Download as pdf or txt
You might also like
- Índice Guild of American Lutherie BooksDocument283 pagesÍndice Guild of American Lutherie BooksDaniel AndradeNo ratings yet
- 2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingDocument9 pages2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingHafeez AliNo ratings yet
- Megalourethra - Clinical Review and ManagementDocument4 pagesMegalourethra - Clinical Review and ManagementNugroho HarsonoNo ratings yet
- CPC IndicationsDocument5 pagesCPC IndicationsCarlos Daniel Giménez MéndezNo ratings yet
- Endoscopic Choroid Plexus Coagulation in InfantsDocument7 pagesEndoscopic Choroid Plexus Coagulation in InfantsCarlos Daniel Giménez MéndezNo ratings yet
- Selective Feticide in Complicated Monochorionic Twin Pregnancies Using Ultrasound-Guided Bipolar Cord CoagulationDocument5 pagesSelective Feticide in Complicated Monochorionic Twin Pregnancies Using Ultrasound-Guided Bipolar Cord CoagulationDesyHandayaniNo ratings yet
- Anillos ClasificacionDocument6 pagesAnillos ClasificacionCorazon MabelNo ratings yet
- Jurnal tht7Document5 pagesJurnal tht7Tri RominiNo ratings yet
- Infected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantDocument4 pagesInfected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantIJAR JOURNALNo ratings yet
- TemplateDocument7 pagesTemplateNaeem BukhariNo ratings yet
- (10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesDocument9 pages(10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesasiyazaidiaNo ratings yet
- Huge Extradural Multilevel Lumbar Abscess. Case ReportDocument11 pagesHuge Extradural Multilevel Lumbar Abscess. Case ReportNervul VagNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Riri KumalaNo ratings yet
- MainDocument5 pagesMainajengiracilyNo ratings yet
- 1 s2.0 S0022346819307535 MainDocument5 pages1 s2.0 S0022346819307535 MainMeta ParamitaNo ratings yet
- Editorial Endoscopic Fourth Ventricular Aqueductoplasty: H L. R, M.DDocument2 pagesEditorial Endoscopic Fourth Ventricular Aqueductoplasty: H L. R, M.DIsmail MuhammadNo ratings yet
- CSF Dynamics in Dandy-Walker SyndromeDocument5 pagesCSF Dynamics in Dandy-Walker SyndromeSergio SaraivaNo ratings yet
- Hirose 2003Document5 pagesHirose 2003lakshay raoNo ratings yet
- Thoracoscopic Repair For Congenital Diaphragmatic Hernia: Experience With 139 CasesDocument5 pagesThoracoscopic Repair For Congenital Diaphragmatic Hernia: Experience With 139 CasesBaiduri YasintianiNo ratings yet
- A Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalDocument4 pagesA Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalHaziq AnuarNo ratings yet
- Abdomen: International Abstracts of Pediatric Surgery 593Document1 pageAbdomen: International Abstracts of Pediatric Surgery 593Yohanes WilliamNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleHazbullah AisyNo ratings yet
- PolMerkurLek2023i1 (Dragged)Document4 pagesPolMerkurLek2023i1 (Dragged)MogiMediawanNo ratings yet
- Acquired Nasopharyngeal StenosisDocument8 pagesAcquired Nasopharyngeal StenosisLuiz Cesar WidolinNo ratings yet
- Stricture Urethra in Children: An Indian Perspective: Original ArticleDocument6 pagesStricture Urethra in Children: An Indian Perspective: Original ArticleLilis Endah SulistiyawatiNo ratings yet
- Congenital Obstructive Hydrocephalus Revised 1 AutorecoveredDocument7 pagesCongenital Obstructive Hydrocephalus Revised 1 Autorecoveredapi-652813198No ratings yet
- Slide, Tracheal BronchusDocument4 pagesSlide, Tracheal Bronchusemmanuel le bretNo ratings yet
- Musculocutaneous Latissimus Dorsi Free Transfer Flap For Total Phalloplasty in ChildrenDocument7 pagesMusculocutaneous Latissimus Dorsi Free Transfer Flap For Total Phalloplasty in ChildrenJad DegheiliNo ratings yet
- (10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsDocument7 pages(10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsPutri PrameswariNo ratings yet
- Intrinsic Third Ventricular Craniopharyngiomas: Report On Six Cases and A Review of The LiteratureDocument8 pagesIntrinsic Third Ventricular Craniopharyngiomas: Report On Six Cases and A Review of The LiteratureAmina GoharyNo ratings yet
- WIITM Art 39955-10Document8 pagesWIITM Art 39955-10Sabri AbyNo ratings yet
- Anorectal MalformationsDocument7 pagesAnorectal MalformationsTomi JuliandiNo ratings yet
- Electrocautery Versus Curette Adenoidectomy: Comparison of Postoperative ResultsDocument8 pagesElectrocautery Versus Curette Adenoidectomy: Comparison of Postoperative Resultsthanhb1lqdNo ratings yet
- Warf 2011Document7 pagesWarf 2011Anonymous x4Ba2BNo ratings yet
- Jurnal Bedah AnakDocument3 pagesJurnal Bedah AnakAstari ArumNo ratings yet
- J Neurosurg Pediatr Article p52Document10 pagesJ Neurosurg Pediatr Article p52Audhrey BNo ratings yet
- Difficult Intubation and Anesthetic Management in An Adult Patient With Undiagnosed Congenital Tracheal Stenosis: A Case ReportDocument6 pagesDifficult Intubation and Anesthetic Management in An Adult Patient With Undiagnosed Congenital Tracheal Stenosis: A Case ReportBianca CaterinalisendraNo ratings yet
- Remote Access Endoscopic Parathyroidectomy: A Study of 17 Cases From Central IndiaDocument6 pagesRemote Access Endoscopic Parathyroidectomy: A Study of 17 Cases From Central IndiaKriti KumariNo ratings yet
- Exemplu 4Document4 pagesExemplu 4Pavel SebastianNo ratings yet
- Timetable PosterExDocument45 pagesTimetable PosterExNeo Rodriguez AlvaradoNo ratings yet
- Avaliação Ultra-Sonográfica Das Técnicas de Punção Da Veia Jugular Interna em CriançasDocument4 pagesAvaliação Ultra-Sonográfica Das Técnicas de Punção Da Veia Jugular Interna em CriançasJing CruzNo ratings yet
- Anoplastia Percutanea 2022Document11 pagesAnoplastia Percutanea 2022Sandra Cárdenas HilasacaNo ratings yet
- Management of T.B.M. Hydrocephalus Role of Shunt Surgery - 55 58Document4 pagesManagement of T.B.M. Hydrocephalus Role of Shunt Surgery - 55 58Kushal BhatiaNo ratings yet
- Dandy Walker SyndromeDocument3 pagesDandy Walker SyndromeIqra AnugerahNo ratings yet
- Nidal Embolization of Brain Arteriovenous Malformations Using Onyx in 94 PatientsDocument6 pagesNidal Embolization of Brain Arteriovenous Malformations Using Onyx in 94 PatientsRifqi AnraNo ratings yet
- Undescended TestisDocument3 pagesUndescended TestisIoannis ValioulisNo ratings yet
- Hydro ManagementDocument7 pagesHydro ManagementHadaAtiyehNo ratings yet
- Cornell A 2003Document13 pagesCornell A 2003dnazaryNo ratings yet
- Wrap Plication of Megaureter Around Normal-Sized Ureter For Complete Duplex System ReimplantationsDocument5 pagesWrap Plication of Megaureter Around Normal-Sized Ureter For Complete Duplex System ReimplantationsDirga Rasyidin LNo ratings yet
- Ijms 40 58Document5 pagesIjms 40 58aprilia siregarNo ratings yet
- HidrosefalusDocument10 pagesHidrosefalusNelly AstikaNo ratings yet
- Jurnal THTDocument5 pagesJurnal THTTri RominiNo ratings yet
- Anesthesia For Cesarean Section in A Patient With AchondroplasiaDocument17 pagesAnesthesia For Cesarean Section in A Patient With AchondroplasiaFathin Amirah AminnuddinNo ratings yet
- Surgical Techniques: Plication of The DiaphragmDocument14 pagesSurgical Techniques: Plication of The DiaphragmFranciscoJ.ReynaSepúlvedaNo ratings yet
- (19330715 - Journal of Neurosurgery - Pediatrics) Intraventricular Bone Dust Migration After Neuroendoscopy - Report of 2 CasesDocument6 pages(19330715 - Journal of Neurosurgery - Pediatrics) Intraventricular Bone Dust Migration After Neuroendoscopy - Report of 2 CasesBruno MañonNo ratings yet
- HydronephrosisDocument3 pagesHydronephrosisCarla AlmerolNo ratings yet
- (19330693 - Journal of Neurosurgery) Neuroendoscopic Stent Placement For Cerebrospinal Fluid Pathway Obstructions in AdultsDocument9 pages(19330693 - Journal of Neurosurgery) Neuroendoscopic Stent Placement For Cerebrospinal Fluid Pathway Obstructions in AdultsVlad VPNo ratings yet
- Vaginal Extrusion of A Ventriculoperitoneal Shunt A Case Report and Review ofDocument10 pagesVaginal Extrusion of A Ventriculoperitoneal Shunt A Case Report and Review ofDian AdiNo ratings yet
- Anaesthetic Implications in A Patient With Morquio A SyndromeDocument4 pagesAnaesthetic Implications in A Patient With Morquio A SyndromepamelaNo ratings yet
- Criog2014 108973Document4 pagesCriog2014 108973Denia Haritsa AprilianiNo ratings yet
- Medi 95 E2797Document3 pagesMedi 95 E2797Rui Pedro PereiraNo ratings yet
- Blume 2004Document8 pagesBlume 2004jela1309No ratings yet
- Goll Witz Er 2018Document7 pagesGoll Witz Er 2018jela1309No ratings yet
- Hypoglossal Nerve Stimulation 1666116571Document8 pagesHypoglossal Nerve Stimulation 1666116571jela1309No ratings yet
- IOM Carotid Endarterectomy PescadorDocument8 pagesIOM Carotid Endarterectomy Pescadorjela1309No ratings yet
- Stokes Second Problem by Laplace TransformDocument19 pagesStokes Second Problem by Laplace TransformSidra AfzalNo ratings yet
- AVO Analysis Guide PDFDocument89 pagesAVO Analysis Guide PDFceciliaNo ratings yet
- Vatican Railway SystemDocument54 pagesVatican Railway SystemAlexander Gordon InesNo ratings yet
- Lynyrd Skynyrd - Steve Gaines Equipment HistoryDocument10 pagesLynyrd Skynyrd - Steve Gaines Equipment HistorySean88% (8)
- Starbucks Business Report ManagementDocument21 pagesStarbucks Business Report ManagementParidhi LapalikarNo ratings yet
- Pragati Maidan Exhibition DetailsDocument10 pagesPragati Maidan Exhibition DetailsDr-Amit KumarNo ratings yet
- Electrical Troubleshooting ManualDocument52 pagesElectrical Troubleshooting ManualMohammed Shdiefat100% (1)
- SSS 2 TD CAT 2nd TermDocument3 pagesSSS 2 TD CAT 2nd TermFagbohunka EricNo ratings yet
- LR Energy Guidance Notes For The Calculation of Probabilistic Explosion Loads PDFDocument18 pagesLR Energy Guidance Notes For The Calculation of Probabilistic Explosion Loads PDFJay JayNo ratings yet
- DR - B - R - Kerur, Dept - of Physics, GUGDocument8 pagesDR - B - R - Kerur, Dept - of Physics, GUGkerurbrk2009No ratings yet
- Solubility and EquilibriaDocument35 pagesSolubility and EquilibriaYosephine Intan AyuningtyasNo ratings yet
- American Lincoln MPV 60 Ecp Parts List FordDocument153 pagesAmerican Lincoln MPV 60 Ecp Parts List FordYew LimNo ratings yet
- AKG-2 Gate 4 Review Package Rev 0Document19 pagesAKG-2 Gate 4 Review Package Rev 0pvpallasigui3126100% (1)
- HW2 CIVE210 Equilibrium-Particles SOLUTIONDocument12 pagesHW2 CIVE210 Equilibrium-Particles SOLUTIONNNo ratings yet
- 74LS245Document2 pages74LS245api-3711187No ratings yet
- MARCH 7-9, 2011: Biomolecular Drug TargetsDocument2 pagesMARCH 7-9, 2011: Biomolecular Drug TargetsSwapanil YadavNo ratings yet
- DLL - Science 6 - Q2 - W2Document5 pagesDLL - Science 6 - Q2 - W2Geoffrey Tolentino-Unida100% (1)
- Control Electrical Appliances Using PCDocument46 pagesControl Electrical Appliances Using PCsumit gandhi100% (1)
- TM 9 2320 304 14 and PDocument1,321 pagesTM 9 2320 304 14 and PjordanloNo ratings yet
- J.saintifika Uji Bioavailabilitas Dan BioekivalensiDocument8 pagesJ.saintifika Uji Bioavailabilitas Dan BioekivalensiAhmad MujahidinNo ratings yet
- TurbineDocument8 pagesTurbineJay Patel100% (1)
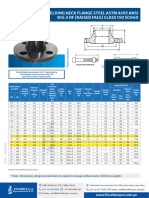
- Bridas WN Clase 150Document1 pageBridas WN Clase 150juan ormacheaNo ratings yet
- Chemistry Exam Q ADocument14 pagesChemistry Exam Q AmateialesandraNo ratings yet
- Private Cloud Appliance x9 DatasheetDocument3 pagesPrivate Cloud Appliance x9 DatasheetKesava ReddyNo ratings yet
- WCR AscoDocument12 pagesWCR AscojuliosieteNo ratings yet
- SPD - List of AnnexuresDocument1 pageSPD - List of AnnexuresadheesNo ratings yet
- T50e Replace DriveDocument24 pagesT50e Replace DrivevcalderonvNo ratings yet
- Fertilizacion Nitrogenada en Maiz Basada en Materia Organica (Sanchez Roldan)Document33 pagesFertilizacion Nitrogenada en Maiz Basada en Materia Organica (Sanchez Roldan)Brian RamosNo ratings yet