
ENGLISH CASE G1P0A0L0 34 35 Weeks of Preterm Pregnancy + Severe
ENGLISH CASE G1P0A0L0 34 35 Weeks of Preterm Pregnancy + Severe
You might also like
- Handbook - The Oliver McGowan Mandatory Training On Learning Disability and AutismDocument101 pagesHandbook - The Oliver McGowan Mandatory Training On Learning Disability and AutismMubeenRahmanNo ratings yet
- Ent Exam IsmDocument266 pagesEnt Exam IsmAmit BhadhanaNo ratings yet
- Case Study On LBWDocument43 pagesCase Study On LBWOmotosho Alex50% (2)
- Gestational Trophoblastic DiseaseDocument25 pagesGestational Trophoblastic DiseaseKarelNo ratings yet
- A Case Presentation of An Adult With Gestational Diabetes Mellitus FinalDocument59 pagesA Case Presentation of An Adult With Gestational Diabetes Mellitus FinalJM PunzalanNo ratings yet
- Eglish Case - HbSAg On Pregnancy - MADocument52 pagesEglish Case - HbSAg On Pregnancy - MAfeliaNo ratings yet
- Blighted OvumDocument31 pagesBlighted OvumHeri FarnasNo ratings yet
- Breech Presentation: (English Case)Document56 pagesBreech Presentation: (English Case)Heri FarnasNo ratings yet
- EC - RI - Management Oligohydramnions Due To PPROM Edit-1Document61 pagesEC - RI - Management Oligohydramnions Due To PPROM Edit-1Ridho Berkah PramudithaNo ratings yet
- Cover Lapkas SerangDocument4 pagesCover Lapkas SerangaffanaufalNo ratings yet
- English Case Iufd+covid-19 Fuad SaddamDocument57 pagesEnglish Case Iufd+covid-19 Fuad SaddamanggatrifiandaprimaNo ratings yet
- NCM119ClinicalLab Pediatric Ward Pneumonia Case Study Group 4Document40 pagesNCM119ClinicalLab Pediatric Ward Pneumonia Case Study Group 4Allysa MacalinoNo ratings yet
- Impending EclampsiaDocument48 pagesImpending EclampsiaBrigita De VegaNo ratings yet
- Midwifery Management in Cephalopelvic DisproportionDocument21 pagesMidwifery Management in Cephalopelvic DisproportionBintari Ancinonyx JubatusNo ratings yet
- Kasus KPD Dan BBLRDocument47 pagesKasus KPD Dan BBLRelzaNo ratings yet
- Preeclampsia With Severe Features, Uncontrolled: University of The Cordilleras College of NursingDocument45 pagesPreeclampsia With Severe Features, Uncontrolled: University of The Cordilleras College of NursingAndrei MarcosNo ratings yet
- Hypertension in Pregnancy Cover PageDocument9 pagesHypertension in Pregnancy Cover PageZechariah NicholasNo ratings yet
- Case Study REVISEDDocument88 pagesCase Study REVISEDE.J. PelayoNo ratings yet
- CR MIRA FixDocument42 pagesCR MIRA FixZahranatha Dzaky FadhilaNo ratings yet
- A Case Study On Severe MalariaDocument39 pagesA Case Study On Severe Malariaokelue kingsleyNo ratings yet
- Thesis Attuah Florence sns17Document31 pagesThesis Attuah Florence sns17Tô ThuỷNo ratings yet
- Cover LaporanDocument6 pagesCover LaporanArio SabrangNo ratings yet
- Phase3 Biomed Sciences Manual 2014 FINALDocument238 pagesPhase3 Biomed Sciences Manual 2014 FINALJohnNo ratings yet
- Acute PancreatitisDocument10 pagesAcute PancreatitisCuttie Anne GalangNo ratings yet
- Laporan DH RATU BIONIKA enDocument61 pagesLaporan DH RATU BIONIKA enratuNo ratings yet
- Prognostic Impact of Disease-Related MalnutritionDocument11 pagesPrognostic Impact of Disease-Related MalnutritionYosephine Maria ChristinaNo ratings yet
- UNICEF SD Neonatal Guidelines Report 2018Document195 pagesUNICEF SD Neonatal Guidelines Report 2018أسرار وغرائب owedahNo ratings yet
- Group 3 Hyperemesis Gravidarum FinalDocument75 pagesGroup 3 Hyperemesis Gravidarum FinalJulhanie K. MatalamNo ratings yet
- Kamara - Factors Associated With Neonatal Hyperbilirubinemia in The First 2weeks of Life in OlaDocument56 pagesKamara - Factors Associated With Neonatal Hyperbilirubinemia in The First 2weeks of Life in OlaJulia StantonNo ratings yet
- Case Report Hirschprung DiseaseDocument26 pagesCase Report Hirschprung Diseasemhd risqNo ratings yet
- BSN 4D-2D Ectopic PregnancyDocument50 pagesBSN 4D-2D Ectopic PregnancyMac Cristian A. CaraganNo ratings yet
- National Clinical Guideline For Intrapartum Fetal Monitoring GuidelineDocument53 pagesNational Clinical Guideline For Intrapartum Fetal Monitoring GuidelineShiv PandeyNo ratings yet
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Prot Sap 000Document24 pagesProt Sap 000Abdiladif MahamudNo ratings yet
- Ddu GMN - Docx FDocument48 pagesDdu GMN - Docx Falexdereje745No ratings yet
- Mukade Elizabeth Alemun Research Proposal For Faculty DefenseDocument51 pagesMukade Elizabeth Alemun Research Proposal For Faculty DefensemwngjrmNo ratings yet
- CS HGDocument74 pagesCS HGTricia Denise EstabilloNo ratings yet
- English in Nursing Ii Nursing Care Plan of Endocrine System (Diabetes Mellitus)Document33 pagesEnglish in Nursing Ii Nursing Care Plan of Endocrine System (Diabetes Mellitus)Najla KhairunnisaNo ratings yet
- REFERAT II - 3rdDocument41 pagesREFERAT II - 3rdagung anugrahNo ratings yet
- G 5 FinalDocument35 pagesG 5 FinalKirubel KassahunNo ratings yet
- Genetics in Diabetes - SGD B10Document18 pagesGenetics in Diabetes - SGD B10Giovanca Verentzia Purnama 1902511148No ratings yet
- English Case - VBACDocument41 pagesEnglish Case - VBACJuan Habli SoufalNo ratings yet
- Case Study Not FinalDocument45 pagesCase Study Not FinalMarshin Thea CelociaNo ratings yet
- Anemia AplastikDocument33 pagesAnemia AplastikEvelin SimarmataNo ratings yet
- Covid-19 Ris UpDocument21 pagesCovid-19 Ris UpGift MesaNo ratings yet
- Buku Parasit MalariaDocument82 pagesBuku Parasit MalariaAnnisa Afdathul RizqaNo ratings yet
- Efficacy and Safety of Pharmacological Treatments of Chagas DiseaseDocument96 pagesEfficacy and Safety of Pharmacological Treatments of Chagas Diseaseyerli bahosNo ratings yet
- Kelvin FinalDocument33 pagesKelvin FinalBenard apiriNo ratings yet
- Role of Modified Biophysical Profile in Predicting Perinatal Outcome in High Risk PregnancyDocument5 pagesRole of Modified Biophysical Profile in Predicting Perinatal Outcome in High Risk PregnancyIJAR JOURNALNo ratings yet
- Caesarean Delivery During Second Stage of Labor - A Study of Fetomaternal Outcome in A Tertiary Care HospitalDocument4 pagesCaesarean Delivery During Second Stage of Labor - A Study of Fetomaternal Outcome in A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- 2020 3F 2b Case Pres AutosavedDocument41 pages2020 3F 2b Case Pres AutosavedMikko McDonie VeloriaNo ratings yet
- LP Artha Gadar Dalam FixDocument33 pagesLP Artha Gadar Dalam FixAnis MutiaraNo ratings yet
- Agus Karlis 2Document83 pagesAgus Karlis 2ayu auraliaNo ratings yet
- A Retrospective Study in A Women With Recuurent Pregnancy Loss in A Tertiary Care CentreDocument2 pagesA Retrospective Study in A Women With Recuurent Pregnancy Loss in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- DENTEP Desertation FINALDocument83 pagesDENTEP Desertation FINALCESAR NDJOKONo ratings yet
- DTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossDocument30 pagesDTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossChe LaiNo ratings yet
- BST Obstetrics Gynaecology Curriculum 2018 19 Years 23 Printable Version PDFDocument78 pagesBST Obstetrics Gynaecology Curriculum 2018 19 Years 23 Printable Version PDFshruthi mzmcNo ratings yet
- Oral Pathology in The Pediatric Patient A Clinical Guide To The Diagnosis and Treatment of Mucosal Lesions 1st Edition Elizabeth PhiliponeDocument45 pagesOral Pathology in The Pediatric Patient A Clinical Guide To The Diagnosis and Treatment of Mucosal Lesions 1st Edition Elizabeth Philiponesherri.gandhi786100% (4)
- Incomplete Abortion: A Mini Case Study OnDocument22 pagesIncomplete Abortion: A Mini Case Study OnSunny MujmuleNo ratings yet
- Inborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsFrom EverandInborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsNo ratings yet
- Gambar To TeksDocument2 pagesGambar To TeksfeliaNo ratings yet
- Teks Cerita SejarahDocument5 pagesTeks Cerita SejarahfeliaNo ratings yet
- Soal Regarding Menoupause ConditionDocument6 pagesSoal Regarding Menoupause ConditionfeliaNo ratings yet
- Daftar Pustaka JurnalDocument3 pagesDaftar Pustaka JurnalfeliaNo ratings yet
- Eglish Case - HbSAg On Pregnancy - MADocument52 pagesEglish Case - HbSAg On Pregnancy - MAfeliaNo ratings yet
- Zuqiaoyin Gb-44: Yin Portals of The FootDocument2 pagesZuqiaoyin Gb-44: Yin Portals of The Footray72roNo ratings yet
- SH Ankh Push PiDocument10 pagesSH Ankh Push PiRavindra ChobariNo ratings yet
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- Presentation1 Ankush (Autosaved)Document17 pagesPresentation1 Ankush (Autosaved)AnshulNo ratings yet
- Stop The Bleed Booklet FinalDocument16 pagesStop The Bleed Booklet FinalUrsula MalauNo ratings yet
- Introduction To AnesthesiologyDocument68 pagesIntroduction To AnesthesiologyOzza AlhudaNo ratings yet
- Test Name Units Value Technology Fasting Blood Sugar Photometry MG/DL 176.9 Reference RangeDocument15 pagesTest Name Units Value Technology Fasting Blood Sugar Photometry MG/DL 176.9 Reference RangeRamesh DeshpandeNo ratings yet
- Selling Sickness, Ray Moynihan and Alan CasselsDocument18 pagesSelling Sickness, Ray Moynihan and Alan Casselsanaluzinha50% (2)
- Herpes ZosterDocument5 pagesHerpes ZosterTeodora PatrauceanNo ratings yet
- PICO & Search Strategy Worksheet: Name: Macayla GreinerDocument6 pagesPICO & Search Strategy Worksheet: Name: Macayla Greinerapi-407402630No ratings yet
- Dr. Ronald Frans, SP - THT-KL, MKes.Document12 pagesDr. Ronald Frans, SP - THT-KL, MKes.alpriani patrasNo ratings yet
- CantharisDocument4 pagesCantharisShubhanshi Bhasin100% (1)
- NCPDocument3 pagesNCPJyn Jyn0% (1)
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryJohn Alex SelorioNo ratings yet
- Humulin R, Novolin RDocument2 pagesHumulin R, Novolin RSheri490100% (2)
- DR Final 2016Document21 pagesDR Final 2016cristianbanNo ratings yet
- Bakteri PeriodontalDocument31 pagesBakteri PeriodontalShahnaz DwiNo ratings yet
- MudrasDocument3 pagesMudrascristianpopoviciNo ratings yet
- AssessmentDocument7 pagesAssessmentSheryhan Tahir BayleNo ratings yet
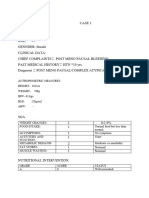
- Case 1Document7 pagesCase 1bsc.clinicalnutrition2018No ratings yet
- Aravind Case StudyDocument14 pagesAravind Case StudyOmkar PranavNo ratings yet
- The History of Leprosy in CambodiaDocument64 pagesThe History of Leprosy in CambodiaNeakreach PichNo ratings yet
- Esophageal Carcinoma in Mogadishu, Somalia: A Four Year Retrospective StudyDocument2 pagesEsophageal Carcinoma in Mogadishu, Somalia: A Four Year Retrospective StudyDr Mohamed KadleNo ratings yet
- Breast CancerDocument68 pagesBreast Cancerapi-3748365100% (4)
- Bio-Psycho-Social Aspect of Pain: Madonna Damayanthie DatuDocument64 pagesBio-Psycho-Social Aspect of Pain: Madonna Damayanthie DatuRey AlwiwikhNo ratings yet
- Sengupta Et Al., 2022 - COVID-19 & Vitamin CDocument8 pagesSengupta Et Al., 2022 - COVID-19 & Vitamin CDr.Pallav SenguptaNo ratings yet
- Urine Analysis.Document2 pagesUrine Analysis.aryasingh14022006No ratings yet
- CBCT 170421190936Document94 pagesCBCT 170421190936hazeemmegahed100% (1)




























































































Download as docx, pdf, or txt
You might also like
- Handbook - The Oliver McGowan Mandatory Training On Learning Disability and AutismDocument101 pagesHandbook - The Oliver McGowan Mandatory Training On Learning Disability and AutismMubeenRahmanNo ratings yet
- Ent Exam IsmDocument266 pagesEnt Exam IsmAmit BhadhanaNo ratings yet
- Case Study On LBWDocument43 pagesCase Study On LBWOmotosho Alex50% (2)
- Gestational Trophoblastic DiseaseDocument25 pagesGestational Trophoblastic DiseaseKarelNo ratings yet
- A Case Presentation of An Adult With Gestational Diabetes Mellitus FinalDocument59 pagesA Case Presentation of An Adult With Gestational Diabetes Mellitus FinalJM PunzalanNo ratings yet
- Eglish Case - HbSAg On Pregnancy - MADocument52 pagesEglish Case - HbSAg On Pregnancy - MAfeliaNo ratings yet
- Blighted OvumDocument31 pagesBlighted OvumHeri FarnasNo ratings yet
- Breech Presentation: (English Case)Document56 pagesBreech Presentation: (English Case)Heri FarnasNo ratings yet
- EC - RI - Management Oligohydramnions Due To PPROM Edit-1Document61 pagesEC - RI - Management Oligohydramnions Due To PPROM Edit-1Ridho Berkah PramudithaNo ratings yet
- Cover Lapkas SerangDocument4 pagesCover Lapkas SerangaffanaufalNo ratings yet
- English Case Iufd+covid-19 Fuad SaddamDocument57 pagesEnglish Case Iufd+covid-19 Fuad SaddamanggatrifiandaprimaNo ratings yet
- NCM119ClinicalLab Pediatric Ward Pneumonia Case Study Group 4Document40 pagesNCM119ClinicalLab Pediatric Ward Pneumonia Case Study Group 4Allysa MacalinoNo ratings yet
- Impending EclampsiaDocument48 pagesImpending EclampsiaBrigita De VegaNo ratings yet
- Midwifery Management in Cephalopelvic DisproportionDocument21 pagesMidwifery Management in Cephalopelvic DisproportionBintari Ancinonyx JubatusNo ratings yet
- Kasus KPD Dan BBLRDocument47 pagesKasus KPD Dan BBLRelzaNo ratings yet
- Preeclampsia With Severe Features, Uncontrolled: University of The Cordilleras College of NursingDocument45 pagesPreeclampsia With Severe Features, Uncontrolled: University of The Cordilleras College of NursingAndrei MarcosNo ratings yet
- Hypertension in Pregnancy Cover PageDocument9 pagesHypertension in Pregnancy Cover PageZechariah NicholasNo ratings yet
- Case Study REVISEDDocument88 pagesCase Study REVISEDE.J. PelayoNo ratings yet
- CR MIRA FixDocument42 pagesCR MIRA FixZahranatha Dzaky FadhilaNo ratings yet
- A Case Study On Severe MalariaDocument39 pagesA Case Study On Severe Malariaokelue kingsleyNo ratings yet
- Thesis Attuah Florence sns17Document31 pagesThesis Attuah Florence sns17Tô ThuỷNo ratings yet
- Cover LaporanDocument6 pagesCover LaporanArio SabrangNo ratings yet
- Phase3 Biomed Sciences Manual 2014 FINALDocument238 pagesPhase3 Biomed Sciences Manual 2014 FINALJohnNo ratings yet
- Acute PancreatitisDocument10 pagesAcute PancreatitisCuttie Anne GalangNo ratings yet
- Laporan DH RATU BIONIKA enDocument61 pagesLaporan DH RATU BIONIKA enratuNo ratings yet
- Prognostic Impact of Disease-Related MalnutritionDocument11 pagesPrognostic Impact of Disease-Related MalnutritionYosephine Maria ChristinaNo ratings yet
- UNICEF SD Neonatal Guidelines Report 2018Document195 pagesUNICEF SD Neonatal Guidelines Report 2018أسرار وغرائب owedahNo ratings yet
- Group 3 Hyperemesis Gravidarum FinalDocument75 pagesGroup 3 Hyperemesis Gravidarum FinalJulhanie K. MatalamNo ratings yet
- Kamara - Factors Associated With Neonatal Hyperbilirubinemia in The First 2weeks of Life in OlaDocument56 pagesKamara - Factors Associated With Neonatal Hyperbilirubinemia in The First 2weeks of Life in OlaJulia StantonNo ratings yet
- Case Report Hirschprung DiseaseDocument26 pagesCase Report Hirschprung Diseasemhd risqNo ratings yet
- BSN 4D-2D Ectopic PregnancyDocument50 pagesBSN 4D-2D Ectopic PregnancyMac Cristian A. CaraganNo ratings yet
- National Clinical Guideline For Intrapartum Fetal Monitoring GuidelineDocument53 pagesNational Clinical Guideline For Intrapartum Fetal Monitoring GuidelineShiv PandeyNo ratings yet
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Prot Sap 000Document24 pagesProt Sap 000Abdiladif MahamudNo ratings yet
- Ddu GMN - Docx FDocument48 pagesDdu GMN - Docx Falexdereje745No ratings yet
- Mukade Elizabeth Alemun Research Proposal For Faculty DefenseDocument51 pagesMukade Elizabeth Alemun Research Proposal For Faculty DefensemwngjrmNo ratings yet
- CS HGDocument74 pagesCS HGTricia Denise EstabilloNo ratings yet
- English in Nursing Ii Nursing Care Plan of Endocrine System (Diabetes Mellitus)Document33 pagesEnglish in Nursing Ii Nursing Care Plan of Endocrine System (Diabetes Mellitus)Najla KhairunnisaNo ratings yet
- REFERAT II - 3rdDocument41 pagesREFERAT II - 3rdagung anugrahNo ratings yet
- G 5 FinalDocument35 pagesG 5 FinalKirubel KassahunNo ratings yet
- Genetics in Diabetes - SGD B10Document18 pagesGenetics in Diabetes - SGD B10Giovanca Verentzia Purnama 1902511148No ratings yet
- English Case - VBACDocument41 pagesEnglish Case - VBACJuan Habli SoufalNo ratings yet
- Case Study Not FinalDocument45 pagesCase Study Not FinalMarshin Thea CelociaNo ratings yet
- Anemia AplastikDocument33 pagesAnemia AplastikEvelin SimarmataNo ratings yet
- Covid-19 Ris UpDocument21 pagesCovid-19 Ris UpGift MesaNo ratings yet
- Buku Parasit MalariaDocument82 pagesBuku Parasit MalariaAnnisa Afdathul RizqaNo ratings yet
- Efficacy and Safety of Pharmacological Treatments of Chagas DiseaseDocument96 pagesEfficacy and Safety of Pharmacological Treatments of Chagas Diseaseyerli bahosNo ratings yet
- Kelvin FinalDocument33 pagesKelvin FinalBenard apiriNo ratings yet
- Role of Modified Biophysical Profile in Predicting Perinatal Outcome in High Risk PregnancyDocument5 pagesRole of Modified Biophysical Profile in Predicting Perinatal Outcome in High Risk PregnancyIJAR JOURNALNo ratings yet
- Caesarean Delivery During Second Stage of Labor - A Study of Fetomaternal Outcome in A Tertiary Care HospitalDocument4 pagesCaesarean Delivery During Second Stage of Labor - A Study of Fetomaternal Outcome in A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- 2020 3F 2b Case Pres AutosavedDocument41 pages2020 3F 2b Case Pres AutosavedMikko McDonie VeloriaNo ratings yet
- LP Artha Gadar Dalam FixDocument33 pagesLP Artha Gadar Dalam FixAnis MutiaraNo ratings yet
- Agus Karlis 2Document83 pagesAgus Karlis 2ayu auraliaNo ratings yet
- A Retrospective Study in A Women With Recuurent Pregnancy Loss in A Tertiary Care CentreDocument2 pagesA Retrospective Study in A Women With Recuurent Pregnancy Loss in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- DENTEP Desertation FINALDocument83 pagesDENTEP Desertation FINALCESAR NDJOKONo ratings yet
- DTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossDocument30 pagesDTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossChe LaiNo ratings yet
- BST Obstetrics Gynaecology Curriculum 2018 19 Years 23 Printable Version PDFDocument78 pagesBST Obstetrics Gynaecology Curriculum 2018 19 Years 23 Printable Version PDFshruthi mzmcNo ratings yet
- Oral Pathology in The Pediatric Patient A Clinical Guide To The Diagnosis and Treatment of Mucosal Lesions 1st Edition Elizabeth PhiliponeDocument45 pagesOral Pathology in The Pediatric Patient A Clinical Guide To The Diagnosis and Treatment of Mucosal Lesions 1st Edition Elizabeth Philiponesherri.gandhi786100% (4)
- Incomplete Abortion: A Mini Case Study OnDocument22 pagesIncomplete Abortion: A Mini Case Study OnSunny MujmuleNo ratings yet
- Inborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsFrom EverandInborn Errors of Metabolism - Early Detection, Key Symptoms and Therapeutic OptionsNo ratings yet
- Gambar To TeksDocument2 pagesGambar To TeksfeliaNo ratings yet
- Teks Cerita SejarahDocument5 pagesTeks Cerita SejarahfeliaNo ratings yet
- Soal Regarding Menoupause ConditionDocument6 pagesSoal Regarding Menoupause ConditionfeliaNo ratings yet
- Daftar Pustaka JurnalDocument3 pagesDaftar Pustaka JurnalfeliaNo ratings yet
- Eglish Case - HbSAg On Pregnancy - MADocument52 pagesEglish Case - HbSAg On Pregnancy - MAfeliaNo ratings yet
- Zuqiaoyin Gb-44: Yin Portals of The FootDocument2 pagesZuqiaoyin Gb-44: Yin Portals of The Footray72roNo ratings yet
- SH Ankh Push PiDocument10 pagesSH Ankh Push PiRavindra ChobariNo ratings yet
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- Presentation1 Ankush (Autosaved)Document17 pagesPresentation1 Ankush (Autosaved)AnshulNo ratings yet
- Stop The Bleed Booklet FinalDocument16 pagesStop The Bleed Booklet FinalUrsula MalauNo ratings yet
- Introduction To AnesthesiologyDocument68 pagesIntroduction To AnesthesiologyOzza AlhudaNo ratings yet
- Test Name Units Value Technology Fasting Blood Sugar Photometry MG/DL 176.9 Reference RangeDocument15 pagesTest Name Units Value Technology Fasting Blood Sugar Photometry MG/DL 176.9 Reference RangeRamesh DeshpandeNo ratings yet
- Selling Sickness, Ray Moynihan and Alan CasselsDocument18 pagesSelling Sickness, Ray Moynihan and Alan Casselsanaluzinha50% (2)
- Herpes ZosterDocument5 pagesHerpes ZosterTeodora PatrauceanNo ratings yet
- PICO & Search Strategy Worksheet: Name: Macayla GreinerDocument6 pagesPICO & Search Strategy Worksheet: Name: Macayla Greinerapi-407402630No ratings yet
- Dr. Ronald Frans, SP - THT-KL, MKes.Document12 pagesDr. Ronald Frans, SP - THT-KL, MKes.alpriani patrasNo ratings yet
- CantharisDocument4 pagesCantharisShubhanshi Bhasin100% (1)
- NCPDocument3 pagesNCPJyn Jyn0% (1)
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryJohn Alex SelorioNo ratings yet
- Humulin R, Novolin RDocument2 pagesHumulin R, Novolin RSheri490100% (2)
- DR Final 2016Document21 pagesDR Final 2016cristianbanNo ratings yet
- Bakteri PeriodontalDocument31 pagesBakteri PeriodontalShahnaz DwiNo ratings yet
- MudrasDocument3 pagesMudrascristianpopoviciNo ratings yet
- AssessmentDocument7 pagesAssessmentSheryhan Tahir BayleNo ratings yet
- Case 1Document7 pagesCase 1bsc.clinicalnutrition2018No ratings yet
- Aravind Case StudyDocument14 pagesAravind Case StudyOmkar PranavNo ratings yet
- The History of Leprosy in CambodiaDocument64 pagesThe History of Leprosy in CambodiaNeakreach PichNo ratings yet
- Esophageal Carcinoma in Mogadishu, Somalia: A Four Year Retrospective StudyDocument2 pagesEsophageal Carcinoma in Mogadishu, Somalia: A Four Year Retrospective StudyDr Mohamed KadleNo ratings yet
- Breast CancerDocument68 pagesBreast Cancerapi-3748365100% (4)
- Bio-Psycho-Social Aspect of Pain: Madonna Damayanthie DatuDocument64 pagesBio-Psycho-Social Aspect of Pain: Madonna Damayanthie DatuRey AlwiwikhNo ratings yet
- Sengupta Et Al., 2022 - COVID-19 & Vitamin CDocument8 pagesSengupta Et Al., 2022 - COVID-19 & Vitamin CDr.Pallav SenguptaNo ratings yet
- Urine Analysis.Document2 pagesUrine Analysis.aryasingh14022006No ratings yet
- CBCT 170421190936Document94 pagesCBCT 170421190936hazeemmegahed100% (1)