Download as docx, pdf, or txt
You might also like
- Bangalore PeenyaDocument4 pagesBangalore Peenyaravishankar78% (9)
- Anemia: Ch. 31 Hematologic ProblemsDocument36 pagesAnemia: Ch. 31 Hematologic Problemshops23100% (3)
- Chapter 14 Red Blood CellsDocument37 pagesChapter 14 Red Blood CellsCatherine LiuNo ratings yet
- Blood Disorders - HandoutDocument8 pagesBlood Disorders - Handoutapi-335571917100% (1)
- 26 Manuals 3338, Anti-Aircraft Ammunition PDFDocument129 pages26 Manuals 3338, Anti-Aircraft Ammunition PDFKosta_g100% (1)
- Internship Survival Guide NSHDocument36 pagesInternship Survival Guide NSHRichardNo ratings yet
- Bryant Plus 80Document1 pageBryant Plus 80LouCypher100% (3)
- Peds HemeImmune OUTLINEDocument10 pagesPeds HemeImmune OUTLINEAshleyNo ratings yet
- Aplastic Hemolitic 2021 OlgaDocument43 pagesAplastic Hemolitic 2021 OlgalaibaNo ratings yet
- Anemia Nursing Care Plan: Presented by Edi Purwanto School of Nursing University of Muhammadiyah MalangDocument26 pagesAnemia Nursing Care Plan: Presented by Edi Purwanto School of Nursing University of Muhammadiyah MalangSevina Eka ChannelNo ratings yet
- Ha I by AbdifatahDocument109 pagesHa I by AbdifatahAbdifatah AhmedNo ratings yet
- Saint Luke's College Of: NursingDocument5 pagesSaint Luke's College Of: NursingApril Mae Magos LabradorNo ratings yet
- Interferences With Diffusion: AnemiaDocument49 pagesInterferences With Diffusion: AnemiaMaryAnn ElizabethNo ratings yet
- Hematology 1Document61 pagesHematology 1katz_hotchickNo ratings yet
- Kuliah AnemiaaDocument44 pagesKuliah AnemiaaAhmad Umar AfNo ratings yet
- III. FINAL Nursing Care of Clients With Disturbances in Male Female Reproduction Sexuality EditedVersionDocument26 pagesIII. FINAL Nursing Care of Clients With Disturbances in Male Female Reproduction Sexuality EditedVersionKurt PepitoNo ratings yet
- Anemia DIC NotesDocument6 pagesAnemia DIC NotesJeanna ChongNo ratings yet
- Anemia NotesDocument6 pagesAnemia NotesElstella Eguavoen Ehicheoya100% (2)
- Hemolytic AnemiaDocument99 pagesHemolytic AnemiaSagar Chandrakant Mhetre100% (3)
- Interpretive Summary: Nucleated RBCDocument2 pagesInterpretive Summary: Nucleated RBCWael SafwatNo ratings yet
- HaematologyDocument62 pagesHaematologyManmeet SNo ratings yet
- SBRC HematologyOncology 1Document80 pagesSBRC HematologyOncology 1dalia khamoNo ratings yet
- Hematologic System, Oncologic Disorders & Anemias: Oded Sumarna M KepDocument68 pagesHematologic System, Oncologic Disorders & Anemias: Oded Sumarna M KepUlfalutfiaNo ratings yet
- Saint Luke's College Of: NursingDocument6 pagesSaint Luke's College Of: NursingApril Mae Magos LabradorNo ratings yet
- Anemia and Red Blood Cell Disorder Lecture by Dr. Rosales (Nov 6, 2017)Document7 pagesAnemia and Red Blood Cell Disorder Lecture by Dr. Rosales (Nov 6, 2017)Ian Gabrielle Mercado CuynoNo ratings yet
- Hematology: Jan Bazner-Chandler CPNP, CNS, MSN, RNDocument80 pagesHematology: Jan Bazner-Chandler CPNP, CNS, MSN, RNWarrenPeaceNo ratings yet
- Hemolytic AnemiaDocument9 pagesHemolytic AnemiaTheeya QuigaoNo ratings yet
- RBC DISORDERS StudentsDocument84 pagesRBC DISORDERS Studentskimberly abianNo ratings yet
- Hematology HematopoiesisDocument69 pagesHematology HematopoiesisSharmin Nahar NabilaNo ratings yet
- Aematology: Col Kamran AfzalDocument32 pagesAematology: Col Kamran AfzalZaraNo ratings yet
- Red Blood Cell DisordersDocument56 pagesRed Blood Cell DisordersMunawar Adhar100% (4)
- 2 - Alterations in Oxygenation 1.1Document309 pages2 - Alterations in Oxygenation 1.1geng gengNo ratings yet
- Approach To Anemia: Bisrat DDocument45 pagesApproach To Anemia: Bisrat Dyared getachewNo ratings yet
- 21 Anaemia and PancytopeniaDocument42 pages21 Anaemia and PancytopeniaLeon Hui MingNo ratings yet
- PejowebApproach To Anemia by Dr. Joel Solorzani RomeroDocument57 pagesPejowebApproach To Anemia by Dr. Joel Solorzani RomeroAshraf FaragNo ratings yet
- Stages of ShockDocument13 pagesStages of ShockA. P.No ratings yet
- Presentation 1Document73 pagesPresentation 1ابراهيم محمدNo ratings yet
- DR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDocument30 pagesDR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDabogski FranceNo ratings yet
- DR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDocument30 pagesDR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDabogski FranceNo ratings yet
- Study Guide Hematologic AssessmentDocument5 pagesStudy Guide Hematologic AssessmentNancy LemusNo ratings yet
- Introduction To HematologyDocument23 pagesIntroduction To HematologyReba PhiliposeNo ratings yet
- Hemolytic AnemiaDocument6 pagesHemolytic AnemiaLupita Yessica Tarigan0% (1)
- Hematopoietic System PathologyDocument78 pagesHematopoietic System PathologyNuhu SibaNo ratings yet
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Lecture 3Document11 pagesLecture 3Jireh Vien AtienzaNo ratings yet
- Peripheral Smear Examination PDFDocument91 pagesPeripheral Smear Examination PDFtufis02100% (1)
- Clinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDocument24 pagesClinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDzil FikriNo ratings yet
- Kelainan Darah 1 FKG 2020Document74 pagesKelainan Darah 1 FKG 2020Jeremy Kartika SoeryonoNo ratings yet
- Aplastic Anemia Is A NormocyticDocument17 pagesAplastic Anemia Is A NormocyticAfrio ArismanNo ratings yet
- Hem OncDocument26 pagesHem OncJim XieNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- AnemiaDocument63 pagesAnemiaShyam RajNo ratings yet
- Nursing Management For Patients With Hematology Problems PDFDocument44 pagesNursing Management For Patients With Hematology Problems PDFAnggie AnggriyanaNo ratings yet
- Anemia DM-1 - REV.Document44 pagesAnemia DM-1 - REV.abdulrahmanbelewa96No ratings yet
- Tutori - Anemia MhsDocument38 pagesTutori - Anemia Mhszaky ariandyNo ratings yet
- Anemia in SurgeryDocument29 pagesAnemia in SurgeryEdwin OkonNo ratings yet
- Adult Nursing (NUR 316) : King Saud University College of NursingDocument45 pagesAdult Nursing (NUR 316) : King Saud University College of NursingNgh JanuarNo ratings yet
- How To Interpret HEMATOLOGY Test ResultsDocument36 pagesHow To Interpret HEMATOLOGY Test Resultssylvia haryantoNo ratings yet
- Red Blood Cells PathologyDocument47 pagesRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- ALLDocument18 pagesALLpritidinda3070No ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportFrom EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNo ratings yet
- Hematology System Problems WorksheetDocument7 pagesHematology System Problems WorksheetJennNo ratings yet
- PNUR 251 Homeostasis S 2022Document56 pagesPNUR 251 Homeostasis S 2022JennNo ratings yet
- Class 1Document3 pagesClass 1JennNo ratings yet
- Electrolytes (3607)Document11 pagesElectrolytes (3607)JennNo ratings yet
- Final NotesDocument19 pagesFinal NotesJennNo ratings yet
- Kirloskar Brothers LimitedDocument36 pagesKirloskar Brothers Limitedgopalakrishnannrm1202No ratings yet
- Concept of Disaster Risk Reduction and ManagementDocument2 pagesConcept of Disaster Risk Reduction and ManagementPrincess BalquinNo ratings yet
- Grade 9: Tle-He Cookery Perform Mise en PlaceDocument8 pagesGrade 9: Tle-He Cookery Perform Mise en PlaceIrine IrineNo ratings yet
- Journal of The American Oriental Society Vol 40Document898 pagesJournal of The American Oriental Society Vol 40Helen2015No ratings yet
- Pathology Lecture 2, Cell Injury (Notes/tafree3')Document18 pagesPathology Lecture 2, Cell Injury (Notes/tafree3')Ali Al-Qudsi100% (3)
- 07 - ATA-38 - E170 - 86pgsDocument86 pages07 - ATA-38 - E170 - 86pgsAlexander Mcfarlane100% (1)
- AREVA T&D Product RangeDocument10 pagesAREVA T&D Product RangeEduardo SolanoNo ratings yet
- Violence Against WomenDocument81 pagesViolence Against WomenOxfamNo ratings yet
- KonectDocument2 pagesKonectHellen DuNo ratings yet
- Mondelez International Inc (PackDocument33 pagesMondelez International Inc (PackPrashik MendheNo ratings yet
- Articulo 1 Indirect Ecological Interactions in The Rhizosphere PDFDocument28 pagesArticulo 1 Indirect Ecological Interactions in The Rhizosphere PDFRUBEN SANTIAGO ARIAS AGUDELONo ratings yet
- Gun Water PDFDocument4 pagesGun Water PDFAlejandro MontecilloNo ratings yet
- Operation FloodDocument4 pagesOperation FloodbhuvaneshkmrsNo ratings yet
- The Survey of Plant KingdomDocument28 pagesThe Survey of Plant KingdomkerryNo ratings yet
- Fluorescence SpectrosDocument52 pagesFluorescence Spectroshafsa BNo ratings yet
- Shell Alvania EPD: Performance, Features & Benefits Main ApplicationsDocument2 pagesShell Alvania EPD: Performance, Features & Benefits Main ApplicationsGrupo Bajío HidalgoNo ratings yet
- Functional Safety and IEC 61508 A Basic Guide PDFDocument9 pagesFunctional Safety and IEC 61508 A Basic Guide PDFfitasmounirNo ratings yet
- Lista de Exercicios Reported Speech 786250Document3 pagesLista de Exercicios Reported Speech 786250Ricardo SazaNo ratings yet
- Read The Following Text Written by Jacquie Mccarnan and Answer The Questions On The RightDocument1 pageRead The Following Text Written by Jacquie Mccarnan and Answer The Questions On The RightBuzila Cristina0% (1)
- Act Critical Skills List Aug 20Document3 pagesAct Critical Skills List Aug 20RobertNo ratings yet
- WantedDocument4 pagesWantedMansoor TheenNo ratings yet
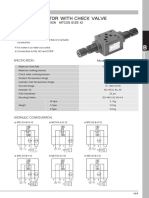
- MTC 03 W Throttle Check ValveDocument4 pagesMTC 03 W Throttle Check Valve박준용No ratings yet
- Life Cycle of FunariaDocument3 pagesLife Cycle of FunariaPalash Ghosh100% (1)
- Resume 2017Document2 pagesResume 2017api-370590770No ratings yet
- Design of Material Handling System For SpecificDocument14 pagesDesign of Material Handling System For SpecificKaran Virbhadre100% (3)
- Hidayah, N., A. N. Al-Baarri, Dan C. BudiartiDocument6 pagesHidayah, N., A. N. Al-Baarri, Dan C. Budiartiaulia rahmahNo ratings yet