Download as docx, pdf, or txt
You might also like
- Chlorine Disinfection AssignmentDocument80 pagesChlorine Disinfection AssignmentGkou Dojku0% (1)
- Water Contamination and Its Related DiseasesDocument3 pagesWater Contamination and Its Related DiseasesrahmanNo ratings yet
- Hazards in Drinking-Water Supply and Waste Management: 3.1 Microbial Risks: Waterborne Infectious DiseaseDocument8 pagesHazards in Drinking-Water Supply and Waste Management: 3.1 Microbial Risks: Waterborne Infectious Diseasekasandra01No ratings yet
- Water Related Diseases and Water ContaminantsDocument8 pagesWater Related Diseases and Water ContaminantsBuenavista, John Edrin D.No ratings yet
- Water and Food BacteriologyDocument95 pagesWater and Food BacteriologydavidmanyielmalualNo ratings yet
- Environment: Highlight of National Trends) : Waterway Filled With "Sludge."Document2 pagesEnvironment: Highlight of National Trends) : Waterway Filled With "Sludge."Jethro Alacon100% (1)
- Health Risk Assessment of Cyanobacterial (Blue-Green Algal) Toxins in Drinking WaterDocument8 pagesHealth Risk Assessment of Cyanobacterial (Blue-Green Algal) Toxins in Drinking WaterTiago MattosNo ratings yet
- Waterborne DiseasesDocument4 pagesWaterborne DiseasesAsifa HussainNo ratings yet
- FINALDocument7 pagesFINALDerrickNo ratings yet
- What Diseases Are Commonly Caused by Wastewater?Document7 pagesWhat Diseases Are Commonly Caused by Wastewater?RimaQuitainNo ratings yet
- Waterborne Diseases 2Document34 pagesWaterborne Diseases 2YOSEF DERDESAWENo ratings yet
- Httpsciteseerx Ist Psu Edudocumentrepid Rep1&Type PDF&Doi Dac388faDocument39 pagesHttpsciteseerx Ist Psu Edudocumentrepid Rep1&Type PDF&Doi Dac388fa98zjwkvysjNo ratings yet
- WHO Guidelines For Drinking Water QualityDocument28 pagesWHO Guidelines For Drinking Water QualityClaire Go-MaNo ratings yet
- GY339 Environmental Classification of Excreta Related Disease 2017Document58 pagesGY339 Environmental Classification of Excreta Related Disease 2017Lorraine100% (1)
- PGH 108 07 334Document5 pagesPGH 108 07 334Insyirah DaudNo ratings yet
- The Illnesses Caused by Our Poor Environmental SanitationDocument11 pagesThe Illnesses Caused by Our Poor Environmental SanitationfordmayNo ratings yet
- Waterborne Diseases 1Document26 pagesWaterborne Diseases 1Dalia Talaat WehediNo ratings yet
- EEN3700 - Learning Unit 1A - 2020Document46 pagesEEN3700 - Learning Unit 1A - 2020JAMES SITHOLENo ratings yet
- Water Borne DiseaseDocument25 pagesWater Borne DiseaseAdefila Sunday DadaNo ratings yet
- Public Health Implications of Indiscriminate Urination and DefeacationDocument6 pagesPublic Health Implications of Indiscriminate Urination and Defeacationoludoyinmola5ojifinnNo ratings yet
- Article 1437044519Document14 pagesArticle 1437044519mohdanasullahNo ratings yet
- Water Borne DiseasesDocument4 pagesWater Borne DiseasesGaurav YadavNo ratings yet
- Water Borne Outbreaks: Sri Sariga - 130Document25 pagesWater Borne Outbreaks: Sri Sariga - 130AvigailNo ratings yet
- Siwila 2020Document14 pagesSiwila 2020GTA5ON360No ratings yet
- Water Borne Diseases in MalaysiaDocument29 pagesWater Borne Diseases in MalaysiaMohd Nazrul Izat0% (1)
- Wastewater Treatment Part 2Document7 pagesWastewater Treatment Part 2Khaled M FawzyNo ratings yet
- What Are Water-Borne Diseases?: Hepatitis A CholeraDocument1 pageWhat Are Water-Borne Diseases?: Hepatitis A Choleraabbey0810No ratings yet
- Chapter 1 CapstoneDocument16 pagesChapter 1 CapstoneJade MarapocNo ratings yet
- Chapter 7 Health Issues Related To Drainage ManagementDocument16 pagesChapter 7 Health Issues Related To Drainage ManagementMichael VillavertNo ratings yet
- A Seminar On Microgansims of Public Health Importance in WaterDocument40 pagesA Seminar On Microgansims of Public Health Importance in Waterjoe topeNo ratings yet
- Food Microbiology: 6.12 The Richmond Report On The Microbiological Safety of FoodDocument8 pagesFood Microbiology: 6.12 The Richmond Report On The Microbiological Safety of FoodElviana YaputraNo ratings yet
- S3 HSRDocument6 pagesS3 HSRPraful KakdeNo ratings yet
- ESST3103 Assignment 1Document9 pagesESST3103 Assignment 1Manda BaboolalNo ratings yet
- Dangerous WatersDocument2 pagesDangerous WatersMichaelChenNo ratings yet
- Water, Sanitation, and Hygiene: Some Facts and FiguresDocument2 pagesWater, Sanitation, and Hygiene: Some Facts and FiguresRanjeet AstroNo ratings yet
- Diarrhea Safe Water Treatment and Storage in The Home: A Practical New Strategy To Prevent Waterborne Disease Mintz E, Reiff F, Tauxe RDocument7 pagesDiarrhea Safe Water Treatment and Storage in The Home: A Practical New Strategy To Prevent Waterborne Disease Mintz E, Reiff F, Tauxe RAmir RuddinNo ratings yet
- Anaam Jawad Alabbasy, Et AlDocument11 pagesAnaam Jawad Alabbasy, Et Alhaidarullah0060116No ratings yet
- Cryptosporidios IS: Bloomfield College Department of Sciences MicrobiologyDocument17 pagesCryptosporidios IS: Bloomfield College Department of Sciences MicrobiologyurdanetacalNo ratings yet
- Doh 07Document37 pagesDoh 07Malack ChagwaNo ratings yet
- Ater and Health Two Precious Resources Linked To One AnotherDocument6 pagesAter and Health Two Precious Resources Linked To One AnotherSomaSorrowNo ratings yet
- Water Borne DiseasesDocument73 pagesWater Borne DiseasesccluruNo ratings yet
- SP1 Water As Disease Transmition (Bryan - 049)Document10 pagesSP1 Water As Disease Transmition (Bryan - 049)Bryan NandaNo ratings yet
- 9711 Pathogenic ProtozoaDocument17 pages9711 Pathogenic Protozoaandria.aquinoNo ratings yet
- Infectious Diarrheal Disease and DehydrationDocument12 pagesInfectious Diarrheal Disease and DehydrationSNo ratings yet
- Emergent Treatment of GastroenteritisDocument28 pagesEmergent Treatment of GastroenteritisLaura Anghel-MocanuNo ratings yet
- Group 8 Power PointDocument10 pagesGroup 8 Power Pointejohn8340No ratings yet
- The Treatment of Rainwater For Potable Use: General Manager, Sales & Marketing, Davey Water ProductsDocument7 pagesThe Treatment of Rainwater For Potable Use: General Manager, Sales & Marketing, Davey Water Productsmohammad yaseenNo ratings yet
- Water SolutionDocument4 pagesWater Solutionagustiani ari wahyu utamiNo ratings yet
- Microbiological Water PollutionDocument2 pagesMicrobiological Water PollutionTamara AprilliaNo ratings yet
- Hygiene Promotion: Toilets and Other HardwareDocument6 pagesHygiene Promotion: Toilets and Other HardwareGerez999No ratings yet
- 78792357article 82887 Libre - pdf1642246297 &response ConDocument7 pages78792357article 82887 Libre - pdf1642246297 &response Con98zjwkvysjNo ratings yet
- Water For The World: Methods of Controlling SchistosomiasisDocument6 pagesWater For The World: Methods of Controlling SchistosomiasisCasimiro ValdambraNo ratings yet
- Untitled PresentationDocument23 pagesUntitled Presentationuq556127No ratings yet
- Research Paper Water Borne DiseasesDocument4 pagesResearch Paper Water Borne Diseasesegtwfsaf100% (1)
- Ahmed Project YSU (1) FINAL EDITION 2016 2017-1Document28 pagesAhmed Project YSU (1) FINAL EDITION 2016 2017-1Yakubu Adamu JajereNo ratings yet
- SchistosomiasisDocument6 pagesSchistosomiasisLyra LorcaNo ratings yet
- Water Hygiene and Sanitation1 2Document62 pagesWater Hygiene and Sanitation1 2mrdaauud09No ratings yet
- Food (Seafood) Borne Outbreaks: R.Varidianto Yudo T., dr.,M.KesDocument21 pagesFood (Seafood) Borne Outbreaks: R.Varidianto Yudo T., dr.,M.KesAkasorachiNo ratings yet
- 1 PBDocument9 pages1 PBSemAyat GoremsNo ratings yet
- Chlorine in Water Disinfection: Hend Galal-GorchevDocument5 pagesChlorine in Water Disinfection: Hend Galal-GorchevMarcela TapiasNo ratings yet
- Rice PaperDocument11 pagesRice PaperEshona ChakrabortyNo ratings yet
- Koushali Singha Roy Review On Marine Fungi PDFDocument15 pagesKoushali Singha Roy Review On Marine Fungi PDFEshona ChakrabortyNo ratings yet
- Review Paper On THERMOPHILIC BACTERIA AND THEIR APPLICATION NEWDocument14 pagesReview Paper On THERMOPHILIC BACTERIA AND THEIR APPLICATION NEWEshona ChakrabortyNo ratings yet
- Jayabrata Mukherjee Review Paper PDFDocument10 pagesJayabrata Mukherjee Review Paper PDFEshona ChakrabortyNo ratings yet
- Fecal Incident Response GuidelinesDocument4 pagesFecal Incident Response Guidelinesm67pvmqymmNo ratings yet
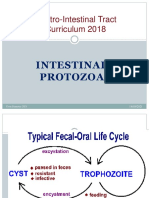
- Intestinal Protozoa 2021Document50 pagesIntestinal Protozoa 2021DragnosNo ratings yet
- WST 083010001Document25 pagesWST 083010001AMANDA PUTRINo ratings yet
- Molecular Characterization of Cryptosporidium - 2019 - Veterinary ParasitologyDocument8 pagesMolecular Characterization of Cryptosporidium - 2019 - Veterinary ParasitologyDewa Aix61No ratings yet
- Hurdey Risk ManagementDocument10 pagesHurdey Risk Managementmichael17ph2003No ratings yet
- Health and Safety in Emergency ResponseDocument11 pagesHealth and Safety in Emergency ResponsePaul Dan OctavianNo ratings yet
- Epidemiology of Cryptosporidium Infection in Different Hosts in Nigeria A Meta-AnalysisDocument13 pagesEpidemiology of Cryptosporidium Infection in Different Hosts in Nigeria A Meta-AnalysiswiwienNo ratings yet
- Topic 3 - Microbial DIsease of Digestive SystemDocument106 pagesTopic 3 - Microbial DIsease of Digestive SystemJewel YvonneNo ratings yet
- Ce 5230 Water Treatment Plant DesignDocument25 pagesCe 5230 Water Treatment Plant Designapi-297914209No ratings yet
- ALVAREZ2002 MolnariDocument15 pagesALVAREZ2002 MolnariBrayan KuraharaNo ratings yet
- Code of Practice PWTAG 2016 PDFDocument40 pagesCode of Practice PWTAG 2016 PDFjpineda_685526No ratings yet
- 2009-Comparative Sensitivity of PCR Primer Sets For Detection of Cryptosporidium ParvumDocument6 pages2009-Comparative Sensitivity of PCR Primer Sets For Detection of Cryptosporidium ParvumWiwien HendrawanNo ratings yet
- About My Family EssayDocument7 pagesAbout My Family Essayniwujuj0juw2100% (2)
- 5 - Masters, Gilbert M. (Water Pollution)Document104 pages5 - Masters, Gilbert M. (Water Pollution)shibu c komathNo ratings yet
- The Disinfection Methods Used For Cryptosporidium Parvum: By: Pinar EryuvaDocument15 pagesThe Disinfection Methods Used For Cryptosporidium Parvum: By: Pinar EryuvaSabina BojadžićNo ratings yet
- Pathogens in The Environment: - Viruses and Prions - Bacteria and Rickettsiae - Fungi and Algae - Protozoans - HelminthsDocument34 pagesPathogens in The Environment: - Viruses and Prions - Bacteria and Rickettsiae - Fungi and Algae - Protozoans - HelminthsEnaANo ratings yet
- Share 'Module - Safety and Sanitation 4-5.docx'Document24 pagesShare 'Module - Safety and Sanitation 4-5.docx'ana mejicoNo ratings yet
- Abb - Industria Del Agua: Agua Potable Y EfluentesDocument154 pagesAbb - Industria Del Agua: Agua Potable Y EfluentesJuan PercNo ratings yet
- Case Study HIV With DiarrheaDocument29 pagesCase Study HIV With DiarrheaMatin Ahmad Khan100% (1)
- Coccidian ParasitesDocument9 pagesCoccidian ParasitessaketNo ratings yet
- Drinking Water and SanitationDocument11 pagesDrinking Water and Sanitationmanusia biasaNo ratings yet
- Parasitology Preservation MethodsDocument5 pagesParasitology Preservation MethodsAinah Charina TapicNo ratings yet
- Literature Review of GiardiasisDocument4 pagesLiterature Review of Giardiasisc5ryek5a100% (1)
- Coccidia: - Characterized by Thick-Walled OocystsDocument26 pagesCoccidia: - Characterized by Thick-Walled Oocyststaty jatyNo ratings yet
- Diagnosis, Parasitose em AvesDocument10 pagesDiagnosis, Parasitose em AvesRoberio OlindaNo ratings yet
- 2021 Parasitology Lab CoccidiansDocument55 pages2021 Parasitology Lab CoccidiansPhilip Patrick LeeNo ratings yet
- Microbiological Water PollutionDocument2 pagesMicrobiological Water PollutionTamara AprilliaNo ratings yet
- 3M Water Filtration Products - High Flow Series - HF40 and HF40 - S Performance Data SheetDocument2 pages3M Water Filtration Products - High Flow Series - HF40 and HF40 - S Performance Data SheetSergioNo ratings yet
- Myhaccp Study: Honey & Lemon Yogurt: Business NameDocument42 pagesMyhaccp Study: Honey & Lemon Yogurt: Business NameDiana Sofia Caldera GaleanoNo ratings yet



























































![Sewage and sewerage of farm homes [1928]](https://imgv2-1-f.scribdassets.com/img/word_document/544942443/149x198/ae3275e6b6/1676295883?v=1)