
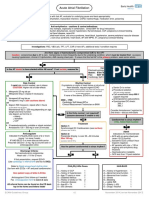
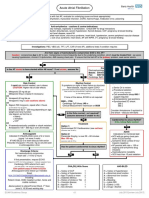
Pathway DIAGNOSIS OF PAF FTR
Pathway DIAGNOSIS OF PAF FTR
You might also like
- From Blue Nines and Red WordsDocument6 pagesFrom Blue Nines and Red Wordsabunour50% (4)
- Ebook PDF - Forbidden Healing - Curiously Simple Solution To Disease by Capt TC RandallDocument351 pagesEbook PDF - Forbidden Healing - Curiously Simple Solution To Disease by Capt TC RandallEbook Pdf100% (6)
- Acute FiaDocument2 pagesAcute FiaAndrei MurariuNo ratings yet
- Treatment Strategies For Pulmonary HypertensionDocument32 pagesTreatment Strategies For Pulmonary Hypertensiondoc_chestNo ratings yet
- Management VasculopatyDocument23 pagesManagement VasculopatyAgus SusantoNo ratings yet
- Atrial Fibrillation (AF) & Flutter Complicating Critical IllnessDocument29 pagesAtrial Fibrillation (AF) & Flutter Complicating Critical IllnessMohammed SadoonNo ratings yet
- Class IC Antiarrhythmics (Na+ Channel Blockers) : Play PicmonicDocument2 pagesClass IC Antiarrhythmics (Na+ Channel Blockers) : Play PicmonicNkurunziza BenjamineNo ratings yet
- Management of Atrial Fibrillation: Speaker: Ri. 張家銘 2003/4/14 According to 2001 AHA practice guidelineDocument52 pagesManagement of Atrial Fibrillation: Speaker: Ri. 張家銘 2003/4/14 According to 2001 AHA practice guidelinealgadarazizNo ratings yet
- Atrial Fibrillation: Prapa KanagaratnamDocument25 pagesAtrial Fibrillation: Prapa KanagaratnamRohit BasuthkarNo ratings yet
- Clinical Approach To AFDocument32 pagesClinical Approach To AFEmdan SengadjiNo ratings yet
- Acute Fia2Document2 pagesAcute Fia2Andrei MurariuNo ratings yet
- Adrenergic - Antagonists TableDocument3 pagesAdrenergic - Antagonists Tablehovico3936No ratings yet
- Op-Ehea210701 4740..4742Document3 pagesOp-Ehea210701 4740..4742Luis Fernando Morales JuradoNo ratings yet
- Prescribing in Chest PainDocument4 pagesPrescribing in Chest PainYY_1992No ratings yet
- Antagonis AdrenergikDocument34 pagesAntagonis AdrenergikGde Ananda ArmanditaNo ratings yet
- Graded Concept Map 2Document1 pageGraded Concept Map 2api-727701816No ratings yet
- Atrial Arrthymia WithoutDocument16 pagesAtrial Arrthymia Withoutapi-716714980No ratings yet
- HFpEF Management 2023Document10 pagesHFpEF Management 2023ctsakalakisNo ratings yet
- Alpha Blocker Indications: 1. Nonselective Alpha-Blockers (Alpha-1 and Alpha-2)Document3 pagesAlpha Blocker Indications: 1. Nonselective Alpha-Blockers (Alpha-1 and Alpha-2)Erick DjuandaNo ratings yet
- 3rd Year PharmacologyDocument43 pages3rd Year PharmacologyShayeeshan SivapalarajahNo ratings yet
- Hybrid Rhythm Control Therapy: 12.1 Combining Antiarrhythmic Drugs and Catheter AblationDocument14 pagesHybrid Rhythm Control Therapy: 12.1 Combining Antiarrhythmic Drugs and Catheter AblationFarah MuthiaNo ratings yet
- CARDIOVASCULARDocument2 pagesCARDIOVASCULARAERONH JOHN PURIFICANDONo ratings yet
- 874 FullDocument10 pages874 FullindraNo ratings yet
- Results of Maze Surgery For Lone Paroxysmal Atrial FibrillationDocument9 pagesResults of Maze Surgery For Lone Paroxysmal Atrial Fibrillationapi-684047665No ratings yet
- Pharmacology Notes Ali RazaDocument18 pagesPharmacology Notes Ali Razaurwaafghan48No ratings yet
- Frequently Used Medical AbbreviationsDocument10 pagesFrequently Used Medical AbbreviationsdunareagalatiNo ratings yet
- Hipertension and Heart Failure - FullDocument3 pagesHipertension and Heart Failure - FullRichardNo ratings yet
- StrokeTIA Clinic Crozer 2022Document1 pageStrokeTIA Clinic Crozer 2022Franky QNo ratings yet
- AmlodipineDocument2 pagesAmlodipinejiglenssNo ratings yet
- Peripartun CardiomyopathyDocument19 pagesPeripartun CardiomyopathyRidyah Ning TyasNo ratings yet
- Reference ID: 3115694: Rev. T 1/2012Document2 pagesReference ID: 3115694: Rev. T 1/2012Gloria CintronNo ratings yet
- Suspected Heart Failure: Section 5 Section 7 Section 8Document10 pagesSuspected Heart Failure: Section 5 Section 7 Section 8Javier TapiaNo ratings yet
- Unit Ii: Drugs For Arrhythmia: ObjectivesDocument3 pagesUnit Ii: Drugs For Arrhythmia: ObjectivesJosa Camille BungayNo ratings yet
- Booklet 2018Document34 pagesBooklet 2018BaluErnestoNo ratings yet
- Rate Versus Rhythm Control in Atrial Fibrillation: RxfilesDocument8 pagesRate Versus Rhythm Control in Atrial Fibrillation: RxfilesMuhammad SafaatNo ratings yet
- Fibrillazione AtrialeDocument66 pagesFibrillazione AtrialeRiccardo ArmellinNo ratings yet
- Guidelines For The Management of Atrial Fibrillation Part-IIDocument66 pagesGuidelines For The Management of Atrial Fibrillation Part-IIJamil Muqtadir BhattiNo ratings yet
- Emerging Therapies in Hfpef 3Document64 pagesEmerging Therapies in Hfpef 3api-588254706No ratings yet
- Nclex Pharm ReviewDocument10 pagesNclex Pharm ReviewRuiqi YangNo ratings yet
- Prehospital Care: Immediate Interventions - AbcsDocument8 pagesPrehospital Care: Immediate Interventions - AbcsindahkurNo ratings yet
- Atrial Fibrillation: Dr. Zirath + Dr. MehtaDocument29 pagesAtrial Fibrillation: Dr. Zirath + Dr. MehtaAjayNo ratings yet
- NIV Algorithm Final Version Jan 2020Document3 pagesNIV Algorithm Final Version Jan 2020AmalNo ratings yet
- PPP305 LA10 08052024 ArrhythmiaDocument37 pagesPPP305 LA10 08052024 Arrhythmiagadk555No ratings yet
- SympatholyticsDocument46 pagesSympatholyticsHari Kamesh KiranNo ratings yet
- Anti Arrhythmic 3 PDFDocument25 pagesAnti Arrhythmic 3 PDFVijay SharmaNo ratings yet
- Capuano 2015Document5 pagesCapuano 2015bpNo ratings yet
- Atrial Fibrillation HandoutDocument5 pagesAtrial Fibrillation HandoutAlfa AlfinNo ratings yet
- Heart Failure With Reduced Ejection FractionDocument11 pagesHeart Failure With Reduced Ejection Fractionpricilia ardianiNo ratings yet
- Atrial Fibrillation: Sanchit TuragaDocument17 pagesAtrial Fibrillation: Sanchit TuragaarianNo ratings yet
- Heart Failure (Paska)Document28 pagesHeart Failure (Paska)myoganoNo ratings yet
- Acute Antipsychotic-Induced Akathisia Revisited: EditorialDocument4 pagesAcute Antipsychotic-Induced Akathisia Revisited: EditorialMaharaniDewiNo ratings yet
- Pharmacology Cardiovascular DrugsDocument27 pagesPharmacology Cardiovascular DrugsMitzel AlvaranNo ratings yet
- 21 9 1034Document6 pages21 9 1034Marcela MurafaNo ratings yet
- Respiratory MedicationDocument4 pagesRespiratory MedicationShang MacarayonNo ratings yet
- Drugs Given During Cardiac Arres For CPRDocument5 pagesDrugs Given During Cardiac Arres For CPREevyaj MimiNo ratings yet
- AHA ASA CVD NH and TIA Prevention 2021 - RemovedDocument4 pagesAHA ASA CVD NH and TIA Prevention 2021 - RemovedAulia Rahmat PaingNo ratings yet
- AF2Document41 pagesAF2Rudy Arindra WijayaNo ratings yet
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocument7 pagesPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
- DR - TrisuloDocument35 pagesDR - TrisuloZaky prasetyaNo ratings yet
- Drug Study inDocument3 pagesDrug Study inaycee0316No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Laporan Nod Malam TGL 15 Mei 2023Document5 pagesLaporan Nod Malam TGL 15 Mei 2023Yoan Eka Putra PalilingNo ratings yet
- Pengajuan Kekurangan Project GS LT 11Document16 pagesPengajuan Kekurangan Project GS LT 11Yoan Eka Putra PalilingNo ratings yet
- Case Study 1Document49 pagesCase Study 1Yoan Eka Putra PalilingNo ratings yet
- WSC 2022 Preliminary Program June Updated WebsiteDocument3 pagesWSC 2022 Preliminary Program June Updated WebsiteYoan Eka Putra PalilingNo ratings yet
- Carpal Tunnel SyndromeDocument9 pagesCarpal Tunnel SyndromeMaha RajaNo ratings yet
- Shang Han LunDocument94 pagesShang Han LunDENo ratings yet
- ISNTC Safety Guideline For The Prevention of COVID 19 in The Training Center PDFDocument1 pageISNTC Safety Guideline For The Prevention of COVID 19 in The Training Center PDFWarren GronaNo ratings yet
- Employee Application Form Parkside 2-4Document5 pagesEmployee Application Form Parkside 2-4dimasfavehotelNo ratings yet
- Posterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentDocument8 pagesPosterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentNegru TeodorNo ratings yet
- Past Life RegressionDocument8 pagesPast Life RegressionGabriel AndradeNo ratings yet
- Activity 6 - Group A - 1EDocument3 pagesActivity 6 - Group A - 1EEazel SolanaNo ratings yet
- Ehlers Danlos SyndromeDocument3 pagesEhlers Danlos SyndromeBonnie MacDonaldNo ratings yet
- Untitled DocumentDocument11 pagesUntitled Documentapi-669702575No ratings yet
- Nurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueDocument7 pagesNurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueIndry LabungasaNo ratings yet
- Basic First Aid: Kristoffer G. Villareal RN, LPTDocument23 pagesBasic First Aid: Kristoffer G. Villareal RN, LPTTopz VillarealNo ratings yet
- Chilhood2.0 AnalysisAndCritiqueDocument2 pagesChilhood2.0 AnalysisAndCritiqueYukaNo ratings yet
- Anatomy of Brain and Function - NaemaDocument7 pagesAnatomy of Brain and Function - NaemaHana Naema ZelinNo ratings yet
- Hydrogen Peroxide Magic - Thacker.bDocument209 pagesHydrogen Peroxide Magic - Thacker.bMathieu ChautardNo ratings yet
- PotakaDocument6 pagesPotakaTrisha Olila CasimeroNo ratings yet
- Prevalence of Fluorosis in Nalgonda DistrictDocument18 pagesPrevalence of Fluorosis in Nalgonda DistrictViswa NathanNo ratings yet
- List of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityDocument33 pagesList of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityJurryNo ratings yet
- DR Vernon Coleman - Coronavirus Will Social Distancing Be PermanentDocument4 pagesDR Vernon Coleman - Coronavirus Will Social Distancing Be PermanentGeorge KourisNo ratings yet
- Drug Study: AmoxicillinDocument3 pagesDrug Study: AmoxicillinKrzia TehNo ratings yet
- Acute ConfusionDocument7 pagesAcute ConfusionYasin JazNo ratings yet
- Handbook of Clinical Anaesthesia, Fourth EditionDocument2 pagesHandbook of Clinical Anaesthesia, Fourth EditionHany ElbarougyNo ratings yet
- Intro To Child Psychology - Module 1Document8 pagesIntro To Child Psychology - Module 1Jessielle100% (1)
- By Dr. AlabastroDocument9 pagesBy Dr. Alabastro2013SecBNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- Theory of Cultural Care and DiversityDocument16 pagesTheory of Cultural Care and DiversityJunne Rafaela NovalNo ratings yet
- Role of The Social Worker in The Outbreak of Pandemics A Case of COVID 19Document8 pagesRole of The Social Worker in The Outbreak of Pandemics A Case of COVID 19Rahul KhannaNo ratings yet
- Atellica NEPH 630 Brochure FINAL 152098222Document4 pagesAtellica NEPH 630 Brochure FINAL 152098222Ahmed MostafaNo ratings yet
- Step 2 Clinical Knowledge (CK) : Sample Test QuestionsDocument55 pagesStep 2 Clinical Knowledge (CK) : Sample Test QuestionsDr.Mohammed N. AbedNo ratings yet


























































































Download as pdf or txt
You might also like
- From Blue Nines and Red WordsDocument6 pagesFrom Blue Nines and Red Wordsabunour50% (4)
- Ebook PDF - Forbidden Healing - Curiously Simple Solution To Disease by Capt TC RandallDocument351 pagesEbook PDF - Forbidden Healing - Curiously Simple Solution To Disease by Capt TC RandallEbook Pdf100% (6)
- Acute FiaDocument2 pagesAcute FiaAndrei MurariuNo ratings yet
- Treatment Strategies For Pulmonary HypertensionDocument32 pagesTreatment Strategies For Pulmonary Hypertensiondoc_chestNo ratings yet
- Management VasculopatyDocument23 pagesManagement VasculopatyAgus SusantoNo ratings yet
- Atrial Fibrillation (AF) & Flutter Complicating Critical IllnessDocument29 pagesAtrial Fibrillation (AF) & Flutter Complicating Critical IllnessMohammed SadoonNo ratings yet
- Class IC Antiarrhythmics (Na+ Channel Blockers) : Play PicmonicDocument2 pagesClass IC Antiarrhythmics (Na+ Channel Blockers) : Play PicmonicNkurunziza BenjamineNo ratings yet
- Management of Atrial Fibrillation: Speaker: Ri. 張家銘 2003/4/14 According to 2001 AHA practice guidelineDocument52 pagesManagement of Atrial Fibrillation: Speaker: Ri. 張家銘 2003/4/14 According to 2001 AHA practice guidelinealgadarazizNo ratings yet
- Atrial Fibrillation: Prapa KanagaratnamDocument25 pagesAtrial Fibrillation: Prapa KanagaratnamRohit BasuthkarNo ratings yet
- Clinical Approach To AFDocument32 pagesClinical Approach To AFEmdan SengadjiNo ratings yet
- Acute Fia2Document2 pagesAcute Fia2Andrei MurariuNo ratings yet
- Adrenergic - Antagonists TableDocument3 pagesAdrenergic - Antagonists Tablehovico3936No ratings yet
- Op-Ehea210701 4740..4742Document3 pagesOp-Ehea210701 4740..4742Luis Fernando Morales JuradoNo ratings yet
- Prescribing in Chest PainDocument4 pagesPrescribing in Chest PainYY_1992No ratings yet
- Antagonis AdrenergikDocument34 pagesAntagonis AdrenergikGde Ananda ArmanditaNo ratings yet
- Graded Concept Map 2Document1 pageGraded Concept Map 2api-727701816No ratings yet
- Atrial Arrthymia WithoutDocument16 pagesAtrial Arrthymia Withoutapi-716714980No ratings yet
- HFpEF Management 2023Document10 pagesHFpEF Management 2023ctsakalakisNo ratings yet
- Alpha Blocker Indications: 1. Nonselective Alpha-Blockers (Alpha-1 and Alpha-2)Document3 pagesAlpha Blocker Indications: 1. Nonselective Alpha-Blockers (Alpha-1 and Alpha-2)Erick DjuandaNo ratings yet
- 3rd Year PharmacologyDocument43 pages3rd Year PharmacologyShayeeshan SivapalarajahNo ratings yet
- Hybrid Rhythm Control Therapy: 12.1 Combining Antiarrhythmic Drugs and Catheter AblationDocument14 pagesHybrid Rhythm Control Therapy: 12.1 Combining Antiarrhythmic Drugs and Catheter AblationFarah MuthiaNo ratings yet
- CARDIOVASCULARDocument2 pagesCARDIOVASCULARAERONH JOHN PURIFICANDONo ratings yet
- 874 FullDocument10 pages874 FullindraNo ratings yet
- Results of Maze Surgery For Lone Paroxysmal Atrial FibrillationDocument9 pagesResults of Maze Surgery For Lone Paroxysmal Atrial Fibrillationapi-684047665No ratings yet
- Pharmacology Notes Ali RazaDocument18 pagesPharmacology Notes Ali Razaurwaafghan48No ratings yet
- Frequently Used Medical AbbreviationsDocument10 pagesFrequently Used Medical AbbreviationsdunareagalatiNo ratings yet
- Hipertension and Heart Failure - FullDocument3 pagesHipertension and Heart Failure - FullRichardNo ratings yet
- StrokeTIA Clinic Crozer 2022Document1 pageStrokeTIA Clinic Crozer 2022Franky QNo ratings yet
- AmlodipineDocument2 pagesAmlodipinejiglenssNo ratings yet
- Peripartun CardiomyopathyDocument19 pagesPeripartun CardiomyopathyRidyah Ning TyasNo ratings yet
- Reference ID: 3115694: Rev. T 1/2012Document2 pagesReference ID: 3115694: Rev. T 1/2012Gloria CintronNo ratings yet
- Suspected Heart Failure: Section 5 Section 7 Section 8Document10 pagesSuspected Heart Failure: Section 5 Section 7 Section 8Javier TapiaNo ratings yet
- Unit Ii: Drugs For Arrhythmia: ObjectivesDocument3 pagesUnit Ii: Drugs For Arrhythmia: ObjectivesJosa Camille BungayNo ratings yet
- Booklet 2018Document34 pagesBooklet 2018BaluErnestoNo ratings yet
- Rate Versus Rhythm Control in Atrial Fibrillation: RxfilesDocument8 pagesRate Versus Rhythm Control in Atrial Fibrillation: RxfilesMuhammad SafaatNo ratings yet
- Fibrillazione AtrialeDocument66 pagesFibrillazione AtrialeRiccardo ArmellinNo ratings yet
- Guidelines For The Management of Atrial Fibrillation Part-IIDocument66 pagesGuidelines For The Management of Atrial Fibrillation Part-IIJamil Muqtadir BhattiNo ratings yet
- Emerging Therapies in Hfpef 3Document64 pagesEmerging Therapies in Hfpef 3api-588254706No ratings yet
- Nclex Pharm ReviewDocument10 pagesNclex Pharm ReviewRuiqi YangNo ratings yet
- Prehospital Care: Immediate Interventions - AbcsDocument8 pagesPrehospital Care: Immediate Interventions - AbcsindahkurNo ratings yet
- Atrial Fibrillation: Dr. Zirath + Dr. MehtaDocument29 pagesAtrial Fibrillation: Dr. Zirath + Dr. MehtaAjayNo ratings yet
- NIV Algorithm Final Version Jan 2020Document3 pagesNIV Algorithm Final Version Jan 2020AmalNo ratings yet
- PPP305 LA10 08052024 ArrhythmiaDocument37 pagesPPP305 LA10 08052024 Arrhythmiagadk555No ratings yet
- SympatholyticsDocument46 pagesSympatholyticsHari Kamesh KiranNo ratings yet
- Anti Arrhythmic 3 PDFDocument25 pagesAnti Arrhythmic 3 PDFVijay SharmaNo ratings yet
- Capuano 2015Document5 pagesCapuano 2015bpNo ratings yet
- Atrial Fibrillation HandoutDocument5 pagesAtrial Fibrillation HandoutAlfa AlfinNo ratings yet
- Heart Failure With Reduced Ejection FractionDocument11 pagesHeart Failure With Reduced Ejection Fractionpricilia ardianiNo ratings yet
- Atrial Fibrillation: Sanchit TuragaDocument17 pagesAtrial Fibrillation: Sanchit TuragaarianNo ratings yet
- Heart Failure (Paska)Document28 pagesHeart Failure (Paska)myoganoNo ratings yet
- Acute Antipsychotic-Induced Akathisia Revisited: EditorialDocument4 pagesAcute Antipsychotic-Induced Akathisia Revisited: EditorialMaharaniDewiNo ratings yet
- Pharmacology Cardiovascular DrugsDocument27 pagesPharmacology Cardiovascular DrugsMitzel AlvaranNo ratings yet
- 21 9 1034Document6 pages21 9 1034Marcela MurafaNo ratings yet
- Respiratory MedicationDocument4 pagesRespiratory MedicationShang MacarayonNo ratings yet
- Drugs Given During Cardiac Arres For CPRDocument5 pagesDrugs Given During Cardiac Arres For CPREevyaj MimiNo ratings yet
- AHA ASA CVD NH and TIA Prevention 2021 - RemovedDocument4 pagesAHA ASA CVD NH and TIA Prevention 2021 - RemovedAulia Rahmat PaingNo ratings yet
- AF2Document41 pagesAF2Rudy Arindra WijayaNo ratings yet
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocument7 pagesPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
- DR - TrisuloDocument35 pagesDR - TrisuloZaky prasetyaNo ratings yet
- Drug Study inDocument3 pagesDrug Study inaycee0316No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Laporan Nod Malam TGL 15 Mei 2023Document5 pagesLaporan Nod Malam TGL 15 Mei 2023Yoan Eka Putra PalilingNo ratings yet
- Pengajuan Kekurangan Project GS LT 11Document16 pagesPengajuan Kekurangan Project GS LT 11Yoan Eka Putra PalilingNo ratings yet
- Case Study 1Document49 pagesCase Study 1Yoan Eka Putra PalilingNo ratings yet
- WSC 2022 Preliminary Program June Updated WebsiteDocument3 pagesWSC 2022 Preliminary Program June Updated WebsiteYoan Eka Putra PalilingNo ratings yet
- Carpal Tunnel SyndromeDocument9 pagesCarpal Tunnel SyndromeMaha RajaNo ratings yet
- Shang Han LunDocument94 pagesShang Han LunDENo ratings yet
- ISNTC Safety Guideline For The Prevention of COVID 19 in The Training Center PDFDocument1 pageISNTC Safety Guideline For The Prevention of COVID 19 in The Training Center PDFWarren GronaNo ratings yet
- Employee Application Form Parkside 2-4Document5 pagesEmployee Application Form Parkside 2-4dimasfavehotelNo ratings yet
- Posterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentDocument8 pagesPosterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentNegru TeodorNo ratings yet
- Past Life RegressionDocument8 pagesPast Life RegressionGabriel AndradeNo ratings yet
- Activity 6 - Group A - 1EDocument3 pagesActivity 6 - Group A - 1EEazel SolanaNo ratings yet
- Ehlers Danlos SyndromeDocument3 pagesEhlers Danlos SyndromeBonnie MacDonaldNo ratings yet
- Untitled DocumentDocument11 pagesUntitled Documentapi-669702575No ratings yet
- Nurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueDocument7 pagesNurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueIndry LabungasaNo ratings yet
- Basic First Aid: Kristoffer G. Villareal RN, LPTDocument23 pagesBasic First Aid: Kristoffer G. Villareal RN, LPTTopz VillarealNo ratings yet
- Chilhood2.0 AnalysisAndCritiqueDocument2 pagesChilhood2.0 AnalysisAndCritiqueYukaNo ratings yet
- Anatomy of Brain and Function - NaemaDocument7 pagesAnatomy of Brain and Function - NaemaHana Naema ZelinNo ratings yet
- Hydrogen Peroxide Magic - Thacker.bDocument209 pagesHydrogen Peroxide Magic - Thacker.bMathieu ChautardNo ratings yet
- PotakaDocument6 pagesPotakaTrisha Olila CasimeroNo ratings yet
- Prevalence of Fluorosis in Nalgonda DistrictDocument18 pagesPrevalence of Fluorosis in Nalgonda DistrictViswa NathanNo ratings yet
- List of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityDocument33 pagesList of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityJurryNo ratings yet
- DR Vernon Coleman - Coronavirus Will Social Distancing Be PermanentDocument4 pagesDR Vernon Coleman - Coronavirus Will Social Distancing Be PermanentGeorge KourisNo ratings yet
- Drug Study: AmoxicillinDocument3 pagesDrug Study: AmoxicillinKrzia TehNo ratings yet
- Acute ConfusionDocument7 pagesAcute ConfusionYasin JazNo ratings yet
- Handbook of Clinical Anaesthesia, Fourth EditionDocument2 pagesHandbook of Clinical Anaesthesia, Fourth EditionHany ElbarougyNo ratings yet
- Intro To Child Psychology - Module 1Document8 pagesIntro To Child Psychology - Module 1Jessielle100% (1)
- By Dr. AlabastroDocument9 pagesBy Dr. Alabastro2013SecBNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- Theory of Cultural Care and DiversityDocument16 pagesTheory of Cultural Care and DiversityJunne Rafaela NovalNo ratings yet
- Role of The Social Worker in The Outbreak of Pandemics A Case of COVID 19Document8 pagesRole of The Social Worker in The Outbreak of Pandemics A Case of COVID 19Rahul KhannaNo ratings yet
- Atellica NEPH 630 Brochure FINAL 152098222Document4 pagesAtellica NEPH 630 Brochure FINAL 152098222Ahmed MostafaNo ratings yet
- Step 2 Clinical Knowledge (CK) : Sample Test QuestionsDocument55 pagesStep 2 Clinical Knowledge (CK) : Sample Test QuestionsDr.Mohammed N. AbedNo ratings yet