Download as docx, pdf, or txt
You might also like
- Glenda Chidrawi - Sarah Bradstock - Margaret Robson - Elizabeth Thrum - Stephanie Hollis - Sarah Jones - Biology in Focus Year 11-Cengage (2017) PDFDocument440 pagesGlenda Chidrawi - Sarah Bradstock - Margaret Robson - Elizabeth Thrum - Stephanie Hollis - Sarah Jones - Biology in Focus Year 11-Cengage (2017) PDFSebastian Carlos75% (4)
- Ebook Concepts of Genetics 3Rd Edition Brooker Test Bank Full Chapter PDFDocument37 pagesEbook Concepts of Genetics 3Rd Edition Brooker Test Bank Full Chapter PDFelmerthuy6ns76100% (13)
- MELLO, P. C. de - Economics of Labor in Brazilian Coffee Plantations, 1850-1888Document261 pagesMELLO, P. C. de - Economics of Labor in Brazilian Coffee Plantations, 1850-1888Marcos Marinho50% (2)
- Branches of Science and Sub ScienceDocument5 pagesBranches of Science and Sub ScienceJoana E. Gaddawan100% (1)
- Bio Factsheet: The Kidney: Excretion and OsmoregulationDocument4 pagesBio Factsheet: The Kidney: Excretion and OsmoregulationjesvinjesvinNo ratings yet
- Chloroplast, PPTDocument21 pagesChloroplast, PPTSuchitra Sk88% (8)
- Pathogenesis of Glaucoma: Determinants of Intraocular PressureDocument17 pagesPathogenesis of Glaucoma: Determinants of Intraocular PressureAdi TriNo ratings yet
- Understanding Trabecular Meshwork Physiology: A Key To The Control of Intraocular Pressure?Document5 pagesUnderstanding Trabecular Meshwork Physiology: A Key To The Control of Intraocular Pressure?RaissaNo ratings yet
- Physiology of Aqueous HumorDocument34 pagesPhysiology of Aqueous HumorCindy Seow Sieng TengNo ratings yet
- Discuss Physiology of Aqueous Formation and Its Drainage and Relate It To How Intraocular Pressure Is ControlledDocument8 pagesDiscuss Physiology of Aqueous Formation and Its Drainage and Relate It To How Intraocular Pressure Is ControlledPrince ChipunguNo ratings yet
- Aquas Humor DynamicsDocument30 pagesAquas Humor DynamicsRatnesh ShuklaNo ratings yet
- Anterior ChamberDocument11 pagesAnterior Chamberhanidya fazwatNo ratings yet
- Aqueous HumorDocument46 pagesAqueous HumorJ NATASHA MARIANo ratings yet
- Glaucoma EssayDocument5 pagesGlaucoma Essaysujataravi6No ratings yet
- Cornea PhysiologyDocument76 pagesCornea Physiologydr_dev50% (2)
- Aqueous Humor Dynamics (DR Poonam)Document28 pagesAqueous Humor Dynamics (DR Poonam)Sampitroda DesaiNo ratings yet
- Dr. Padmaja PhadeDocument46 pagesDr. Padmaja PhadeElaine ChongNo ratings yet
- Functional MorphologyDocument12 pagesFunctional MorphologyNelly ElizabethNo ratings yet
- VitreousDocument37 pagesVitreousIhsanluthfi AbdillahNo ratings yet
- Understanding Trabecular Meshwork Physiology: A Key To The Control of Intraocular Pressure?Document5 pagesUnderstanding Trabecular Meshwork Physiology: A Key To The Control of Intraocular Pressure?Nail AlheloNo ratings yet
- Congestive Cardiac FalureDocument57 pagesCongestive Cardiac FalurelightningiceNo ratings yet
- VisionDocument199 pagesVisionAshtami Satheesh 2007No ratings yet
- CNUR823 - Module 2Document26 pagesCNUR823 - Module 2AumNo ratings yet
- Anatomy and Pa Tho Physiology of Aqueous Production and OutflowDocument34 pagesAnatomy and Pa Tho Physiology of Aqueous Production and OutflowChristine TanNo ratings yet
- Pathophysiology of KidneysDocument35 pagesPathophysiology of KidneysAli Aborges Jr.No ratings yet
- 25.4 Microscopic Anatomy of The Kidney - Anatomy and Physiology 2e - OpenStaxDocument5 pages25.4 Microscopic Anatomy of The Kidney - Anatomy and Physiology 2e - OpenStaxMarlene AngwaforNo ratings yet
- The Multifunctional ChoroidDocument38 pagesThe Multifunctional ChoroidyinvilllNo ratings yet
- 1 Body FluidsDocument9 pages1 Body FluidsSenthereng MoaisiNo ratings yet
- GlaucomaDocument57 pagesGlaucomaAmmad ShahidNo ratings yet
- 11.3 - The KidneyDocument7 pages11.3 - The KidneyraghadNo ratings yet
- Celulas Müller EdemaDocument10 pagesCelulas Müller EdemaOrielle RocioNo ratings yet
- Emergency Fluid TherapyDocument7 pagesEmergency Fluid TherapyAnaNo ratings yet
- Pathophysiology of Body Fluids: Mansyur Arif, MD, PHDDocument14 pagesPathophysiology of Body Fluids: Mansyur Arif, MD, PHDLIEBERKHUNNo ratings yet
- Assignment 2022 B213298B OPTC201Document4 pagesAssignment 2022 B213298B OPTC201Kudzai RusereNo ratings yet
- 24circulation Part 2Document11 pages24circulation Part 2Jaydave PatelNo ratings yet
- A Level Biology NotesDocument6 pagesA Level Biology NotesMira AluedeNo ratings yet
- Fluid Therapy Options and Rational SelectionDocument13 pagesFluid Therapy Options and Rational SelectionRoberto López MataNo ratings yet
- Microcirculation & Lymphatics - New-1Document23 pagesMicrocirculation & Lymphatics - New-1Danial HaiderNo ratings yet
- Urine Concentration and DilutionDocument7 pagesUrine Concentration and DilutionHussein Ali AljamaliNo ratings yet
- Fluid and Electrolytes - MTDocument14 pagesFluid and Electrolytes - MTAlliah Polvorido AnaudNo ratings yet
- Harvade College of Science, Business and Management Studies Polt 1-12, Harvade Close, Off Obada Road Abeokuta Ogun StateDocument21 pagesHarvade College of Science, Business and Management Studies Polt 1-12, Harvade Close, Off Obada Road Abeokuta Ogun StateOluwaseun TosinNo ratings yet
- Aqueous Humour: Anatomy & Physiology: by Tahir Muneeb - September 7, 2012 6 3502Document9 pagesAqueous Humour: Anatomy & Physiology: by Tahir Muneeb - September 7, 2012 6 3502nnurulhudaaNo ratings yet
- Kidney 3Document4 pagesKidney 3rsnsl7410No ratings yet
- Bonanno 2001Document8 pagesBonanno 2001soranydNo ratings yet
- Diuretics: Dr. Ashley M. StokesDocument26 pagesDiuretics: Dr. Ashley M. StokesDhaif dhaifNo ratings yet
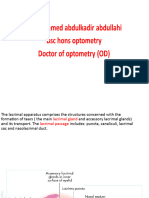
- L5 Lacrimal ApparatousDocument28 pagesL5 Lacrimal ApparatousX And ZNo ratings yet
- Anatomy and Physiology of Cornea: Dr. Joseph JohnDocument46 pagesAnatomy and Physiology of Cornea: Dr. Joseph JohnBIBI MOHANAN100% (1)
- Johnson Ta MM 2010Document10 pagesJohnson Ta MM 2010Lewi Esther SiahaanNo ratings yet
- Hydrostatic Pressure and Colloid Osmotic Pressure QuestionsDocument2 pagesHydrostatic Pressure and Colloid Osmotic Pressure QuestionsCorinneNo ratings yet
- Ocular Biochemistry LECTURE NOTE-1Document44 pagesOcular Biochemistry LECTURE NOTE-1Divine OkolieNo ratings yet
- Excretion (Continued)Document9 pagesExcretion (Continued)t0000123No ratings yet
- Anatomy of Anterior Chamber Angle and Physiology ofDocument24 pagesAnatomy of Anterior Chamber Angle and Physiology ofAnumeha Jindal100% (1)
- Cerebro Spinal Fluid and The Meninges: Dr. Setyawati Asih Putri, SPS, M.Kes, FinaDocument30 pagesCerebro Spinal Fluid and The Meninges: Dr. Setyawati Asih Putri, SPS, M.Kes, FinakhairaniNo ratings yet
- Urinary System EditedDocument8 pagesUrinary System EditedJanith VimukthiNo ratings yet
- A Level Transport FinestDocument25 pagesA Level Transport FinestBaguma alexNo ratings yet
- Capitulo 6 Dinamica Humor AcuosoDocument10 pagesCapitulo 6 Dinamica Humor AcuosoLuisa Mayta PitmanNo ratings yet
- CSF Meningen PPTUNIZARDocument29 pagesCSF Meningen PPTUNIZARrinaldy IX9No ratings yet
- Kidneys and UrineDocument8 pagesKidneys and UrineMira ChotaiNo ratings yet
- Distal Convoluted Tubules, Counter Current Mechanism, MicturitionDocument94 pagesDistal Convoluted Tubules, Counter Current Mechanism, MicturitionSarah BirechNo ratings yet
- Liquido IntersticialDocument15 pagesLiquido IntersticialSofia BelénNo ratings yet
- 1-Anatomy of The Eye BallDocument6 pages1-Anatomy of The Eye BalltressNo ratings yet
- Urine FormationDocument49 pagesUrine FormationCor GuerreroNo ratings yet
- Chapter 16Document9 pagesChapter 16g_komolafeNo ratings yet
- Suprachoroidal Space InterventionsFrom EverandSuprachoroidal Space InterventionsShohista SaidkasimovaNo ratings yet
- Microcirculation of Blood 101: The Next Generation of HealthcareFrom EverandMicrocirculation of Blood 101: The Next Generation of HealthcareNo ratings yet
- English TOEFL Ets TOEFL Preparation Kit Volume 2 Practice Test C SW CompressDocument6 pagesEnglish TOEFL Ets TOEFL Preparation Kit Volume 2 Practice Test C SW CompressGitz OfficialNo ratings yet
- The Sentient Cell The Cellular Foundations of Consciousness Arthur S Reber Full ChapterDocument67 pagesThe Sentient Cell The Cellular Foundations of Consciousness Arthur S Reber Full Chapterwade.escamilla468100% (6)
- Gap FillingDocument21 pagesGap Fillingmarycathrin1973No ratings yet
- ANTHRO PYQs - 1985-2023Document59 pagesANTHRO PYQs - 1985-2023RajNo ratings yet
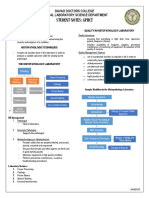
- Student Notes: GPHCT: Davao Doctors College Medical Laboratory Science DepartmentDocument7 pagesStudent Notes: GPHCT: Davao Doctors College Medical Laboratory Science DepartmentFedz FederisoNo ratings yet
- Number 1 9a9 9a7 28december 2023Document9 pagesNumber 1 9a9 9a7 28december 2023Phạm Quang HuyNo ratings yet
- Q4 STEM General Biology 2 Week 3Document4 pagesQ4 STEM General Biology 2 Week 3ralphNo ratings yet
- Test Bank For Human Genetics 10 Edition Ricki LewisDocument36 pagesTest Bank For Human Genetics 10 Edition Ricki Lewissloppy.obsidian.v8ovu100% (47)
- Sci 10 Unit 3 Mod 1 (Lecture)Document45 pagesSci 10 Unit 3 Mod 1 (Lecture)Jonessa BenignosNo ratings yet
- Cell Kinetics and Fermenter DesignDocument64 pagesCell Kinetics and Fermenter Designabdisa767No ratings yet
- Lecture 3connective TissueDocument20 pagesLecture 3connective TissueMohit SharmaNo ratings yet
- Department of Education: Republic of The PhilippinesDocument5 pagesDepartment of Education: Republic of The Philippinesmaricar relator100% (1)
- Psychology As A ScienceDocument15 pagesPsychology As A ScienceUrwa Tul WosqaNo ratings yet
- B94 - EAP Course 14th MeetingDocument6 pagesB94 - EAP Course 14th Meeting28 MeisyafaNo ratings yet
- Pub - Encyclopedia of Genetics Genomics Proteomics and B PDFDocument4,046 pagesPub - Encyclopedia of Genetics Genomics Proteomics and B PDFraj252000100% (1)
- MCQs of Biology Book of Class IXDocument25 pagesMCQs of Biology Book of Class IXShazil HameedNo ratings yet
- Ebook PDF The Science of Agriculture A Biological Approach 5th Edition PDFDocument41 pagesEbook PDF The Science of Agriculture A Biological Approach 5th Edition PDFmarilyn.trojanowski475100% (39)
- Bicoid Is A: Operator DNA TranscriptionDocument3 pagesBicoid Is A: Operator DNA TranscriptionNiño Matthew Fetalvero RiojaNo ratings yet
- Coek - Info - Neurocomputing Foundations of ResearchDocument5 pagesCoek - Info - Neurocomputing Foundations of Researchkgdeepak122950No ratings yet
- Analisis Faktor Eksploitasi Hutan Di Iuphhk-Ha PT Bina Multi Alam LestariDocument8 pagesAnalisis Faktor Eksploitasi Hutan Di Iuphhk-Ha PT Bina Multi Alam LestariNadyaNo ratings yet
- Chapter 6 Types of Tissue CultureDocument129 pagesChapter 6 Types of Tissue Culturerajiv pathakNo ratings yet
- HYDRAGEL ß1-ß2 HydrasisDocument11 pagesHYDRAGEL ß1-ß2 HydrasisAli AlloNo ratings yet
- Annotated-Scopes Trial Student MaterialsDocument8 pagesAnnotated-Scopes Trial Student MaterialsBernardo ThenNo ratings yet
- Parts of Plant Cell and Its FunctionsDocument2 pagesParts of Plant Cell and Its FunctionsThiody Hope Mongas50% (2)
- Maintenance and Preservation of Microbial CulturesDocument5 pagesMaintenance and Preservation of Microbial CulturesSumit KumarNo ratings yet