Download as pdf or txt
You might also like
- Great Writing 4 5th Edition Great Essays Answer KeyDocument10 pagesGreat Writing 4 5th Edition Great Essays Answer KeyAseel80% (10)
- Profile: DashboardDocument22 pagesProfile: DashboardGhenea Catalin-StefanNo ratings yet
- Caustic Soda e CHB 014Document1 pageCaustic Soda e CHB 014Wasif KarimNo ratings yet
- Assignment #4 Supported Student Self-Assessment (Antonia2)Document32 pagesAssignment #4 Supported Student Self-Assessment (Antonia2)SapMars 0No ratings yet
- Spookmaster Pumpkin Carving Patterns Book 2Document62 pagesSpookmaster Pumpkin Carving Patterns Book 2Mister MisterNo ratings yet
- Positive and Negative Syndrome Scale (Panss) Rating Criteria General Rating InstructionsDocument13 pagesPositive and Negative Syndrome Scale (Panss) Rating Criteria General Rating InstructionsBangkit Bayupamungkas100% (1)
- Parl List TKDocument4 pagesParl List TKJosé Chancafe Angeles100% (1)
- DND 3.5 Spell CardsDocument9 pagesDND 3.5 Spell CardsMister MisterNo ratings yet
- Treatment Plan: VCA Animal Specialty GroupDocument4 pagesTreatment Plan: VCA Animal Specialty Groupjingnwe houNo ratings yet
- Budget PRDocument1 pageBudget PRapi-527913909No ratings yet
- Corte 6 A 12-05-2024Document1 pageCorte 6 A 12-05-2024PetResort PetResortmxNo ratings yet
- Habersham Medical Center 1 1009Document126 pagesHabersham Medical Center 1 1009swarnaNo ratings yet
- Invoice 4328984Document1 pageInvoice 4328984John PeanutbutterNo ratings yet
- Bala RajuDocument9 pagesBala RajuSrichandEadaNo ratings yet
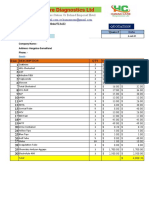
- Human Care Diagnostics LTD: Telephone: +520043/520044/513422 Quote #Document3 pagesHuman Care Diagnostics LTD: Telephone: +520043/520044/513422 Quote #Marwaan Updilaahi HazzanNo ratings yet
- 3 Sigma Spndcat 010109-111609Document3 pages3 Sigma Spndcat 010109-111609SteveackleyNo ratings yet
- Sale 1125 08-04-2024Document1 pageSale 1125 08-04-2024deepak123megNo ratings yet
- Covenant University Medical Centre: Fee-For-Service R EportDocument2 pagesCovenant University Medical Centre: Fee-For-Service R Eportakinlabi aderibigbeNo ratings yet
- Lista Veterinaria 20 de Marzo Del 2024Document6 pagesLista Veterinaria 20 de Marzo Del 2024Ramon RamirezNo ratings yet
- Bon OkDocument3 pagesBon OkDiffa RahmadinaNo ratings yet
- Wilcox Medical Center ChargemasterDocument601 pagesWilcox Medical Center ChargemasterMarthaNo ratings yet
- Isla's Expenses: Description Quantity Unit Price CostDocument2 pagesIsla's Expenses: Description Quantity Unit Price CostKaren SabiliNo ratings yet
- 2019 WDH CHRG Master Ave DRG WebsiteDocument306 pages2019 WDH CHRG Master Ave DRG Websitejona tumukundeNo ratings yet
- Money Spell (Recieve Money in Your Account) Money Flow +27788676511 and Be Successful For The Rest of Your Life in Limpopo, Mpumalanga, Polokwane, North West, Pretoria, Witbank, SowetoDocument306 pagesMoney Spell (Recieve Money in Your Account) Money Flow +27788676511 and Be Successful For The Rest of Your Life in Limpopo, Mpumalanga, Polokwane, North West, Pretoria, Witbank, Sowetojona tumukundeNo ratings yet
- Data Alkes Dan Reagent LabDocument4 pagesData Alkes Dan Reagent Labaden farid adiredjaNo ratings yet
- Budgeting Project 4Document7 pagesBudgeting Project 4api-527875218No ratings yet
- 0 - Paquetes Vinces PalenqueDocument4 pages0 - Paquetes Vinces PalenqueAngie LavalleNo ratings yet
- Matmed Ana PaulaDocument1 pageMatmed Ana PaulacainavmelloNo ratings yet
- TesdtalvaroDocument3 pagesTesdtalvaroJose AlvarezNo ratings yet
- Cin7 Quote 12025 HCAR2854-63 21 Nov 2022 312 PMDocument5 pagesCin7 Quote 12025 HCAR2854-63 21 Nov 2022 312 PMroddy narayanNo ratings yet
- Laporan Bulanan Mutasi Barang Persediaan (Habis Pakai Laborat)Document16 pagesLaporan Bulanan Mutasi Barang Persediaan (Habis Pakai Laborat)putraNo ratings yet
- Unit Cost Op PhacoDocument5 pagesUnit Cost Op PhacoYulis NawatiNo ratings yet
- December 19, 2022 (6am - 2PM)Document1 pageDecember 19, 2022 (6am - 2PM)Jasher Dave AcabalNo ratings yet
- Reactivos VB1Document3 pagesReactivos VB1Jorge BernésNo ratings yet
- Tucker SchultzDocument1 pageTucker SchultzAnonymous px3Lk9jNo ratings yet
- Black Friday - Maureen - Pribadi (Ada Longevity Punya Grup)Document1 pageBlack Friday - Maureen - Pribadi (Ada Longevity Punya Grup)maureeniciousNo ratings yet
- + Função CONT - NÚM 4 Senac Função Cont - Valores 9, Função Contar - Vazio 1Document4 pages+ Função CONT - NÚM 4 Senac Função Cont - Valores 9, Função Contar - Vazio 1Emily MartinsNo ratings yet
- Laporan Stock Opname Obat Dan BHP Nov 2022Document5 pagesLaporan Stock Opname Obat Dan BHP Nov 2022RSINU DEMAK OFFICIALNo ratings yet
- (Depo) SO JANUARI 2022Document70 pages(Depo) SO JANUARI 2022NANDANo ratings yet
- Women's Reproductive Health Free Clinic: Personnel ExpensesDocument2 pagesWomen's Reproductive Health Free Clinic: Personnel ExpensesHujale MaxamedNo ratings yet
- Costos de ProducciónDocument21 pagesCostos de ProducciónLondres RDNo ratings yet
- Dream MarketDocument3 pagesDream MarketPatrick PerezNo ratings yet
- Elektif NO Uraian QTY: PendaftaranDocument3 pagesElektif NO Uraian QTY: PendaftaranrismayantiNo ratings yet
- 1 Ha Tomato 5.21Document4 pages1 Ha Tomato 5.21Tadiwanashe JackNo ratings yet
- Vet 1Document6 pagesVet 1framkarugahNo ratings yet
- Price List 16 06 20Document3 pagesPrice List 16 06 20k3 rsuihaNo ratings yet
- Electrical Material (18%GST Extra) PDFDocument2 pagesElectrical Material (18%GST Extra) PDFswami samruddhiNo ratings yet
- GoodbillDocument1 pageGoodbillmiranda criggerNo ratings yet
- Smry PDFDocument1 pageSmry PDFABDIKANI SHEIKH MOHAMOUDNo ratings yet
- Refocusing BOK PuskesmasDocument22 pagesRefocusing BOK PuskesmasMusripinPanabaliNo ratings yet
- James Grabowski Paystub 2022-12-30 RedactedDocument2 pagesJames Grabowski Paystub 2022-12-30 RedactedDaniela CarrascoNo ratings yet
- Senergy Product ChartDocument17 pagesSenergy Product Chartvctrrls16No ratings yet
- Estimate 1425 17-11-2023Document1 pageEstimate 1425 17-11-2023bashar mohammedNo ratings yet
- Kelompok Akmen LanjutanDocument5 pagesKelompok Akmen LanjutanHilly HNNo ratings yet
- Australian Laboratory Services Pty LTD ABN 84 009 936 029 Excellence in Analytical ChemistryDocument2 pagesAustralian Laboratory Services Pty LTD ABN 84 009 936 029 Excellence in Analytical Chemistrycloudno911No ratings yet
- Product Name CAS Number Prices in USD : Product Name Specification S Iu/mg US$/eachDocument2 pagesProduct Name CAS Number Prices in USD : Product Name Specification S Iu/mg US$/eachZhangNo ratings yet
- Amount Lina Abg Fendi Abg Nor Total Bill For SKH $14,968.97Document2 pagesAmount Lina Abg Fendi Abg Nor Total Bill For SKH $14,968.97Natasha SalimanNo ratings yet
- + Função CONT - NÚM 4 Senac Função Cont - Valores 9, Função Contar - Vazio 1Document4 pages+ Função CONT - NÚM 4 Senac Função Cont - Valores 9, Função Contar - Vazio 1Emily MartinsNo ratings yet
- BaselineCostUpdate Updated Coscted Bituminous Baseline Cases 28Document2 pagesBaselineCostUpdate Updated Coscted Bituminous Baseline Cases 28Gustavo ArrietaNo ratings yet
- Excel Perencanaan Reagen 2024Document48 pagesExcel Perencanaan Reagen 2024Sri MaryatiNo ratings yet
- LISTA DE PRECIOS 7 de Noviembre 2023Document7 pagesLISTA DE PRECIOS 7 de Noviembre 2023Martin ItalianiNo ratings yet
- Stock AhDocument2 pagesStock AhCP KANPURNo ratings yet
- 2018 Mhealth DirectDocument2 pages2018 Mhealth DirectSasha NelsonNo ratings yet
- Hi-Tech Pharmaceuticals: International Price GuideDocument15 pagesHi-Tech Pharmaceuticals: International Price GuideJAHSNo ratings yet
- ListaPrecios SimilaresDocument32 pagesListaPrecios SimilaresSaul Montano Polanco100% (1)
- Receipt 5.17.23 Chloe JuddDocument1 pageReceipt 5.17.23 Chloe JuddMister MisterNo ratings yet
- Payment 664150Document1 pagePayment 664150Mister MisterNo ratings yet
- Chloe Judd's Recheck RecordDocument2 pagesChloe Judd's Recheck RecordMister MisterNo ratings yet
- Prewriting: NameDocument6 pagesPrewriting: NameMister MisterNo ratings yet
- Prewriting: Body: Three Student/teacher Interviews With DetailsDocument6 pagesPrewriting: Body: Three Student/teacher Interviews With DetailsMister MisterNo ratings yet
- C U P S: Editing - CUPS DoneDocument1 pageC U P S: Editing - CUPS DoneMister MisterNo ratings yet
- MNFSTDocument396 pagesMNFSTMister MisterNo ratings yet
- Spookmaster Pumpkin Carving Patterns Book 4Document66 pagesSpookmaster Pumpkin Carving Patterns Book 4Mister MisterNo ratings yet
- Spook Master Pumpkin Carving Templates: Book 1Document63 pagesSpook Master Pumpkin Carving Templates: Book 1Mister MisterNo ratings yet
- Spookmaster Pumpkin Carving Patterns Book 3Document57 pagesSpookmaster Pumpkin Carving Patterns Book 3Mister MisterNo ratings yet
- Ethical Issues Involved in Online Counseling: Practitioners' CornerDocument13 pagesEthical Issues Involved in Online Counseling: Practitioners' CornerabcdNo ratings yet
- 5 Sciatica Exercises For Pain Relief (With Pictures) : Back IntelligenceDocument26 pages5 Sciatica Exercises For Pain Relief (With Pictures) : Back Intelligenceanand sahu100% (1)
- Moving Meditation of SilambamDocument4 pagesMoving Meditation of SilambamGabrielNo ratings yet
- Clement Clarke 100 Year Anniversary BookDocument28 pagesClement Clarke 100 Year Anniversary BookHaag-Streit UK (HS-UK)No ratings yet
- Rounsaville. A Stage of Behavioral Therapies ResearchDocument10 pagesRounsaville. A Stage of Behavioral Therapies ResearchRubí Corona TápiaNo ratings yet
- AQM 65 BrochureDocument30 pagesAQM 65 BrochureEric Thorania KhanNo ratings yet
- Routes of Drug AdministrationDocument34 pagesRoutes of Drug AdministrationNa SyaNo ratings yet
- De Thi Thu Tuyen Sinh Vao Lop 10 Mon Tieng Anh Phong GD DT Tam Dao Vinh Phuc Nam Hoc 2016 2017Document6 pagesDe Thi Thu Tuyen Sinh Vao Lop 10 Mon Tieng Anh Phong GD DT Tam Dao Vinh Phuc Nam Hoc 2016 2017Huyền KhánhNo ratings yet
- Manufacture of RadiopharmaceuticalsDocument9 pagesManufacture of RadiopharmaceuticalsRainMan75No ratings yet
- Navpers 18068F U.S. Navy Enlisted Classification Manual April 2012Document1,612 pagesNavpers 18068F U.S. Navy Enlisted Classification Manual April 2012VietVetSteve100% (1)
- I. Sparq Manufacturing Management Department: Itec854 Danial Bavi / Id: 45485348Document6 pagesI. Sparq Manufacturing Management Department: Itec854 Danial Bavi / Id: 45485348fawas hamdiNo ratings yet
- Material Safety Data Sheet Blended Cement FinalDocument14 pagesMaterial Safety Data Sheet Blended Cement FinalAndrea Dela CruzNo ratings yet
- 20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnDocument161 pages20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnNgọc HuyềnNo ratings yet
- Ankle Sprain ED LeafletDocument2 pagesAnkle Sprain ED LeafletDeborayuni AstutiNo ratings yet
- Challenges of Urban Housing Quality Insights A - 2016 - Procedia - Social and BDocument9 pagesChallenges of Urban Housing Quality Insights A - 2016 - Procedia - Social and BKATE NATALEY CASTILLONo ratings yet
- Horror Story Paige HinckleyDocument15 pagesHorror Story Paige Hinckleyapi-668313628No ratings yet
- Advanced Clinical Naturopathic Medicine Leah Hechtman 2 Full Chapter PDFDocument69 pagesAdvanced Clinical Naturopathic Medicine Leah Hechtman 2 Full Chapter PDFsapitonuk100% (8)
- Counseling Special PopulationsDocument31 pagesCounseling Special PopulationsLore Stefan100% (1)
- Stomach and Duodenum (Forsharing)Document79 pagesStomach and Duodenum (Forsharing)adversal8avrikNo ratings yet
- Gejala Gastrointestinal Pada Pasien COVID-19: Kristianty T. Silangen, Bradley J. Waleleng, Frans E. N. WantaniaDocument8 pagesGejala Gastrointestinal Pada Pasien COVID-19: Kristianty T. Silangen, Bradley J. Waleleng, Frans E. N. WantaniaHedya Nadhrati SururaNo ratings yet
- 4th Periodical Test MapehDocument6 pages4th Periodical Test MapehMichael CasilNo ratings yet
- Keywords To RememberDocument2 pagesKeywords To RememberMajolika Syakira DeviNo ratings yet
- RA-EHS-047-E2 - Covid-19 Site Risk Assessment 002Document16 pagesRA-EHS-047-E2 - Covid-19 Site Risk Assessment 002Samsu RizalNo ratings yet
- Doctor-Patient-Relationship-.ppt (1) 2Document28 pagesDoctor-Patient-Relationship-.ppt (1) 2nketjimotswaledi100% (1)
- Sensus Ruangan 2021Document101 pagesSensus Ruangan 2021Harris JanuarNo ratings yet