedicureDesiree Clarisse B. DelaCruz100% (4)
- Fluid & Electrolytes Cheat SheetDocument1 pageFluid & Electrolytes Cheat SheetGelyn Gaylon0% (1)
- Cheat Sheet For Fluid Balance and ElectrolytesDocument2 pagesCheat Sheet For Fluid Balance and ElectrolytesLiel TorresNo ratings yet
- Drug StudyDocument8 pagesDrug StudyZanie CruzNo ratings yet
- Hallmark Signs and Symptoms PDFDocument6 pagesHallmark Signs and Symptoms PDFjjNo ratings yet
- Daily Rounds in IcuDocument59 pagesDaily Rounds in IcutuulipNo ratings yet
- High Yield Surgery Compatible VersionDocument77 pagesHigh Yield Surgery Compatible VersionEdgar Soto100% (1)
- Generic: Hydromorphone (SC) Brand Name: DilaudidDocument1 pageGeneric: Hydromorphone (SC) Brand Name: DilaudidPreet ChahalNo ratings yet
- ChartingDocument1 pageChartingAdrianaMarreroNo ratings yet
- HeartFailure Nursing FIK 2014Document101 pagesHeartFailure Nursing FIK 2014Putri NurlaeliNo ratings yet
- Nursing Care of Clients With Upper Airway or Respiratory DisordersDocument6 pagesNursing Care of Clients With Upper Airway or Respiratory DisordersLuna MarieNo ratings yet
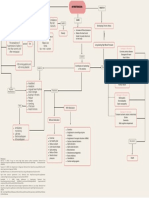
- Concept Map On HypertensionDocument1 pageConcept Map On Hypertensionleh XDNo ratings yet
- Nursing CS Wound DocumentationDocument1 pageNursing CS Wound DocumentationJazzmine GuraNo ratings yet
- F&E For Elderly - ModuleDocument163 pagesF&E For Elderly - ModuleArihk NiladaNo ratings yet
- This Study Resource Was: Student Name: - Section: - Date of Patient CareDocument2 pagesThis Study Resource Was: Student Name: - Section: - Date of Patient CareSashaNo ratings yet
- Common Abbreviations For The Patient Note USMLE Step 2CSDocument1 pageCommon Abbreviations For The Patient Note USMLE Step 2CSTiondi francisNo ratings yet
- Growth Hormone DisordersDocument1 pageGrowth Hormone DisordersVishalNo ratings yet
- Drug Study Drug Name Classificatio N Dosage/ Prepatarion Indication Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesDrug Study Drug Name Classificatio N Dosage/ Prepatarion Indication Contraindication Side Effects Nursing ResponsibilitiesTheresa AbrilloNo ratings yet
- Careplan 4Document16 pagesCareplan 4api-653800047No ratings yet
- 9 ECG Strips On The NCLEX: 1. Normal Sinus RhythmDocument4 pages9 ECG Strips On The NCLEX: 1. Normal Sinus RhythmH T (Ah Ki)No ratings yet
- Quiz 1 Med Surg SummerDocument8 pagesQuiz 1 Med Surg SummerMc Harris VinasoyNo ratings yet
- Module 4 - Cardiac EmergencyDocument30 pagesModule 4 - Cardiac EmergencyElaine AntonetteNo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Emergency Ortho BCS 2017Document80 pagesEmergency Ortho BCS 2017Priza Razunip100% (1)
- Sbar Template 08Document2 pagesSbar Template 08ayuNo ratings yet
- 145-Drug Calculations For Nurses A Step by Step Approach, 3rd Edition-Robert Lapham Heather AgarDocument265 pages145-Drug Calculations For Nurses A Step by Step Approach, 3rd Edition-Robert Lapham Heather AgarSULDAANUL CAASHIQIINNo ratings yet
- Chronic Renal FailureDocument7 pagesChronic Renal Failuretantalizin marieNo ratings yet
- Mohammed H. Eid - The Intensivist-Middle East & ElMarwa For Publishing & Distribution, GN (2019)Document372 pagesMohammed H. Eid - The Intensivist-Middle East & ElMarwa For Publishing & Distribution, GN (2019)Mohamed Moussa100% (1)
- Think Nursing! ReportDocument20 pagesThink Nursing! ReportRobert Fraser RNNo ratings yet
- Asthma - Diagnostics & CausesDocument1 pageAsthma - Diagnostics & CausesVishalNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NKatrinaJimenezNo ratings yet
- 4.3 InfectiousDocument29 pages4.3 InfectiousJohn Anthony de GùzmanNo ratings yet
- Dysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1onDocument4 pagesDysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1ontantalizin marieNo ratings yet
- Perioperative Nursing ReportDocument19 pagesPerioperative Nursing ReportPortia Dulce Patatag Toquero100% (1)
- 12 Drugs Acting On The Cardiovascular SystemDocument7 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- Pediatric NursingDocument146 pagesPediatric NursingJannele BernadasNo ratings yet
- Google Doc Mark K NCLEX Study GuideDocument36 pagesGoogle Doc Mark K NCLEX Study GuideSVPSNo ratings yet
- Assessment and Concept Map Care Plan For Critical Care PatientDocument11 pagesAssessment and Concept Map Care Plan For Critical Care Patientapi-604551723No ratings yet
- ABCDEF Bundle WebcastDocument42 pagesABCDEF Bundle WebcastsoulstakersNo ratings yet
- Pressure InjuriesDocument1 pagePressure InjuriesPaola OrtizNo ratings yet
- Chapter 6 Care of The Patient Experiencing Shock or Heart FailureDocument49 pagesChapter 6 Care of The Patient Experiencing Shock or Heart FailureJennifer KellerNo ratings yet
- Pneumonia Patho & SignsDocument1 pagePneumonia Patho & SignsVishalNo ratings yet
- Unfolding Reasoning Dementia Physical AggressionDocument7 pagesUnfolding Reasoning Dementia Physical AggressionnoslendadnarimNo ratings yet
- Med Cards Starting With A PDFDocument7 pagesMed Cards Starting With A PDFDonn Patrick AlegreNo ratings yet
- StrokeDocument1 pageStrokeMariel Febreo Merlan100% (1)
- Brain Sheet2011Document1 pageBrain Sheet2011nursekatieNo ratings yet
- OTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderDocument2 pagesOTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderAdocueNo ratings yet
- Cardiovascular & Hematologic SystemDocument163 pagesCardiovascular & Hematologic SystemRellie CastroNo ratings yet
- Introduction To Nursing PharmacologyDocument97 pagesIntroduction To Nursing PharmacologyLiel TorresNo ratings yet
- NCM 106 Midterm 1Document26 pagesNCM 106 Midterm 1JULIANNAH ATHENA MERCADONo ratings yet
- ASIA International Standards For Neurological Classification of Spinal Cord InjuryDocument2 pagesASIA International Standards For Neurological Classification of Spinal Cord InjuryMicah Tagle100% (1)
- Med Surg 2 - 2 Diagnostic Examinations For Gastrointestinal SystemDocument18 pagesMed Surg 2 - 2 Diagnostic Examinations For Gastrointestinal SystemMaxinne RoseñoNo ratings yet
- Sirs & ModsDocument5 pagesSirs & Modsmarlou agananNo ratings yet
- Head To Toe AssessmentDocument3 pagesHead To Toe Assessmentsandaman2225No ratings yet
- Med Surg Chapter 65 Flashcards - QuizletDocument17 pagesMed Surg Chapter 65 Flashcards - QuizletMonica JubaneNo ratings yet
- ArrythmiaDocument31 pagesArrythmialubnaNo ratings yet
- Last CareplanDocument22 pagesLast CareplanNneka Adaeze AnyanwuNo ratings yet
- Internet Tools For Advanced Nursing PracticeDocument17 pagesInternet Tools For Advanced Nursing PracticeCzey AnonatNo ratings yet
- Med Surg RevDocument14 pagesMed Surg RevSamantha VeraNo ratings yet
- Hematology System Problems WorksheetDocument7 pagesHematology System Problems WorksheetJennNo ratings yet
- Anemia & Leukemia NotesDocument6 pagesAnemia & Leukemia NotesJennNo ratings yet
- PNUR 251 Homeostasis S 2022Document56 pagesPNUR 251 Homeostasis S 2022JennNo ratings yet
- Class 1Document3 pagesClass 1JennNo ratings yet
- Final NotesDocument19 pagesFinal NotesJennNo ratings yet
- CH 41 LBP - Braddom's Physical Medicine & RehabilitationDocument46 pagesCH 41 LBP - Braddom's Physical Medicine & RehabilitationPyrectic WilliamsNo ratings yet
- Get The Story of Offshore Arctic Engineering 1st Edition Dan Masterson PDF Full ChapterDocument24 pagesGet The Story of Offshore Arctic Engineering 1st Edition Dan Masterson PDF Full Chapterglantzyraola100% (8)
- Flu Virus American English Student BWDocument3 pagesFlu Virus American English Student BWNathalia Robles OrtizNo ratings yet
- Week 13 CD COURSE TASK 7. Dengue Fever, Filariasis, Malaria and EncephalitisDocument5 pagesWeek 13 CD COURSE TASK 7. Dengue Fever, Filariasis, Malaria and EncephalitisRogelyn PatriarcaNo ratings yet
- Mystery Respiratory Illness, Greenspring Near Fort Detrick (July 2019) - CDC No ResultDocument4 pagesMystery Respiratory Illness, Greenspring Near Fort Detrick (July 2019) - CDC No ResultKevin SteinerNo ratings yet
- Clinical Aspects and Health Benefits of Ginger Zingiber Officinale in Both Traditional Chinese Medicine and Modern IndustryDocument12 pagesClinical Aspects and Health Benefits of Ginger Zingiber Officinale in Both Traditional Chinese Medicine and Modern IndustryWarungSimbahSecangNo ratings yet
- 2021 Essential Brain Hygiene EguideDocument26 pages2021 Essential Brain Hygiene EguideHector SolarNo ratings yet
- Health Medicine 2Document5 pagesHealth Medicine 2omaradnanNo ratings yet
- Thomas G Plante (Ed.) - Abnormal Psychology Across The Ages-Praeger (2013)Document872 pagesThomas G Plante (Ed.) - Abnormal Psychology Across The Ages-Praeger (2013)TARUSHI KAURNo ratings yet
- Deep Neck InfectionsDocument9 pagesDeep Neck InfectionsfayzaNo ratings yet
- Bahasa Inggris Kelas 6Document4 pagesBahasa Inggris Kelas 6Nia Asih KurniasariNo ratings yet
- Speaking For Difficult Patient Oet MaterialsDocument2 pagesSpeaking For Difficult Patient Oet MaterialsThae Wint100% (2)
- SP100 Hazard Identification ParanDocument10 pagesSP100 Hazard Identification ParanErine ParanNo ratings yet
- Root Cause Analysis To IdentifDocument17 pagesRoot Cause Analysis To IdentifDina AryaniNo ratings yet
- PIDSR VPD SurveillanceDocument89 pagesPIDSR VPD SurveillanceMichelle TuraNo ratings yet
- PROMETRIC EXAM 23/11/2016: A. MalyringingDocument8 pagesPROMETRIC EXAM 23/11/2016: A. MalyringingTrycNo ratings yet
- Sea Remedies PowerpointDocument19 pagesSea Remedies PowerpointDr. Smita MahajanNo ratings yet
- Funda ExamDocument21 pagesFunda ExamFebykates Egos-RafisuraNo ratings yet
- Blueprints PsychiatryDocument432 pagesBlueprints PsychiatryFiona Fleming87% (15)
- ToS & Ospe Final Year MbbsDocument99 pagesToS & Ospe Final Year MbbsAdnanNo ratings yet
- LeukoeritroblastikDocument2 pagesLeukoeritroblastiknadaNo ratings yet
- PESTEL AnalysisDocument7 pagesPESTEL AnalysiszenerdiodeNo ratings yet
- Trichomonas Vaginalis NCPDocument2 pagesTrichomonas Vaginalis NCP3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- The Carbon Butterfly Innovative Entrepren - Yaniv IzakiDocument39 pagesThe Carbon Butterfly Innovative Entrepren - Yaniv IzakifabchatNo ratings yet
- Psychiatric Adverse Effects of AntibioticsDocument9 pagesPsychiatric Adverse Effects of AntibioticszorplNo ratings yet
- Accidents RiddorDocument8 pagesAccidents RiddorSafrina RamadhaniNo ratings yet
- Chlamydia SPP: Angelica Barbosa BuitragoDocument23 pagesChlamydia SPP: Angelica Barbosa BuitragoLeo LopezNo ratings yet
- Bilirubin: Reference RangeDocument6 pagesBilirubin: Reference Rangeal ghiffari muhammad rayhanNo ratings yet