Download as pdf or txt
You might also like
- En1568 PDFDocument9 pagesEn1568 PDFRahul BhattNo ratings yet
- Ingersoll Rand Compressor Eiger Part ListDocument70 pagesIngersoll Rand Compressor Eiger Part ListAlpesh Lakhani50% (2)
- Y U RanchDocument2 pagesY U RanchHibo RiazNo ratings yet
- Warehouse AnalyticsDocument62 pagesWarehouse AnalyticsMary Williams100% (1)
- Academic Fee - 2022-2023Document2 pagesAcademic Fee - 2022-2023thangarajbala123No ratings yet
- EWS Scholarship SchemeDocument3 pagesEWS Scholarship SchemeSam BasNo ratings yet
- Anshul KaushalDocument4 pagesAnshul KaushalAnshul KaushalNo ratings yet
- Course: BA (H) ECONOMICS Course: BA (H) ECONOMICSDocument1 pageCourse: BA (H) ECONOMICS Course: BA (H) ECONOMICSTushar ChadhaNo ratings yet
- Fees PolicyDocument17 pagesFees PolicyRidwan MohsinNo ratings yet
- PGVocational 1 ST Counselling 16092019Document1 pagePGVocational 1 ST Counselling 16092019Vishal BhardwajNo ratings yet
- Bba 2020-21Document60 pagesBba 2020-21zenexdegreematerialsNo ratings yet
- Schedule of TuitionDocument5 pagesSchedule of TuitionJoanne Pauline Tenedero - RuelaNo ratings yet
- Notification (Semestefr Ees)Document2 pagesNotification (Semestefr Ees)Cool JugglerNo ratings yet
- McKinsey PST Test PracticeDocument6 pagesMcKinsey PST Test PracticeShan Vahora100% (4)
- Muhammad Medical College, Mirpurkhas Fee Structure For Mbbs 2021-2022 Fixed Fees For Local StudentsDocument1 pageMuhammad Medical College, Mirpurkhas Fee Structure For Mbbs 2021-2022 Fixed Fees For Local StudentsAbdul QadeerNo ratings yet
- MBBS Fee Structure 1 CompressedDocument1 pageMBBS Fee Structure 1 CompressedMuhammad Zaryab KhanNo ratings yet
- Notification Dated 07.04.22 Regarding Conduct of Examination For Even Semester May June 2022Document2 pagesNotification Dated 07.04.22 Regarding Conduct of Examination For Even Semester May June 2022avisinghoo7No ratings yet
- Lesson 10 ReportDocument26 pagesLesson 10 ReportSessylu TalaveraNo ratings yet
- Circular: Savitribai Phule Pune UniversityDocument2 pagesCircular: Savitribai Phule Pune UniversityShivamNo ratings yet
- Placement & Higher StudiesDocument8 pagesPlacement & Higher StudiesSukhoi 33No ratings yet
- PAF IAST BAC Fee Policyv2June23.12Document2 pagesPAF IAST BAC Fee Policyv2June23.12shb4507No ratings yet
- Study Permit 2Document2 pagesStudy Permit 2Ghebre PalloNo ratings yet
- Fee Structure 24 25Document1 pageFee Structure 24 25Monika SinghalNo ratings yet
- GO Fee 2019-20Document11 pagesGO Fee 2019-20Srinivas goudNo ratings yet
- T&P Regulations - 2023 Batch - FinalDocument7 pagesT&P Regulations - 2023 Batch - Final124 SHAIL SINGHNo ratings yet
- Kibabii University College: Students Fees PolicyDocument11 pagesKibabii University College: Students Fees PolicyBRIAN WANYONYINo ratings yet
- FEE ISA Brochure 2023Document1 pageFEE ISA Brochure 2023jayasuryasurya2507No ratings yet
- Schedule of Fees For The Academic Year 2020-21 First Degree (FD)Document4 pagesSchedule of Fees For The Academic Year 2020-21 First Degree (FD)Pranshu SaraswatNo ratings yet
- Catc Lists 2020Document1,022 pagesCatc Lists 2020Halal BoiNo ratings yet
- Master's Program Tuition Spring 2024 - International - FinanceDocument15 pagesMaster's Program Tuition Spring 2024 - International - FinancebamoakoNo ratings yet
- University Link - Catarman Site: University of Eastern PhilippinesDocument3 pagesUniversity Link - Catarman Site: University of Eastern PhilippinesMark Johnson San JuanNo ratings yet
- SHS Student Discipline HandbookDocument39 pagesSHS Student Discipline HandbookJakeNo ratings yet
- Ecole Polytechnique Bachelor Program Handbook and Code of Conduct 2022Document43 pagesEcole Polytechnique Bachelor Program Handbook and Code of Conduct 2022emmanuelaudige7No ratings yet
- SSS H&T CheckList 2012Document26 pagesSSS H&T CheckList 2012vaishalipol24No ratings yet
- Scms Group: Admission BrochureDocument24 pagesScms Group: Admission BrochureSooraj DilipNo ratings yet
- University of Calcutta: A/S 40 013 Dated: 12 02 2020Document15 pagesUniversity of Calcutta: A/S 40 013 Dated: 12 02 2020sangbarto basuNo ratings yet
- Case Study 2: Beemis Technical CollegeDocument5 pagesCase Study 2: Beemis Technical Collegeanon-811984No ratings yet
- SPOT Admission 2023-24Document3 pagesSPOT Admission 2023-24Fake AccNo ratings yet
- University of Westminster Refund and Compensation PolicyDocument7 pagesUniversity of Westminster Refund and Compensation PolicyDr. Farzina RahmanNo ratings yet
- Affiliation CriteriaDocument11 pagesAffiliation CriteriaMuhammad AzeemNo ratings yet
- Lab 2Document2 pagesLab 2shifaNo ratings yet
- UPFU Vs UPDocument1 pageUPFU Vs UPMaribel Nicole LopezNo ratings yet
- Fee ScheduleDocument1 pageFee ScheduleDeepak SwamiNo ratings yet
- HEC Institutional Affiliation Constituent Colleges Policy - 2023Document19 pagesHEC Institutional Affiliation Constituent Colleges Policy - 2023Jawad NaqviNo ratings yet
- Balik-Eskwela Project Action PlanDocument4 pagesBalik-Eskwela Project Action PlanLaiel CapistranoNo ratings yet
- Orge University. AnjieDocument4 pagesOrge University. AnjieKim Kyun SiNo ratings yet
- 63723515f03ec595261401 WSADFeeDocument1 page63723515f03ec595261401 WSADFeekhatija kubraNo ratings yet
- Fee Structure For Pre-Foundation Career Care Programmes: Academic Session 2017-2018 - Regular Classroom ProgrammeDocument2 pagesFee Structure For Pre-Foundation Career Care Programmes: Academic Session 2017-2018 - Regular Classroom ProgrammeMd Rizwan AhmadNo ratings yet
- Electrical Licensing2013Document2 pagesElectrical Licensing2013David SilverNo ratings yet
- Recombinant DNA Technology: October 2017Document2 pagesRecombinant DNA Technology: October 2017Indah Indryani UNo ratings yet
- Guidelines For Payments of NRF Postgraduate Scholarships 2022 FinalDocument3 pagesGuidelines For Payments of NRF Postgraduate Scholarships 2022 Finallungiswambewu700No ratings yet
- Electrical Licensing2013 2Document2 pagesElectrical Licensing2013 2Samuel HamiltonNo ratings yet
- Certificate of Registration: Tarlac State UniversityDocument1 pageCertificate of Registration: Tarlac State UniversityMark Jhosua Austria GalinatoNo ratings yet
- Virtual Universigty Prospectus 2017 18Document114 pagesVirtual Universigty Prospectus 2017 18Gulzar Ahmad Rawn0% (1)
- Pranveer Singh Institute of Technology: B.Tech B.Pharm Mba Mca M.Tech M.Pharm D.PharmDocument12 pagesPranveer Singh Institute of Technology: B.Tech B.Pharm Mba Mca M.Tech M.Pharm D.PharmAayush MishraNo ratings yet
- Course Crediting Form: Personal Information Academic InformationDocument1 pageCourse Crediting Form: Personal Information Academic InformationNico Vladmir KaiserNo ratings yet
- Sy Admission Circular For A.Y. 2023-2024Document2 pagesSy Admission Circular For A.Y. 2023-2024Akash RanaNo ratings yet
- Family Tuition Benefit PolicyDocument13 pagesFamily Tuition Benefit PolicySunandha SrinivasanNo ratings yet
- Family Tuition Benefit ProcedureDocument2 pagesFamily Tuition Benefit ProcedureSunandha SrinivasanNo ratings yet
- IoT Backend With RedisDocument9 pagesIoT Backend With RedisSunandha SrinivasanNo ratings yet
- PLSQL ContextSwitchingDocument8 pagesPLSQL ContextSwitchingSunandha SrinivasanNo ratings yet
- Def Abstracts Presentations Meet The Oracle MastersDocument4 pagesDef Abstracts Presentations Meet The Oracle MastersSunandha SrinivasanNo ratings yet
- 43 CA CPT Dec 2010 Question Paper With Answer Key 2Document6 pages43 CA CPT Dec 2010 Question Paper With Answer Key 2Vishal Gattani100% (1)
- Pedia TrikDocument45 pagesPedia TrikZulKifli NahumpangNo ratings yet
- Biodiversity Management PlanDocument55 pagesBiodiversity Management Planshamroz khanNo ratings yet
- Yahoo Data DownloadDocument5 pagesYahoo Data DownloadbianchaoNo ratings yet
- SPC SpreadsheetDocument10 pagesSPC SpreadsheetSpyros IliakisNo ratings yet
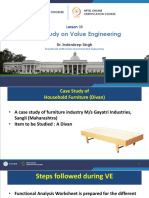
- Case Study On Value Engineering: Lesson 10Document16 pagesCase Study On Value Engineering: Lesson 10arunNo ratings yet
- Akira TVDocument22 pagesAkira TVErmand WindNo ratings yet
- 04 Dev275 s00Document10 pages04 Dev275 s00Vishnu PatidarNo ratings yet
- TC15M 65M Manual PDFDocument15 pagesTC15M 65M Manual PDFReciclando ChatarraNo ratings yet
- ENGINEERING DESIGN GUIDELINES Reboiler Rev1.3web PDFDocument12 pagesENGINEERING DESIGN GUIDELINES Reboiler Rev1.3web PDFSamit MitraNo ratings yet
- EPACII PCP Operational ManualDocument118 pagesEPACII PCP Operational ManualSergey ZaytsevNo ratings yet
- The Dual in LPDocument17 pagesThe Dual in LPShreeyesh MenonNo ratings yet
- CB-8466 ECF ClearFire Economizer PDFDocument16 pagesCB-8466 ECF ClearFire Economizer PDFAbdul RazzaqNo ratings yet
- Tally Exrercise 2: Date Description AmountDocument1 pageTally Exrercise 2: Date Description AmountExcel WaysNo ratings yet
- Commercial PoliciesDocument8 pagesCommercial Policiesapi-3706009No ratings yet
- Huawei Rru3801c Dnai 2012 TocDocument5 pagesHuawei Rru3801c Dnai 2012 TocEarl LumNo ratings yet
- Honda Atlas Cars (Pakistan) Limited 31 March 2022Document75 pagesHonda Atlas Cars (Pakistan) Limited 31 March 2022Ahmad Hanif AwanNo ratings yet
- GHMC taxGHMC TAXDocument12 pagesGHMC taxGHMC TAXpoornima_npNo ratings yet
- Capital Budgeting Techniques Capital Budgeting TechniquesDocument65 pagesCapital Budgeting Techniques Capital Budgeting Techniquesarslan shahNo ratings yet
- Submitted By-Rashmi Parmar (8601) Trisha Sinha Roy (8629) Sanchari Mohanta (8631) Raunak Shirali (8609) Karan Khot (8615) Swapnil Kulkarni (8625)Document38 pagesSubmitted By-Rashmi Parmar (8601) Trisha Sinha Roy (8629) Sanchari Mohanta (8631) Raunak Shirali (8609) Karan Khot (8615) Swapnil Kulkarni (8625)Vipul PartapNo ratings yet
- ORLANDI Catalogue Blue en-DEDocument44 pagesORLANDI Catalogue Blue en-DEtinashemambarizaNo ratings yet
- Variable Pitch Fan System - If EquippedDocument3 pagesVariable Pitch Fan System - If EquippedEVER DAVID SAAVEDRA HUAYHUANo ratings yet
- AneurysmDocument37 pagesAneurysmbilal safiNo ratings yet
- Revolusi Industri 4.0: Impak Terhadap Perkembangan Pendidikan Tinggi Di MalaysiaDocument13 pagesRevolusi Industri 4.0: Impak Terhadap Perkembangan Pendidikan Tinggi Di Malaysiaeiman medinaNo ratings yet
- Sample Letter of Intent To Transfer FundsDocument2 pagesSample Letter of Intent To Transfer Fundsnavid kamravaNo ratings yet
- DSA Weekly PlanDocument3 pagesDSA Weekly PlanJatin0% (1)