
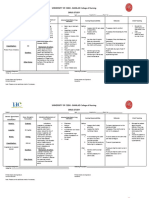
Nursing Diagnosis Acute Pain
Nursing Diagnosis Acute Pain
You might also like
- A Bridge To Wiseman Comprehension Questions Fixed VersionDocument12 pagesA Bridge To Wiseman Comprehension Questions Fixed Versionkizzytoy45No ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial Infarctionmariejo95% (125)
- Head Injury Assessment Tool - LNR PDFDocument4 pagesHead Injury Assessment Tool - LNR PDFvishwamedhi100% (1)
- Barnhill 2001Document9 pagesBarnhill 2001Lia C CriscoulloNo ratings yet
- C Post Concussion ChecklistDocument1 pageC Post Concussion Checklistalston96No ratings yet
- Appendectomy NCP GarganianDocument8 pagesAppendectomy NCP GarganianMa. Therese GarganianNo ratings yet
- DPE 101 Foundations of Education 1 Activity 2 Conditioning Theories For Teddy StoddardDocument4 pagesDPE 101 Foundations of Education 1 Activity 2 Conditioning Theories For Teddy StoddardAl Jay MejosNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing Diagnosislovelove DayoNo ratings yet
- D.2. PlanningDocument24 pagesD.2. PlanningAirene Gonzales SantiagoNo ratings yet
- Appendix 1: Healthy Students Healthy LivesDocument3 pagesAppendix 1: Healthy Students Healthy Livesempower93 empower93No ratings yet
- Sinonasal Outcome Test (SNOT) ScoreDocument1 pageSinonasal Outcome Test (SNOT) ScoreElfawizzyNo ratings yet
- Daily Concussion Symptom AssessmentDocument2 pagesDaily Concussion Symptom AssessmentAndrea RothNo ratings yet
- QoL - BD Full VersionDocument2 pagesQoL - BD Full Versiondwfz6b2cmjNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanRaphael Reyes Enriquez100% (1)
- HN43 EnglishDocument2 pagesHN43 EnglishAayush KapoorNo ratings yet
- Specimen Qlq-c30 EnglishDocument2 pagesSpecimen Qlq-c30 EnglishFenny KusumasariNo ratings yet
- New LongitudinalDocument2 pagesNew LongitudinalArijit DeyNo ratings yet
- 24 Chronic Pelvic Pain GuidelinesDocument132 pages24 Chronic Pelvic Pain Guidelinesclaumilena76No ratings yet
- Nursing diagnosis for pneumothoraxDocument1 pageNursing diagnosis for pneumothoraxJulia MendiolaNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionjamieboyRN88% (8)
- QLQ-C30 English PDFDocument2 pagesQLQ-C30 English PDFabi nayaNo ratings yet
- Philosophy Palliative Care and End of Life Care Per 15-02-2021Document33 pagesPhilosophy Palliative Care and End of Life Care Per 15-02-2021rizki ikhsanNo ratings yet
- Cuestionario FA12Document1 pageCuestionario FA12Julen Cruz QuiñonesNo ratings yet
- 1631 DN4 QuestionnaireDocument2 pages1631 DN4 QuestionnaireRaywa 217100% (1)
- Data AnalysisDocument8 pagesData AnalysisIndryNo ratings yet
- APA DSM5 Level 2 Depression Child Age 11 To 17Document3 pagesAPA DSM5 Level 2 Depression Child Age 11 To 17Eris TerryNo ratings yet
- IPOS Renal Paciente - SemanaDocument2 pagesIPOS Renal Paciente - SemanaUNEME HEMODIALISISNo ratings yet
- NCP Increased ICPDocument3 pagesNCP Increased ICPMa. Kaile Shyla LlacarNo ratings yet
- Bukidnon State University College of NursingDocument5 pagesBukidnon State University College of NursingAIZA MAE BANGGAY100% (1)
- Sympton Relief in Palliative Care PDFDocument300 pagesSympton Relief in Palliative Care PDFdjsalman25% (4)
- Breathing TAI - NijmegenFormDocument1 pageBreathing TAI - NijmegenFormLynseyNo ratings yet
- Head Nursing TemplateDocument9 pagesHead Nursing TemplateBianca MaeNo ratings yet
- Assessment Nursing Diagnosis Client Goal Outcome Criteria Nursing Interventions Rationale Actual EvaluationDocument10 pagesAssessment Nursing Diagnosis Client Goal Outcome Criteria Nursing Interventions Rationale Actual EvaluationDara Sophia EncarguezNo ratings yet
- Clinic 2nd Quarterly ReportDocument5 pagesClinic 2nd Quarterly ReportEunice Rosabel AbalosNo ratings yet
- Pharyngitis/Laryngitis: Subjective Cues: Short Term Outcome: Short Term OutcomeDocument2 pagesPharyngitis/Laryngitis: Subjective Cues: Short Term Outcome: Short Term OutcomefifiNo ratings yet
- Drug Study FORMDocument3 pagesDrug Study FORMJONICAJAM JAMORANo ratings yet
- Acute Pain TonsilitisncpDocument2 pagesAcute Pain Tonsilitisncpjustinekaye diongsonNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanScribdTranslationsNo ratings yet
- Dialysis Symptom Index: The University of Pittsburgh Medical CenterDocument4 pagesDialysis Symptom Index: The University of Pittsburgh Medical CenterMahir YousuffNo ratings yet
- Tonsilitis & Allergic Rhinitis NCPDocument11 pagesTonsilitis & Allergic Rhinitis NCPJorgia SalardaNo ratings yet
- Patient Survey (Qor - 40) : Part ADocument4 pagesPatient Survey (Qor - 40) : Part ARahadian MalikNo ratings yet
- NCP Colorectal CancerDocument4 pagesNCP Colorectal CancerWinnie AriolaNo ratings yet
- Rheumatoid Arthritis Nursing Care Plan PDFDocument3 pagesRheumatoid Arthritis Nursing Care Plan PDFIzhra MargateNo ratings yet
- Laporan Kimia Farma Maros 2 MeiDocument14 pagesLaporan Kimia Farma Maros 2 MeiSitti AsiaNo ratings yet
- Acute Pain (Cramps)Document5 pagesAcute Pain (Cramps)Fhey Bernadette BeltranNo ratings yet
- Reflux Severity Index (RSI) : 1 Month, How Did The FollowingDocument2 pagesReflux Severity Index (RSI) : 1 Month, How Did The FollowingAnak CarolusNo ratings yet
- Facilitator Handbook 1Document201 pagesFacilitator Handbook 1Sahil AnsariNo ratings yet
- Acute Pain Related To Hyper Secretion of Gastric Juices As Evidenced by Yellowish Vomitus and Pain Scale of 10/10Document2 pagesAcute Pain Related To Hyper Secretion of Gastric Juices As Evidenced by Yellowish Vomitus and Pain Scale of 10/10danaNo ratings yet
- Carpal Tunnel Syndrome Questionnaire (CTSQ)Document1 pageCarpal Tunnel Syndrome Questionnaire (CTSQ)Samuel Iñiguez JiménezNo ratings yet
- Jan 2023 Narrative ReportDocument6 pagesJan 2023 Narrative ReportSusan Loida SorianoNo ratings yet
- Chapter - Pain Assessment and ManagementDocument3 pagesChapter - Pain Assessment and ManagementrxNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionRocelyn CristobalNo ratings yet
- Chronic Pelvic PainDocument86 pagesChronic Pelvic PainRiean AuliaNo ratings yet
- Lesson Plan - Pain (Unit 4)Document28 pagesLesson Plan - Pain (Unit 4)Jincy JohnyNo ratings yet
- NCP Draft - Ectopic PregnancyDocument10 pagesNCP Draft - Ectopic PregnancyD CNo ratings yet
- NCP ExampleDocument2 pagesNCP ExampleLeady Joy MorboNo ratings yet
- Quality of Life QuestionnaireDocument4 pagesQuality of Life QuestionnaireJosé NetoNo ratings yet
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- PNCDocument2 pagesPNClovelove DayoNo ratings yet
- ASSESMENTFINALFINALDocument4 pagesASSESMENTFINALFINALlovelove DayoNo ratings yet
- Review InflamDocument17 pagesReview Inflamlovelove DayoNo ratings yet
- Lourlyn's Angels?Document27 pagesLourlyn's Angels?lovelove DayoNo ratings yet
- The Goal - Aim of-WPS OfficeDocument1 pageThe Goal - Aim of-WPS Officelovelove DayoNo ratings yet
- Significance of The Study and Research DesignDocument1 pageSignificance of The Study and Research Designlovelove DayoNo ratings yet
- Seizure Nursing ManagementDocument1 pageSeizure Nursing Managementlovelove DayoNo ratings yet
- Oral Revalida and Comprehensive ExamDocument13 pagesOral Revalida and Comprehensive Examlovelove DayoNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing Diagnosislovelove DayoNo ratings yet
- MAIN PROBLEM OF-WPS OfficeDocument1 pageMAIN PROBLEM OF-WPS Officelovelove DayoNo ratings yet
- Impact Evaluation IntroDocument12 pagesImpact Evaluation IntroKhuê TrầnNo ratings yet
- Fight, Flight, and FreezeDocument5 pagesFight, Flight, and FreezeLili SingerNo ratings yet
- Reading Practice 01: Just RelaxDocument14 pagesReading Practice 01: Just RelaxNg Thanh ChienNo ratings yet
- Emotional Intelligence Unit I EmotionDocument39 pagesEmotional Intelligence Unit I EmotionHema PriyaNo ratings yet
- Organizing Training of Young Football Players Initial StageDocument3 pagesOrganizing Training of Young Football Players Initial StageAcademic JournalNo ratings yet
- Chapter 3 Levenson. Coping With IllnessDocument40 pagesChapter 3 Levenson. Coping With Illnessjodalo.jdlrNo ratings yet
- MAPEH G-10 1st QuarterDocument11 pagesMAPEH G-10 1st QuarterGian Manzano SelidioNo ratings yet
- 3 Increasing Rejection of IntimaDocument27 pages3 Increasing Rejection of IntimaHan YeNo ratings yet
- Leadership AssessmentDocument9 pagesLeadership Assessmentchanceux 11No ratings yet
- What Is Happening To The Filipino Family?: Ma. Lourdes A. Carandang, PHDDocument24 pagesWhat Is Happening To The Filipino Family?: Ma. Lourdes A. Carandang, PHDAngel CarocheNo ratings yet
- Tweezer Dexterity by Saima KhanDocument6 pagesTweezer Dexterity by Saima KhanHmm OkNo ratings yet
- Long-Term Sickness Absence Due To Mental Disorders Is Associated With Individual Features and Psychosocial Work ConditionsDocument16 pagesLong-Term Sickness Absence Due To Mental Disorders Is Associated With Individual Features and Psychosocial Work ConditionsPollyanna Lavinia Lima RibeiroNo ratings yet
- Bashing Bobo: Introducing Psychological ResearchDocument7 pagesBashing Bobo: Introducing Psychological ResearchAera BangNo ratings yet
- Talk Show ScriptDocument4 pagesTalk Show ScriptJarey SalvalozaNo ratings yet
- The Happy Powder: Neurotransmitter SolutionDocument6 pagesThe Happy Powder: Neurotransmitter SolutionaligaramNo ratings yet
- 2010 ADA Standards For Accessible DesignDocument187 pages2010 ADA Standards For Accessible Designwera-delagarza3536No ratings yet
- Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th Edition Townsend Test BankDocument29 pagesPsychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th Edition Townsend Test BankMichaelJohnsonijybp100% (20)
- Freud, Luria and The Clinical Method: Mark SolmsDocument27 pagesFreud, Luria and The Clinical Method: Mark SolmsVALERIA AGUILAR100% (1)
- Training Your BrainDocument17 pagesTraining Your BrainRajeshNo ratings yet
- Meeting The Ethical Challenges of Leadership - Casting Lightor SHDocument5 pagesMeeting The Ethical Challenges of Leadership - Casting Lightor SHMKNo ratings yet
- CHAPTER 1-3 (1st Set)Document31 pagesCHAPTER 1-3 (1st Set)Jimmy LojaNo ratings yet
- A Systematic Review of The Outcome of Child Abuse in Long-Term CareDocument18 pagesA Systematic Review of The Outcome of Child Abuse in Long-Term CareBea100% (1)
- Intro To Meditation 4 Part Series Handouts Madison 201410Document10 pagesIntro To Meditation 4 Part Series Handouts Madison 201410Mahavidya KarunaNo ratings yet
- Chapter 6: Behavior Intervention Plans (Bip) : Learner OutcomesDocument70 pagesChapter 6: Behavior Intervention Plans (Bip) : Learner OutcomesSabiha BegumNo ratings yet
- Diss Sim 2020 Module 6 PDFDocument27 pagesDiss Sim 2020 Module 6 PDFJuvy MatabalanNo ratings yet
- Family and CommunityDocument46 pagesFamily and CommunityCez0408No ratings yet
- Welfare Checks and Therapeutic Risk Management.8Document5 pagesWelfare Checks and Therapeutic Risk Management.8Marco Dave Gutierrez ParedesNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- A Bridge To Wiseman Comprehension Questions Fixed VersionDocument12 pagesA Bridge To Wiseman Comprehension Questions Fixed Versionkizzytoy45No ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial Infarctionmariejo95% (125)
- Head Injury Assessment Tool - LNR PDFDocument4 pagesHead Injury Assessment Tool - LNR PDFvishwamedhi100% (1)
- Barnhill 2001Document9 pagesBarnhill 2001Lia C CriscoulloNo ratings yet
- C Post Concussion ChecklistDocument1 pageC Post Concussion Checklistalston96No ratings yet
- Appendectomy NCP GarganianDocument8 pagesAppendectomy NCP GarganianMa. Therese GarganianNo ratings yet
- DPE 101 Foundations of Education 1 Activity 2 Conditioning Theories For Teddy StoddardDocument4 pagesDPE 101 Foundations of Education 1 Activity 2 Conditioning Theories For Teddy StoddardAl Jay MejosNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing Diagnosislovelove DayoNo ratings yet
- D.2. PlanningDocument24 pagesD.2. PlanningAirene Gonzales SantiagoNo ratings yet
- Appendix 1: Healthy Students Healthy LivesDocument3 pagesAppendix 1: Healthy Students Healthy Livesempower93 empower93No ratings yet
- Sinonasal Outcome Test (SNOT) ScoreDocument1 pageSinonasal Outcome Test (SNOT) ScoreElfawizzyNo ratings yet
- Daily Concussion Symptom AssessmentDocument2 pagesDaily Concussion Symptom AssessmentAndrea RothNo ratings yet
- QoL - BD Full VersionDocument2 pagesQoL - BD Full Versiondwfz6b2cmjNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanRaphael Reyes Enriquez100% (1)
- HN43 EnglishDocument2 pagesHN43 EnglishAayush KapoorNo ratings yet
- Specimen Qlq-c30 EnglishDocument2 pagesSpecimen Qlq-c30 EnglishFenny KusumasariNo ratings yet
- New LongitudinalDocument2 pagesNew LongitudinalArijit DeyNo ratings yet
- 24 Chronic Pelvic Pain GuidelinesDocument132 pages24 Chronic Pelvic Pain Guidelinesclaumilena76No ratings yet
- Nursing diagnosis for pneumothoraxDocument1 pageNursing diagnosis for pneumothoraxJulia MendiolaNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionjamieboyRN88% (8)
- QLQ-C30 English PDFDocument2 pagesQLQ-C30 English PDFabi nayaNo ratings yet
- Philosophy Palliative Care and End of Life Care Per 15-02-2021Document33 pagesPhilosophy Palliative Care and End of Life Care Per 15-02-2021rizki ikhsanNo ratings yet
- Cuestionario FA12Document1 pageCuestionario FA12Julen Cruz QuiñonesNo ratings yet
- 1631 DN4 QuestionnaireDocument2 pages1631 DN4 QuestionnaireRaywa 217100% (1)
- Data AnalysisDocument8 pagesData AnalysisIndryNo ratings yet
- APA DSM5 Level 2 Depression Child Age 11 To 17Document3 pagesAPA DSM5 Level 2 Depression Child Age 11 To 17Eris TerryNo ratings yet
- IPOS Renal Paciente - SemanaDocument2 pagesIPOS Renal Paciente - SemanaUNEME HEMODIALISISNo ratings yet
- NCP Increased ICPDocument3 pagesNCP Increased ICPMa. Kaile Shyla LlacarNo ratings yet
- Bukidnon State University College of NursingDocument5 pagesBukidnon State University College of NursingAIZA MAE BANGGAY100% (1)
- Sympton Relief in Palliative Care PDFDocument300 pagesSympton Relief in Palliative Care PDFdjsalman25% (4)
- Breathing TAI - NijmegenFormDocument1 pageBreathing TAI - NijmegenFormLynseyNo ratings yet
- Head Nursing TemplateDocument9 pagesHead Nursing TemplateBianca MaeNo ratings yet
- Assessment Nursing Diagnosis Client Goal Outcome Criteria Nursing Interventions Rationale Actual EvaluationDocument10 pagesAssessment Nursing Diagnosis Client Goal Outcome Criteria Nursing Interventions Rationale Actual EvaluationDara Sophia EncarguezNo ratings yet
- Clinic 2nd Quarterly ReportDocument5 pagesClinic 2nd Quarterly ReportEunice Rosabel AbalosNo ratings yet
- Pharyngitis/Laryngitis: Subjective Cues: Short Term Outcome: Short Term OutcomeDocument2 pagesPharyngitis/Laryngitis: Subjective Cues: Short Term Outcome: Short Term OutcomefifiNo ratings yet
- Drug Study FORMDocument3 pagesDrug Study FORMJONICAJAM JAMORANo ratings yet
- Acute Pain TonsilitisncpDocument2 pagesAcute Pain Tonsilitisncpjustinekaye diongsonNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanScribdTranslationsNo ratings yet
- Dialysis Symptom Index: The University of Pittsburgh Medical CenterDocument4 pagesDialysis Symptom Index: The University of Pittsburgh Medical CenterMahir YousuffNo ratings yet
- Tonsilitis & Allergic Rhinitis NCPDocument11 pagesTonsilitis & Allergic Rhinitis NCPJorgia SalardaNo ratings yet
- Patient Survey (Qor - 40) : Part ADocument4 pagesPatient Survey (Qor - 40) : Part ARahadian MalikNo ratings yet
- NCP Colorectal CancerDocument4 pagesNCP Colorectal CancerWinnie AriolaNo ratings yet
- Rheumatoid Arthritis Nursing Care Plan PDFDocument3 pagesRheumatoid Arthritis Nursing Care Plan PDFIzhra MargateNo ratings yet
- Laporan Kimia Farma Maros 2 MeiDocument14 pagesLaporan Kimia Farma Maros 2 MeiSitti AsiaNo ratings yet
- Acute Pain (Cramps)Document5 pagesAcute Pain (Cramps)Fhey Bernadette BeltranNo ratings yet
- Reflux Severity Index (RSI) : 1 Month, How Did The FollowingDocument2 pagesReflux Severity Index (RSI) : 1 Month, How Did The FollowingAnak CarolusNo ratings yet
- Facilitator Handbook 1Document201 pagesFacilitator Handbook 1Sahil AnsariNo ratings yet
- Acute Pain Related To Hyper Secretion of Gastric Juices As Evidenced by Yellowish Vomitus and Pain Scale of 10/10Document2 pagesAcute Pain Related To Hyper Secretion of Gastric Juices As Evidenced by Yellowish Vomitus and Pain Scale of 10/10danaNo ratings yet
- Carpal Tunnel Syndrome Questionnaire (CTSQ)Document1 pageCarpal Tunnel Syndrome Questionnaire (CTSQ)Samuel Iñiguez JiménezNo ratings yet
- Jan 2023 Narrative ReportDocument6 pagesJan 2023 Narrative ReportSusan Loida SorianoNo ratings yet
- Chapter - Pain Assessment and ManagementDocument3 pagesChapter - Pain Assessment and ManagementrxNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionRocelyn CristobalNo ratings yet
- Chronic Pelvic PainDocument86 pagesChronic Pelvic PainRiean AuliaNo ratings yet
- Lesson Plan - Pain (Unit 4)Document28 pagesLesson Plan - Pain (Unit 4)Jincy JohnyNo ratings yet
- NCP Draft - Ectopic PregnancyDocument10 pagesNCP Draft - Ectopic PregnancyD CNo ratings yet
- NCP ExampleDocument2 pagesNCP ExampleLeady Joy MorboNo ratings yet
- Quality of Life QuestionnaireDocument4 pagesQuality of Life QuestionnaireJosé NetoNo ratings yet
- Pain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowFrom EverandPain Free 1-2-3: A Proven Program for Eliminating Chronic Pain NowRating: 1 out of 5 stars1/5 (1)
- PNCDocument2 pagesPNClovelove DayoNo ratings yet
- ASSESMENTFINALFINALDocument4 pagesASSESMENTFINALFINALlovelove DayoNo ratings yet
- Review InflamDocument17 pagesReview Inflamlovelove DayoNo ratings yet
- Lourlyn's Angels?Document27 pagesLourlyn's Angels?lovelove DayoNo ratings yet
- The Goal - Aim of-WPS OfficeDocument1 pageThe Goal - Aim of-WPS Officelovelove DayoNo ratings yet
- Significance of The Study and Research DesignDocument1 pageSignificance of The Study and Research Designlovelove DayoNo ratings yet
- Seizure Nursing ManagementDocument1 pageSeizure Nursing Managementlovelove DayoNo ratings yet
- Oral Revalida and Comprehensive ExamDocument13 pagesOral Revalida and Comprehensive Examlovelove DayoNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing Diagnosislovelove DayoNo ratings yet
- MAIN PROBLEM OF-WPS OfficeDocument1 pageMAIN PROBLEM OF-WPS Officelovelove DayoNo ratings yet
- Impact Evaluation IntroDocument12 pagesImpact Evaluation IntroKhuê TrầnNo ratings yet
- Fight, Flight, and FreezeDocument5 pagesFight, Flight, and FreezeLili SingerNo ratings yet
- Reading Practice 01: Just RelaxDocument14 pagesReading Practice 01: Just RelaxNg Thanh ChienNo ratings yet
- Emotional Intelligence Unit I EmotionDocument39 pagesEmotional Intelligence Unit I EmotionHema PriyaNo ratings yet
- Organizing Training of Young Football Players Initial StageDocument3 pagesOrganizing Training of Young Football Players Initial StageAcademic JournalNo ratings yet
- Chapter 3 Levenson. Coping With IllnessDocument40 pagesChapter 3 Levenson. Coping With Illnessjodalo.jdlrNo ratings yet
- MAPEH G-10 1st QuarterDocument11 pagesMAPEH G-10 1st QuarterGian Manzano SelidioNo ratings yet
- 3 Increasing Rejection of IntimaDocument27 pages3 Increasing Rejection of IntimaHan YeNo ratings yet
- Leadership AssessmentDocument9 pagesLeadership Assessmentchanceux 11No ratings yet
- What Is Happening To The Filipino Family?: Ma. Lourdes A. Carandang, PHDDocument24 pagesWhat Is Happening To The Filipino Family?: Ma. Lourdes A. Carandang, PHDAngel CarocheNo ratings yet
- Tweezer Dexterity by Saima KhanDocument6 pagesTweezer Dexterity by Saima KhanHmm OkNo ratings yet
- Long-Term Sickness Absence Due To Mental Disorders Is Associated With Individual Features and Psychosocial Work ConditionsDocument16 pagesLong-Term Sickness Absence Due To Mental Disorders Is Associated With Individual Features and Psychosocial Work ConditionsPollyanna Lavinia Lima RibeiroNo ratings yet
- Bashing Bobo: Introducing Psychological ResearchDocument7 pagesBashing Bobo: Introducing Psychological ResearchAera BangNo ratings yet
- Talk Show ScriptDocument4 pagesTalk Show ScriptJarey SalvalozaNo ratings yet
- The Happy Powder: Neurotransmitter SolutionDocument6 pagesThe Happy Powder: Neurotransmitter SolutionaligaramNo ratings yet
- 2010 ADA Standards For Accessible DesignDocument187 pages2010 ADA Standards For Accessible Designwera-delagarza3536No ratings yet
- Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th Edition Townsend Test BankDocument29 pagesPsychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th Edition Townsend Test BankMichaelJohnsonijybp100% (20)
- Freud, Luria and The Clinical Method: Mark SolmsDocument27 pagesFreud, Luria and The Clinical Method: Mark SolmsVALERIA AGUILAR100% (1)
- Training Your BrainDocument17 pagesTraining Your BrainRajeshNo ratings yet
- Meeting The Ethical Challenges of Leadership - Casting Lightor SHDocument5 pagesMeeting The Ethical Challenges of Leadership - Casting Lightor SHMKNo ratings yet
- CHAPTER 1-3 (1st Set)Document31 pagesCHAPTER 1-3 (1st Set)Jimmy LojaNo ratings yet
- A Systematic Review of The Outcome of Child Abuse in Long-Term CareDocument18 pagesA Systematic Review of The Outcome of Child Abuse in Long-Term CareBea100% (1)
- Intro To Meditation 4 Part Series Handouts Madison 201410Document10 pagesIntro To Meditation 4 Part Series Handouts Madison 201410Mahavidya KarunaNo ratings yet
- Chapter 6: Behavior Intervention Plans (Bip) : Learner OutcomesDocument70 pagesChapter 6: Behavior Intervention Plans (Bip) : Learner OutcomesSabiha BegumNo ratings yet
- Diss Sim 2020 Module 6 PDFDocument27 pagesDiss Sim 2020 Module 6 PDFJuvy MatabalanNo ratings yet
- Family and CommunityDocument46 pagesFamily and CommunityCez0408No ratings yet
- Welfare Checks and Therapeutic Risk Management.8Document5 pagesWelfare Checks and Therapeutic Risk Management.8Marco Dave Gutierrez ParedesNo ratings yet