Download as docx, pdf, or txt
You might also like
- G-0546 Outpatient Nutrition Assessment FormDocument3 pagesG-0546 Outpatient Nutrition Assessment FormGiovanna Rosario Arroyo100% (2)
- Essential Nursing Content VideoDocument11 pagesEssential Nursing Content VideoNikki SanchezNo ratings yet
- Just One More Question: Stories From A Life in Neurology - Niall TubridyDocument6 pagesJust One More Question: Stories From A Life in Neurology - Niall TubridyracymotaNo ratings yet
- Drug of Abuse (Table) PDFDocument2 pagesDrug of Abuse (Table) PDFtchanochNo ratings yet
- Pharmacology Important Things To RememberDocument5 pagesPharmacology Important Things To RememberHydie100% (1)
- VN8 Term 2 Calendar Updated June 2, 2021Document7 pagesVN8 Term 2 Calendar Updated June 2, 2021Janmarie BongcaronNo ratings yet
- GastrointestinalDocument23 pagesGastrointestinalArvee Caezar F. VizcarraNo ratings yet
- NCLEX Mark K NotesDocument131 pagesNCLEX Mark K NotesRhika Mae ObraNo ratings yet
- Chronic Renal FailureDocument7 pagesChronic Renal Failuretantalizin marieNo ratings yet
- PHARMACOLOGY CompilesDocument83 pagesPHARMACOLOGY Compilesjj alotintoNo ratings yet
- Nurseslabs Lab Values PDFDocument2 pagesNurseslabs Lab Values PDFJan BularioNo ratings yet
- NCLEX Review GuideDocument3 pagesNCLEX Review GuidefallenangelleNo ratings yet
- Integumentry PDFDocument17 pagesIntegumentry PDFMehul RathoreNo ratings yet
- Cns Stimulants: Drug Name Class Uses Action Side EffectsDocument6 pagesCns Stimulants: Drug Name Class Uses Action Side EffectsJennifer ViciosoNo ratings yet
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDocument5 pagesProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosNo ratings yet
- UWORLDNCLEXreview2021 090Document100 pagesUWORLDNCLEXreview2021 090lilchibaby3161100% (1)
- 11th 12th STD Standard Class Nursing Health Care Hospital Hygiene Higher Secondary School College NotesDocument5 pages11th 12th STD Standard Class Nursing Health Care Hospital Hygiene Higher Secondary School College NotesRonny IswahyudiNo ratings yet
- High Yield Surgery Compatible Version-2Document20 pagesHigh Yield Surgery Compatible Version-2zoozsuhai2No ratings yet
- PHARMACILOGY SUMMryDocument16 pagesPHARMACILOGY SUMMryKathy Real VillsNo ratings yet
- Drugs in Blood DisordersDocument1 pageDrugs in Blood DisordersSantosh patelNo ratings yet
- Module 4 - Cardiac EmergencyDocument30 pagesModule 4 - Cardiac EmergencyElaine AntonetteNo ratings yet
- CardiovascularDocument34 pagesCardiovascularRianna LarezaNo ratings yet
- Free Planner PDFDocument4 pagesFree Planner PDFcindy crisantaNo ratings yet
- 60 Most Common DrugsDocument1 page60 Most Common DrugsNikkaLim100% (1)
- Pressure InjuriesDocument1 pagePressure InjuriesPaola OrtizNo ratings yet
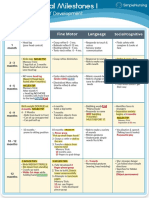
- Visual Chart 1 - Developmental MilestonesDocument1 pageVisual Chart 1 - Developmental MilestonesVishalNo ratings yet
- Breadmaker: Care & Instruction ManualDocument33 pagesBreadmaker: Care & Instruction ManualMichelle Florina PedianiNo ratings yet
- Toast Master NclexDocument13 pagesToast Master NclexAyu CantikaNo ratings yet
- Guide To Diabetes MedicationsDocument2 pagesGuide To Diabetes MedicationsJianhua ShiNo ratings yet
- Week 8 - Lecture Notes For StudentsDocument22 pagesWeek 8 - Lecture Notes For StudentsLoren SarigumbaNo ratings yet
- Medical Emergencies GuidebookDocument211 pagesMedical Emergencies GuidebookNadreen OsmanNo ratings yet
- Electrolytes (3607)Document11 pagesElectrolytes (3607)JennNo ratings yet
- Med Surg 2 - 10 Nursing Care of Clients With Biliary DisordersDocument4 pagesMed Surg 2 - 10 Nursing Care of Clients With Biliary DisordersMaxinne RoseñoNo ratings yet
- Generic: Hydromorphone (SC) Brand Name: DilaudidDocument1 pageGeneric: Hydromorphone (SC) Brand Name: DilaudidPreet ChahalNo ratings yet
- Pharm Expansion 17 NDFDocument1 pagePharm Expansion 17 NDFNokz M. Raki-inNo ratings yet
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- Common Abbreviations For The Patient Note USMLE Step 2CSDocument1 pageCommon Abbreviations For The Patient Note USMLE Step 2CSTiondi francisNo ratings yet
- Syllabus For NclexDocument50 pagesSyllabus For NclexTirthaNo ratings yet
- Physiology Clinical Diagnosis Treatment: TSI AntibodiesDocument10 pagesPhysiology Clinical Diagnosis Treatment: TSI Antibodies85robertNo ratings yet
- OB Med SheetDocument12 pagesOB Med SheetSam DanaNo ratings yet
- High Yield Surgery Compatible VersionDocument77 pagesHigh Yield Surgery Compatible VersionEdgar Soto100% (1)
- Dayly PlannerDocument2 pagesDayly PlannerRuben Dario Rodriguez LopezNo ratings yet
- Health Assessment - Cardiac & PVSDocument56 pagesHealth Assessment - Cardiac & PVSclaire3230No ratings yet
- Fluid and Electrolytes Cram SheetDocument8 pagesFluid and Electrolytes Cram SheetChrizley Shawn DeroniaNo ratings yet
- Dosage CalculationDocument11 pagesDosage Calculationpaulzilicous.artNo ratings yet
- Diets and NutritionDocument19 pagesDiets and Nutritionpaulzilicous.artNo ratings yet
- Immune SystemDocument19 pagesImmune Systempaulzilicous.artNo ratings yet
- Med Surg RevDocument14 pagesMed Surg RevSamantha VeraNo ratings yet
- 12 Drugs Acting On The Cardiovascular SystemDocument7 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- Critical CareDocument21 pagesCritical Carepaulzilicous.artNo ratings yet
- Bundle Fundamentals of Nursing PDFDocument59 pagesBundle Fundamentals of Nursing PDFسلطان محمد فوزي سلمانNo ratings yet
- Med Surge Skills Checklist Inna StreszDocument6 pagesMed Surge Skills Checklist Inna StreszPrecious Angelique MalacatNo ratings yet
- Electrolyte Imbalances Causes: Signs & Symptoms:: Physical Exam: Lab FindingsDocument4 pagesElectrolyte Imbalances Causes: Signs & Symptoms:: Physical Exam: Lab Findingsworleyb83No ratings yet
- SNS (Anti-Cholinergic/adrenergic) : Medical SurgicalDocument50 pagesSNS (Anti-Cholinergic/adrenergic) : Medical Surgicalkimm_nineteenNo ratings yet
- Nervous SystemDocument23 pagesNervous SystemAlliyah SalindoNo ratings yet
- Drug StudyDocument8 pagesDrug StudyZanie CruzNo ratings yet
- Recipes: Bread MakerDocument37 pagesRecipes: Bread MakerJayr Maslog NatorNo ratings yet
- Pharmacology Review For FinalsDocument9 pagesPharmacology Review For FinalsJaya ReyesNo ratings yet
- GastroenterologyDocument59 pagesGastroenterologyActeen MyoseenNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- 2 Fleet EnemaDocument4 pages2 Fleet EnemaCAÑADA, JOHANNELYN M.No ratings yet
- ENEMADocument101 pagesENEMAEmilina AlmenarioNo ratings yet
- Pharma Parenteral Dosage CalculationDocument3 pagesPharma Parenteral Dosage CalculationMaxinne RoseñoNo ratings yet
- Med Surg 2 - 11 Review On The Anatomy and Physiology of The Endocrine SystemDocument3 pagesMed Surg 2 - 11 Review On The Anatomy and Physiology of The Endocrine SystemMaxinne RoseñoNo ratings yet
- Med Surg 2 - 8 Malabsorption Syndromes and Nursing Care of Clients With Hepatic DisordersDocument8 pagesMed Surg 2 - 8 Malabsorption Syndromes and Nursing Care of Clients With Hepatic DisordersMaxinne RoseñoNo ratings yet
- Med Surg 2 - 9 Nursing Care of Clients With Disturbances in DigestionDocument5 pagesMed Surg 2 - 9 Nursing Care of Clients With Disturbances in DigestionMaxinne RoseñoNo ratings yet
- Med Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Document7 pagesMed Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Maxinne RoseñoNo ratings yet
- Med Surg 2 - 10 Nursing Care of Clients With Biliary DisordersDocument4 pagesMed Surg 2 - 10 Nursing Care of Clients With Biliary DisordersMaxinne RoseñoNo ratings yet
- Med Surg 2 - 2 Diagnostic Examinations For Gastrointestinal SystemDocument18 pagesMed Surg 2 - 2 Diagnostic Examinations For Gastrointestinal SystemMaxinne RoseñoNo ratings yet
- Med Surg 2 - 1 Review of Anatomy and Physiology of The GIT and Accessory OrgansDocument8 pagesMed Surg 2 - 1 Review of Anatomy and Physiology of The GIT and Accessory OrgansMaxinne RoseñoNo ratings yet
- Med Surg 2 - 3 Diagnostic Examinations For Gastrointestinal SystemDocument15 pagesMed Surg 2 - 3 Diagnostic Examinations For Gastrointestinal SystemMaxinne RoseñoNo ratings yet
- Med Surg 2 - 5 Malabsorption Sydromes and Nursing Care of Clients With Hepatic DisordersDocument9 pagesMed Surg 2 - 5 Malabsorption Sydromes and Nursing Care of Clients With Hepatic DisordersMaxinne RoseñoNo ratings yet
- Group 1 KuanDocument4 pagesGroup 1 KuanMaxinne RoseñoNo ratings yet
- PDF Spirituality in Nursing Standing On Holy Ground 6Th Edition Mary Elizabeth Obrien Ebook Full ChapterDocument53 pagesPDF Spirituality in Nursing Standing On Holy Ground 6Th Edition Mary Elizabeth Obrien Ebook Full Chaptercarl.jones252100% (1)
- L'Onunei: Module 004 Physical Activity Assessment and StressDocument4 pagesL'Onunei: Module 004 Physical Activity Assessment and StressJoshua V. OlisNo ratings yet
- M1 - NURS341 - 2017-18 - F1 (2) - MergedDocument130 pagesM1 - NURS341 - 2017-18 - F1 (2) - Mergedmariam husseinNo ratings yet
- Nutritional CuresDocument40 pagesNutritional CuresTURGIS100% (2)
- Practice Guidelines For Telemental HealthDocument51 pagesPractice Guidelines For Telemental HealthNataanatiNo ratings yet
- Hatchery Brochure PDFDocument8 pagesHatchery Brochure PDFUmair ShafiqueNo ratings yet
- Pneumonia, Is It Bacterial or Viral FINAL EDITINGDocument31 pagesPneumonia, Is It Bacterial or Viral FINAL EDITINGdv prnt1909No ratings yet
- Cadcor Safety ManualDocument54 pagesCadcor Safety ManualMARY ANN GUEVARRANo ratings yet
- Rle Procedure StudyDocument4 pagesRle Procedure StudyMyangel LoiseNo ratings yet
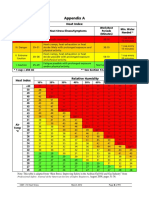
- Part I - 13 Heat Stress 8Document1 pagePart I - 13 Heat Stress 8SKH CultureNo ratings yet
- Form Pre Job MeetingDocument2 pagesForm Pre Job Meetingrian1099No ratings yet
- University of Mindanao - Tagum: Department of Teacher EducationDocument15 pagesUniversity of Mindanao - Tagum: Department of Teacher EducationRESTY ARCAYNANo ratings yet
- UnmadaaDocument34 pagesUnmadaaArathi laxman100% (1)
- Child-Friendly School SurveyDocument3 pagesChild-Friendly School SurveyRobina CariasoNo ratings yet
- Title of Proposal AcronymDocument51 pagesTitle of Proposal AcronymHadish BekuretsionNo ratings yet
- Privação Do SonoDocument3 pagesPrivação Do SonoHugo BarbosaNo ratings yet
- Financiers - Other ContactsDocument8 pagesFinanciers - Other Contactssolnyshko28110705No ratings yet
- Clean Water For AllDocument8 pagesClean Water For AllArgie Joy Marie AmpolNo ratings yet
- Science and Technology Health Writing. J.GALOSDocument25 pagesScience and Technology Health Writing. J.GALOSLance FabreNo ratings yet
- TFN PrelimDocument9 pagesTFN PrelimElla ArnocoNo ratings yet
- Haemorrhoid Review-MainDocument9 pagesHaemorrhoid Review-MainWarren SeowNo ratings yet
- Intellectual Attributes of PersonalityDocument40 pagesIntellectual Attributes of PersonalitycedzmonderoNo ratings yet
- Chapter 5 KleinDocument2 pagesChapter 5 KleinHeartcheNo ratings yet
- DENT 420 Syllabus FINAL 2014-15 - Oct 10 2014 RKDocument34 pagesDENT 420 Syllabus FINAL 2014-15 - Oct 10 2014 RKDraspiNo ratings yet
- Artigo - Randomized Controlled Trial of Mindfulness-Based Stress Reduction Versus AerobicDocument26 pagesArtigo - Randomized Controlled Trial of Mindfulness-Based Stress Reduction Versus AerobicrcsampaNo ratings yet
- Minimally Invasive Cardiac Surgery in Lucknow - Dr. Gauranga MajumdarDocument3 pagesMinimally Invasive Cardiac Surgery in Lucknow - Dr. Gauranga MajumdarBest Heart Bypass Surgery Dr. Gauranga MajumdarNo ratings yet
- The Instability Severity Index ScoreDocument8 pagesThe Instability Severity Index ScoreAndré FariasNo ratings yet
- Medex Academy EssayDocument1 pageMedex Academy Essayapi-592597628No ratings yet