Download as pdf or txt
You might also like
- WORKBOOK Traveller BeginnerDocument101 pagesWORKBOOK Traveller BeginnerRita Martínez Romero100% (3)
- W20 - Pentex Employee Indoctrination Handbook PDFDocument97 pagesW20 - Pentex Employee Indoctrination Handbook PDFjr_666100% (2)
- (BC) Kopytoff - The Cultural Biography of Things Commoditization As ProcessDocument29 pages(BC) Kopytoff - The Cultural Biography of Things Commoditization As ProcessKostasBaliotisNo ratings yet
- Shampoo in BedDocument19 pagesShampoo in BedNorman Batalla Juruena, DHCM, PhD, RN93% (14)
- Trauma Informed PracticesDocument24 pagesTrauma Informed PracticesLucero100% (3)
- 2 Environmental EpidemiologyDocument33 pages2 Environmental EpidemiologyRatna Ismail80% (5)
- Comparison and Summary of Types of ArthritisDocument2 pagesComparison and Summary of Types of ArthritisShaz Chindhy50% (2)
- SynthroidDocument3 pagesSynthroidKatie McPeekNo ratings yet
- Advancedvisualargument 2Document1 pageAdvancedvisualargument 2api-340854474No ratings yet
- District Training in Editorial Writing Balastigue, BelindaDocument69 pagesDistrict Training in Editorial Writing Balastigue, BelindaBeverly Jabonillo CabaleNo ratings yet
- KunalDocument36 pagesKunalSubhash KumarNo ratings yet
- 1.4 - Diffusion and Osmosis - CrosswordPuzzleDocument1 page1.4 - Diffusion and Osmosis - CrosswordPuzzlemmssthNo ratings yet
- Logical Form and Language: Gerhard PreyerDocument18 pagesLogical Form and Language: Gerhard PreyerBETSIE BAHRUNo ratings yet
- Group3 - The Internal Operational Environment of BusinessDocument19 pagesGroup3 - The Internal Operational Environment of BusinessJoie Lynn LiberatoNo ratings yet
- Reinventing GovernmentDocument296 pagesReinventing GovernmentPaul PurbaNo ratings yet
- Lumped ElementDocument4 pagesLumped ElementDharani ShahNo ratings yet
- Insight SoundDocument19 pagesInsight SoundMichael ToddNo ratings yet
- Dokumen - Tips - Chapter 8 PVRDocument34 pagesDokumen - Tips - Chapter 8 PVRjonathan.rzwNo ratings yet
- History: Pharmaceutical Engineering Is A Branch ofDocument7 pagesHistory: Pharmaceutical Engineering Is A Branch ofJonahNo ratings yet
- DT Window Shopping 02Document3 pagesDT Window Shopping 02Rabeel AfzalNo ratings yet
- Presentation 3Document1 pagePresentation 3api-3698735No ratings yet
- Measures Temperature Temperature Gradient Mercury-In-Glass ThermometerDocument4 pagesMeasures Temperature Temperature Gradient Mercury-In-Glass ThermometerNomunbileg KhNo ratings yet
- Crossword 1MWHpHImzDocument1 pageCrossword 1MWHpHImzHildiana Jontan JonesNo ratings yet
- Red Zone Report 2018Document211 pagesRed Zone Report 2018YunquanNo ratings yet
- Kami Export - 1688 - 001 PDFDocument4 pagesKami Export - 1688 - 001 PDFAlexander RussellNo ratings yet
- Absorption Costing or Full CostingDocument4 pagesAbsorption Costing or Full CostingMeghan Kaye LiwenNo ratings yet
- Clever Investor REI 101 GlossaryDocument24 pagesClever Investor REI 101 GlossaryMiguelNo ratings yet
- Hote LS& Trav ELS: Your Trans Actio N Has Been Suce Ssfull y Comp Leted !Document1 pageHote LS& Trav ELS: Your Trans Actio N Has Been Suce Ssfull y Comp Leted !Omar FarouqNo ratings yet
- Comment: Map Clusters of Diseases To Tackle MultimorbidityDocument3 pagesComment: Map Clusters of Diseases To Tackle MultimorbidityThiago SartiNo ratings yet
- Duragesic (Fentanyl Citrate)Document4 pagesDuragesic (Fentanyl Citrate)E100% (1)
- TEst EnglezaDocument9 pagesTEst Englezajeo mamaNo ratings yet
- Principles of MKT HandoutDocument336 pagesPrinciples of MKT HandoutNguyên Văn NhậtNo ratings yet
- Nanotechnology: For The Materials Science Journal, See - For Other Uses of "Nanotech", SeeDocument5 pagesNanotechnology: For The Materials Science Journal, See - For Other Uses of "Nanotech", SeeJonahNo ratings yet
- Week4 Heredity Inheritance-And-Variation MutationsDocument25 pagesWeek4 Heredity Inheritance-And-Variation Mutationsperlasirisalthea22No ratings yet
- Bryan Fuentes - Chapter 8 Neuron Practice - PacketDocument4 pagesBryan Fuentes - Chapter 8 Neuron Practice - PacketBryan FuentesNo ratings yet
- PDF Link It Level3 Teachers Pack CompressDocument137 pagesPDF Link It Level3 Teachers Pack CompressRodrigo Isaac Prado RamírezNo ratings yet
- Manipal Question PapersDocument23 pagesManipal Question PapersAman GuptaNo ratings yet
- 2022fall Arc1015 LowingDocument11 pages2022fall Arc1015 Lowingapi-726085240No ratings yet
- Classroom OrientationDocument32 pagesClassroom OrientationTin Cabrera-LansanganNo ratings yet
- Crossword HrC9kJmwzQDocument1 pageCrossword HrC9kJmwzQMarian SacopNo ratings yet
- Principles of MKT HandoutDocument336 pagesPrinciples of MKT Handoutlienlien31012004No ratings yet
- L10 Kolhberg'sDocument21 pagesL10 Kolhberg'shrmt LabNo ratings yet
- Data Structure Presenation2Document10 pagesData Structure Presenation2Andleeb juttiNo ratings yet
- The Quest For An All-Inclusive Human GenomeDocument4 pagesThe Quest For An All-Inclusive Human GenomeAnahí TessaNo ratings yet
- Deep FermDocument5 pagesDeep FermJonahNo ratings yet
- EgyptpuzzleDocument1 pageEgyptpuzzleemail2n213No ratings yet
- Lexi C OgraphyDocument6 pagesLexi C OgraphyJoe EdwardsNo ratings yet
- Settlement Crossword MemoDocument2 pagesSettlement Crossword MemoBarry Van SelmNo ratings yet
- Crossword Fast FashionDocument1 pageCrossword Fast FashionTechnologic Girl100% (1)
- Crossword fQV6YBvesSDocument1 pageCrossword fQV6YBvesSHoàng Anh ThưNo ratings yet
- WT SanitarywareDocument84 pagesWT SanitarywarePOOJA YOGENDRANo ratings yet
- 06 - Chapter 1Document55 pages06 - Chapter 1RaghaNo ratings yet
- 10 - ING - Cartilla Ingles Decimo Tercer Periodo InglesDocument13 pages10 - ING - Cartilla Ingles Decimo Tercer Periodo InglesvivianegubuNo ratings yet
- TabletsDocument28 pagesTabletsMuhammad sheraz67% (3)
- Report Text Non-Living ThingsDocument9 pagesReport Text Non-Living Thingshakimmirza318No ratings yet
- The Orthodontic-Oral Surgery Interface.Document6 pagesThe Orthodontic-Oral Surgery Interface.jing.zhao222No ratings yet
- Q Q M Indz: BossesliseDocument13 pagesQ Q M Indz: BosseslisePranav MishraNo ratings yet
- Engineering The Microbiome: OutlookDocument3 pagesEngineering The Microbiome: OutlookLindo PulgosoNo ratings yet
- The Structure of A Cultural Crisis Thinking About Cloth in FrancDocument24 pagesThe Structure of A Cultural Crisis Thinking About Cloth in FrancMelissa García MerazNo ratings yet
- French RevolutionDocument66 pagesFrench Revolutionaakash5c02No ratings yet
- T TP 1684849982 Pirate Alphabet Mazes Differentiated Letter Mazes - Ver - 1Document4 pagesT TP 1684849982 Pirate Alphabet Mazes Differentiated Letter Mazes - Ver - 1English RoomNo ratings yet
- Corrigenda: Corrigendum: Pramel7 Mediates Ground-State Pluripotency Through Proteasomal-Epigenetic Combined PathwaysDocument1 pageCorrigenda: Corrigendum: Pramel7 Mediates Ground-State Pluripotency Through Proteasomal-Epigenetic Combined PathwaysnugrahoneyNo ratings yet
- TangierDocument15 pagesTangierYosnier ViñalsNo ratings yet
- Specialconsiderationobturatorhernia 110210102125 Phpapp02Document17 pagesSpecialconsiderationobturatorhernia 110210102125 Phpapp02Ricky Aris FandikaNo ratings yet
- Radiationproctitis 090421073253 Phpapp02Document18 pagesRadiationproctitis 090421073253 Phpapp02Ricky Aris FandikaNo ratings yet
- 2015 Primary Breast Sarcoma A Retrospective Study Over 35 Years From A Single InstitutionDocument8 pages2015 Primary Breast Sarcoma A Retrospective Study Over 35 Years From A Single InstitutionRicky Aris FandikaNo ratings yet
- Primary Breast Sarcoma: A Rare Pathology in Women From The National Cancer Institute (Incan) of MexicoDocument3 pagesPrimary Breast Sarcoma: A Rare Pathology in Women From The National Cancer Institute (Incan) of MexicoRicky Aris FandikaNo ratings yet
- Neoadjuvant Chemotherapy For Primary Sarcoma of The Breast: A Case ReportDocument6 pagesNeoadjuvant Chemotherapy For Primary Sarcoma of The Breast: A Case ReportRicky Aris FandikaNo ratings yet
- Primary Breast Sarcoma: Clinicopathologic Series From The Mayo Clinic and Review of The LiteratureDocument5 pagesPrimary Breast Sarcoma: Clinicopathologic Series From The Mayo Clinic and Review of The LiteratureRicky Aris FandikaNo ratings yet
- A Scary Onset of A Rare and Aggressive Type of Primary Breast Sarcoma: A Case ReportDocument6 pagesA Scary Onset of A Rare and Aggressive Type of Primary Breast Sarcoma: A Case ReportRicky Aris FandikaNo ratings yet
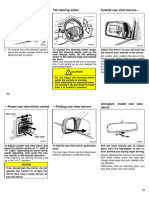
- Tilt Steering Wheel Outside Rear View MirrorsDocument3 pagesTilt Steering Wheel Outside Rear View MirrorsRicky Aris FandikaNo ratings yet
- 2008 Evaluation and Management of Persistent Problems After Surgery For Hirschsprung Disease in A ChildDocument7 pages2008 Evaluation and Management of Persistent Problems After Surgery For Hirschsprung Disease in A ChildRicky Aris FandikaNo ratings yet
- Harris Hip ScoreDocument2 pagesHarris Hip ScoreRicky Aris Fandika50% (2)
- Asm 8056Document2 pagesAsm 8056Taranpreet KaurNo ratings yet
- CHAPTER 16 Nursing Informatics and Healthcare PolicyDocument9 pagesCHAPTER 16 Nursing Informatics and Healthcare PolicyAllyssa Leila Estrebillo OrbeNo ratings yet
- QCGH Appendicitis ReportDocument48 pagesQCGH Appendicitis ReportIsabel ArcangelNo ratings yet
- File One: Chronology of 2002/03 UCLA investigation of employees and the Heimlich Institute's "malariotherapy" experiments in China (documents obtained via public records request to UCLA); direct download at: http://db.tt/viY1LyWeDocument126 pagesFile One: Chronology of 2002/03 UCLA investigation of employees and the Heimlich Institute's "malariotherapy" experiments in China (documents obtained via public records request to UCLA); direct download at: http://db.tt/viY1LyWepmheimlichNo ratings yet
- Science Reviewer 3rd QuarterDocument7 pagesScience Reviewer 3rd QuarterLyrMa NCNo ratings yet
- Key - Unit 5Document4 pagesKey - Unit 5Thuỷ TiênNo ratings yet
- Terminator - Safety Data SheetDocument8 pagesTerminator - Safety Data Sheetr afriantoNo ratings yet
- MystudyDocument5 pagesMystudyErica MarianeNo ratings yet
- Surveillance: Acute Flaccid Paralysis (AFP) SurveillanceDocument6 pagesSurveillance: Acute Flaccid Paralysis (AFP) SurveillancePratik MistryNo ratings yet
- FIT - TeachersDocument23 pagesFIT - TeachersdawnNo ratings yet
- HSPScale Research and Utility Smith Et AlDocument22 pagesHSPScale Research and Utility Smith Et AlpernotlisNo ratings yet
- Dpo2024 0014 CHD DirectorsDocument3 pagesDpo2024 0014 CHD DirectorsArmand BudlaoNo ratings yet
- Disusun Untuk Memenuhi Sebagian Syarat Kepaniteraan Klinik Dibagian Ilmu Penyakit Anak RSUD MuntilanDocument3 pagesDisusun Untuk Memenuhi Sebagian Syarat Kepaniteraan Klinik Dibagian Ilmu Penyakit Anak RSUD MuntilanAdistha TofanoNo ratings yet
- A Study On Socio-Economic Status of The Tea Garden Women Workers With Special Reference To Bokakhat Sub-Division of Golaghat District of AssamDocument4 pagesA Study On Socio-Economic Status of The Tea Garden Women Workers With Special Reference To Bokakhat Sub-Division of Golaghat District of AssamIt's ashu 434No ratings yet
- GMC Patient - Questionnaire PDF - 48210488Document2 pagesGMC Patient - Questionnaire PDF - 48210488adybutucNo ratings yet
- OHAS Ochs FinaDocument32 pagesOHAS Ochs FinaNot Racist By The WayNo ratings yet
- Test Bank For Nursing A Concept Based Approach To Learning Volume II 3rd Edition 3rd EditionDocument93 pagesTest Bank For Nursing A Concept Based Approach To Learning Volume II 3rd Edition 3rd EditionLarry Cessor100% (34)
- Peripheral NeuropathyDocument16 pagesPeripheral NeuropathyKhaled OssamaNo ratings yet
- Rashmi Agarwal, Amit Mhapuskar, Manjula Hebbale, Meenal Tepan, AyusheeDocument5 pagesRashmi Agarwal, Amit Mhapuskar, Manjula Hebbale, Meenal Tepan, AyusheemutiaNo ratings yet
- Understanding PDFDocument4 pagesUnderstanding PDFchyntiaNo ratings yet
- Set 2Document28 pagesSet 2Alyssa MontimorNo ratings yet
- Doctor's Excuse Note For Work TemplateDocument2 pagesDoctor's Excuse Note For Work Templatesilamo2267No ratings yet
- Factory Efficiency Comes To The Hospital - The New York TimesDocument7 pagesFactory Efficiency Comes To The Hospital - The New York Timesprasanna020391No ratings yet
- Corrective Action and Preventive Action Plan: RFO/CODocument3 pagesCorrective Action and Preventive Action Plan: RFO/COAlfred John TrinidadNo ratings yet
- Terapi CompressionDocument10 pagesTerapi CompressionErlinda KarimNo ratings yet
- Vap AssignmentDocument36 pagesVap AssignmentmochkurniawanNo ratings yet