Download as pdf or txt
You might also like
- Thibarmy Program Fat LossDocument18 pagesThibarmy Program Fat LossWilliam Spratling86% (14)
- Oral Revalida Emergencies 2017 ScriptDocument86 pagesOral Revalida Emergencies 2017 ScriptMara Medina - Borleo100% (7)
- POLYGRAPHYDocument12 pagesPOLYGRAPHYKhimber Claire Lala MaduyoNo ratings yet
- Cardiovascular NCLEX QuestionsDocument33 pagesCardiovascular NCLEX QuestionsPatricia VasquezNo ratings yet
- Veterinary Neurologic Rehabilitation The Rationale For ADocument9 pagesVeterinary Neurologic Rehabilitation The Rationale For ACarolina Vargas VélezNo ratings yet
- Management of Spasticity After Spinal Cord Injury: Current Techniques and Future DirectionsDocument11 pagesManagement of Spasticity After Spinal Cord Injury: Current Techniques and Future DirectionslabsoneducationNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptAchenk BarcelonistaNo ratings yet
- Spasticity After SCI PDFDocument10 pagesSpasticity After SCI PDFNovaria PuspitaNo ratings yet
- Influence of Myofacial Release and Stretching To Relieve Spasticity in Patients With Stroke - A Systematic ReviewDocument5 pagesInfluence of Myofacial Release and Stretching To Relieve Spasticity in Patients With Stroke - A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Art 3Document17 pagesArt 3ALEJANDRA GARZÓN CUELLAR.No ratings yet
- Physio Shacklock 95Document8 pagesPhysio Shacklock 95Raihan HabibNo ratings yet
- Nihms 1583867Document48 pagesNihms 1583867RONALDO ABDALLANo ratings yet
- NeurodinamycDocument7 pagesNeurodinamycDANAE AYALANo ratings yet
- Bhimani - Clinical Understanding of SpasticityDocument10 pagesBhimani - Clinical Understanding of SpasticityFriendlymeNo ratings yet
- Neurodynamic Mobilization and Peripheral Nerve Regeneration: A Narrative ReviewDocument8 pagesNeurodynamic Mobilization and Peripheral Nerve Regeneration: A Narrative Reviewadam.stenmanNo ratings yet
- 0 2021 Jacky Ganguly, Dinkar Kulshreshtha, Mohammed AlmotiriDocument21 pages0 2021 Jacky Ganguly, Dinkar Kulshreshtha, Mohammed AlmotiriLinaMaría CarreñoParraNo ratings yet
- Muscle Tone PhysiologyDocument21 pagesMuscle Tone PhysiologySagar SangoleNo ratings yet
- Accepted Manuscript: 10.1016/j.jpain.2015.08.008Document30 pagesAccepted Manuscript: 10.1016/j.jpain.2015.08.008Ayat BissNo ratings yet
- InterDocument17 pagesInterNita YulindaNo ratings yet
- Kelompok 2Document23 pagesKelompok 2lutfiah nabilahNo ratings yet
- Fphys 06 00240Document14 pagesFphys 06 00240elbueno21No ratings yet
- 01 STR 0000105386 05173 5eDocument7 pages01 STR 0000105386 05173 5eAmelito Miguel AndayaNo ratings yet
- Brain Research Bulletin: ReviewDocument22 pagesBrain Research Bulletin: ReviewCarlosNo ratings yet
- 2017 Article 1793Document5 pages2017 Article 1793annisaNo ratings yet
- Nerve Entrapment - UpdateDocument17 pagesNerve Entrapment - UpdatealobrienNo ratings yet
- 2010 - Rehabilitation Procedures in The Management of Spasti PDFDocument17 pages2010 - Rehabilitation Procedures in The Management of Spasti PDFEmmanuel RamosNo ratings yet
- Asj 2020 0146Document6 pagesAsj 2020 0146Mandeep JangraNo ratings yet
- Muscle Tone Physiology and Abnormalities (2021)Document20 pagesMuscle Tone Physiology and Abnormalities (2021)andresNo ratings yet
- Physiotherapeutic Intervention in A Patient With Spinal Cord Injury (SCI) .Document7 pagesPhysiotherapeutic Intervention in A Patient With Spinal Cord Injury (SCI) .eka aningNo ratings yet
- Jurnal 3Document27 pagesJurnal 3Anisa FirdausNo ratings yet
- Fdocuments - in - The Puzzle of Pain Loss of Mobility Evasive Movements The Puzzle of PainDocument21 pagesFdocuments - in - The Puzzle of Pain Loss of Mobility Evasive Movements The Puzzle of PainMARIA TERAPEUTANo ratings yet
- Efficacy of Contra-Lateral Neurodynamics On Median Nerve Extensibility in Cervical Radiculopathy PatientsDocument6 pagesEfficacy of Contra-Lateral Neurodynamics On Median Nerve Extensibility in Cervical Radiculopathy PatientsSylvia Grace100% (1)
- 2023 Vahdatpour Effectiveness - of - TECAR - Therapy - On CTCDocument10 pages2023 Vahdatpour Effectiveness - of - TECAR - Therapy - On CTCXavier ArmengouNo ratings yet
- SASSO 2020 - PBM in Sciatic Nerve Crush Injuries in Rodents - A SR and Perspectives For Clinical TreatmentDocument13 pagesSASSO 2020 - PBM in Sciatic Nerve Crush Injuries in Rodents - A SR and Perspectives For Clinical TreatmentMauricio ZeniNo ratings yet
- Peripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeDocument13 pagesPeripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeRafael MoreiraNo ratings yet
- The Nervous System, The Muscular System, and The Effects of Stroke On ThemDocument6 pagesThe Nervous System, The Muscular System, and The Effects of Stroke On ThemCyril MatisNo ratings yet
- J Clinph 2005 04 020Document11 pagesJ Clinph 2005 04 020Andres Rojas JerezNo ratings yet
- Bishop 2017Document10 pagesBishop 2017Mahdi HosseiniNo ratings yet
- Clinical Neurodynamics and Sports Medicine: Origins and DevelopmentDocument8 pagesClinical Neurodynamics and Sports Medicine: Origins and DevelopmentWahid NasrudinNo ratings yet
- Muscle Tone and JoinDocument12 pagesMuscle Tone and JoinomarihuanoNo ratings yet
- Introduction To Neuro Rehabilitation and Restorative Neurology (Article) Author Milan R DimitrijevicDocument3 pagesIntroduction To Neuro Rehabilitation and Restorative Neurology (Article) Author Milan R DimitrijevicPredrag NikolicNo ratings yet
- 2016 Effect of Laser Acupuncture On Heart Rate Variability of Nonpatients and Patients With Spinal Cord InjuryDocument2 pages2016 Effect of Laser Acupuncture On Heart Rate Variability of Nonpatients and Patients With Spinal Cord Injuryenfermeironilson6321No ratings yet
- Spasticity NeurologyDocument10 pagesSpasticity NeurologySamuel BodoarcaNo ratings yet
- Beda Efek Mirror Therapy Dengan Proprioceptive Neuromuscular Facilitation Dalam Meningkatkan Fungsional Anggota Gerak Atas Pada Pasien PascastrokeDocument10 pagesBeda Efek Mirror Therapy Dengan Proprioceptive Neuromuscular Facilitation Dalam Meningkatkan Fungsional Anggota Gerak Atas Pada Pasien PascastrokeTabita WidyasariNo ratings yet
- Cortical Mechanisms in MigraineDocument14 pagesCortical Mechanisms in MigraineLoida CamargoNo ratings yet
- Hypothalamus and Amygdala Response To Acupuncture StimuliDocument13 pagesHypothalamus and Amygdala Response To Acupuncture StimuliAnibal CisternasNo ratings yet
- Clinical Biomechanics: 10.1016/j.clinbiomech.2014.07.006Document35 pagesClinical Biomechanics: 10.1016/j.clinbiomech.2014.07.006camilaNo ratings yet
- Butler's Neuromobilizations Combined With Proprioceptive Neuromuscular Facilitation Are Effective in Reducing of Upper Limb Sensory in Late-Stage Stroke Subjects: A Three-Group Randomized TrialDocument12 pagesButler's Neuromobilizations Combined With Proprioceptive Neuromuscular Facilitation Are Effective in Reducing of Upper Limb Sensory in Late-Stage Stroke Subjects: A Three-Group Randomized TrialCarmen Menaya FernandezNo ratings yet
- Clinical Neurophysiology: Derek M. Miller, James F. Baker, W. Zev RymerDocument9 pagesClinical Neurophysiology: Derek M. Miller, James F. Baker, W. Zev RymerMiguelNo ratings yet
- Spinal Manipulative Therapy and Somatosensory ActivationDocument21 pagesSpinal Manipulative Therapy and Somatosensory ActivationAlan KipperNo ratings yet
- Maynard 2023Document13 pagesMaynard 2023Ram KNo ratings yet
- Neurophysiological Effects of Spinal Manipulation: Joel G. Pickar, DC, PHDDocument15 pagesNeurophysiological Effects of Spinal Manipulation: Joel G. Pickar, DC, PHDAnonymous ZmRV6WqNo ratings yet
- PR Ujian Neuro AuliaDocument10 pagesPR Ujian Neuro AuliaAULIA ANGRAININo ratings yet
- 2014 Addressing Neuroplastic Changes in Distributed Areas of The Nervous System Associated With Chronic Musculoskeletal DisordersDocument10 pages2014 Addressing Neuroplastic Changes in Distributed Areas of The Nervous System Associated With Chronic Musculoskeletal DisordersCristian OyarzoNo ratings yet
- Nerve InjuryDocument7 pagesNerve Injuryzwecker4458No ratings yet
- Original Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global OutcomeDocument6 pagesOriginal Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global Outcomeasep budiyantoNo ratings yet
- Sensorimotor Training A Global Approach For BalancDocument9 pagesSensorimotor Training A Global Approach For BalancVizaNo ratings yet
- Mejrh 134171Document9 pagesMejrh 134171Amazonia clinicaNo ratings yet
- JCM 11 03739 v2Document19 pagesJCM 11 03739 v2Edher Benitez PliegoNo ratings yet
- The Effects of Spinal Mobilizations On The Sympathetic NervousDocument8 pagesThe Effects of Spinal Mobilizations On The Sympathetic NervousbesombespierreNo ratings yet
- Spinal Cord InjuryDocument18 pagesSpinal Cord InjuryLaura AlvarezNo ratings yet
- VibrationDocument11 pagesVibrationFernando BrantalikNo ratings yet
- Spasticity: March 5 2017 Cherry Junn, MDDocument49 pagesSpasticity: March 5 2017 Cherry Junn, MDMarius DorinNo ratings yet
- Asop 06 0640Document4 pagesAsop 06 0640Ihsanul Ma'arifNo ratings yet
- PDF Ukm Penyuluhan Covid Hafiz CompressDocument7 pagesPDF Ukm Penyuluhan Covid Hafiz CompressIhsanul Ma'arifNo ratings yet
- Coagulopathy in COVID-19: Manifestations and Management: Cme MocDocument8 pagesCoagulopathy in COVID-19: Manifestations and Management: Cme MocIhsanul Ma'arifNo ratings yet
- 1628 4012 1 PBDocument13 pages1628 4012 1 PBIhsanul Ma'arifNo ratings yet
- Uncommon Variants of Fixed Drug Eruption PDFDocument7 pagesUncommon Variants of Fixed Drug Eruption PDFIhsanul Ma'arifNo ratings yet
- UntitledDocument2 pagesUntitledIhsanul Ma'arifNo ratings yet
- 4Document16 pages4Ihsanul Ma'arifNo ratings yet
- Toward Universal Donor Blood: Enzymatic Conversion of A AndbtootypeDocument10 pagesToward Universal Donor Blood: Enzymatic Conversion of A AndbtootypeIhsanul Ma'arifNo ratings yet
- C085222001#SITTI MASITA MOKOAGOW#Ilmu Patologi Klinik-1Document2 pagesC085222001#SITTI MASITA MOKOAGOW#Ilmu Patologi Klinik-1Ihsanul Ma'arifNo ratings yet
- Review Article: Human ABO Blood Groups and Their Associations With Different DiseasesDocument9 pagesReview Article: Human ABO Blood Groups and Their Associations With Different DiseasesIhsanul Ma'arifNo ratings yet
- Continuing Education Activity: ABO Blood Group SystemDocument5 pagesContinuing Education Activity: ABO Blood Group SystemIhsanul Ma'arifNo ratings yet
- TENRIDocument6 pagesTENRIIhsanul Ma'arifNo ratings yet
- C135221004 - Alfitra HalilDocument20 pagesC135221004 - Alfitra HalilIhsanul Ma'arifNo ratings yet
- Bebas KariesDocument21 pagesBebas KariesIhsanul Ma'arifNo ratings yet
- Chlampah, Journal Edit CR ParkinsonDocument8 pagesChlampah, Journal Edit CR ParkinsonIhsanul Ma'arifNo ratings yet
- Kerley's LineDocument3 pagesKerley's LineCitie VillaNo ratings yet
- Physiological Modeling - Final Project (Circulatory System)Document18 pagesPhysiological Modeling - Final Project (Circulatory System)Joshua DamianNo ratings yet
- Cells of Immune System Notes 2Document70 pagesCells of Immune System Notes 2Sudeeksha Ravikoti100% (1)
- Unit 4 Circulatory SystemDocument157 pagesUnit 4 Circulatory SystemChandan ShahNo ratings yet
- Bio Respiration Chapter SummaryDocument2 pagesBio Respiration Chapter SummaryYoussef Abdurrahman WeinmanNo ratings yet
- 5th Form Biology-Movement in Plants-TropismsDocument25 pages5th Form Biology-Movement in Plants-TropismsJharell CaravlhoNo ratings yet
- Module 2 - Symptoms and Syndromes in Diseases of Internal OrgansDocument133 pagesModule 2 - Symptoms and Syndromes in Diseases of Internal OrgansХассан ЯасирNo ratings yet
- Lower Respiratory DiseasesDocument137 pagesLower Respiratory DiseasesVictor StevenNo ratings yet
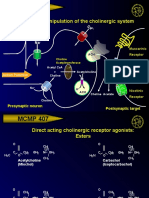
- MCMP 407: Pharmacologic Manipulation of The Cholinergic SystemDocument13 pagesMCMP 407: Pharmacologic Manipulation of The Cholinergic System16_dev5038No ratings yet
- Hypokalemia Disease AmnaDocument5 pagesHypokalemia Disease AmnaIzhar AhmadNo ratings yet
- Muscles Lab Report - NoDocument3 pagesMuscles Lab Report - Noapi-3801039No ratings yet
- Csec Biology TestDocument8 pagesCsec Biology TestImmanuel LashleyNo ratings yet
- Mid Test FK, Bahasa Inggris 1, Ang.2021Document2 pagesMid Test FK, Bahasa Inggris 1, Ang.2021Ary MfNo ratings yet
- Dopamine DRUG STUDY-ENDODocument3 pagesDopamine DRUG STUDY-ENDOaaron tabernaNo ratings yet
- Stem 12 H.O.P.E Module 1Document4 pagesStem 12 H.O.P.E Module 1Kari SuNo ratings yet
- Intradialitic HypotensionDocument7 pagesIntradialitic HypotensionanitaNo ratings yet
- Ventilator Hyperinflation by Physiotherapists Guideline - Bunbury HospitalDocument8 pagesVentilator Hyperinflation by Physiotherapists Guideline - Bunbury HospitalCarolina Rosa MartinsNo ratings yet
- اسئلتيDocument9 pagesاسئلتيahmedNo ratings yet
- Aj L3 CHD Qs & Ms Q1.: Diagram 1 Shows A Section Through The Heart. Diagram 1Document9 pagesAj L3 CHD Qs & Ms Q1.: Diagram 1 Shows A Section Through The Heart. Diagram 1IntelaNo ratings yet
- Unit 2 - AP Classroom Video HW SheetDocument8 pagesUnit 2 - AP Classroom Video HW SheetAubrey HovanNo ratings yet
- Grade 11 Irritability, Sensitivity and CoordinationDocument94 pagesGrade 11 Irritability, Sensitivity and CoordinationAsawni McDowellNo ratings yet
- BIO 9.3 - HomeworkDocument4 pagesBIO 9.3 - HomeworkalradilaylaNo ratings yet
- Human Body - A Visual Encyclopedia (PDFDrive) - 69-71Document3 pagesHuman Body - A Visual Encyclopedia (PDFDrive) - 69-71Neeha NMNo ratings yet
- Organisation of The Organism PDFDocument79 pagesOrganisation of The Organism PDFrachit100% (2)
- Blood Tests Glomerular Filtration Rate (GFR)Document2 pagesBlood Tests Glomerular Filtration Rate (GFR)Jane FlorendoNo ratings yet
- Dehydration Secondary To Diarrhea - NPDDocument3 pagesDehydration Secondary To Diarrhea - NPDLovely Grace PoreNo ratings yet