
Tone, Power Reflexes - Edited March 2022 (JMS)
Tone, Power Reflexes - Edited March 2022 (JMS)
You might also like
- Answer Key: Introduction To Clinical CodingDocument101 pagesAnswer Key: Introduction To Clinical Codingthamizh555100% (1)
- 100 Diseases Treated by Single Point of AcupunctureDocument209 pages100 Diseases Treated by Single Point of AcupunctureAgeng Rikhmawan100% (32)
- Home Exercise Programs For Musculoskeletal and Sports InjuriesDocument265 pagesHome Exercise Programs For Musculoskeletal and Sports Injuriesvitor flenik100% (5)
- Surface & Radiological Anatomy (3rd Ed) (Gnv64)Document226 pagesSurface & Radiological Anatomy (3rd Ed) (Gnv64)muzaqin100% (2)
- AnatomicalTermsWorksheet NewDocument2 pagesAnatomicalTermsWorksheet NewMark Benedict100% (1)
- The Home Gym Workout BookDocument68 pagesThe Home Gym Workout BookMatthew Dodd100% (3)
- Fit Mamaml - Resistance Tubes Workout GuideDocument57 pagesFit Mamaml - Resistance Tubes Workout GuideGîrï Göwðâ0% (1)
- J-Bands JR Exercise ManualDocument16 pagesJ-Bands JR Exercise Manualca r aNo ratings yet
- Trauma CompleteDocument128 pagesTrauma Completeashvin_7No ratings yet
- Soccer Exercise Library PDFDocument89 pagesSoccer Exercise Library PDFBruno Oliveira Do Nascimento100% (1)
- Sound Healing e BookDocument44 pagesSound Healing e Bookgusperreas7280100% (12)
- 3 PARTS 2 Technical EnglishDocument21 pages3 PARTS 2 Technical EnglishMirian Puma100% (1)
- Lesions of Upper Motor Neurons and Lower Motor NeuronsDocument9 pagesLesions of Upper Motor Neurons and Lower Motor NeuronsJessy Ahmed El DamacyNo ratings yet
- Umn LMN Adn2015Document65 pagesUmn LMN Adn2015Kunal KatyayanNo ratings yet
- NEURO - Retdem: A. Testing For Corneal Reflex (CN5 & CN7 Test)Document1 pageNEURO - Retdem: A. Testing For Corneal Reflex (CN5 & CN7 Test)Peter GirasolNo ratings yet
- Peripheral Nerve InjuriesDocument112 pagesPeripheral Nerve InjuriesManmeet Kaur100% (1)
- Ingles Resumen FinalDocument26 pagesIngles Resumen FinalKarli ValentineNo ratings yet
- Evaluation of Low Back Pain (Ray)Document81 pagesEvaluation of Low Back Pain (Ray)Naeem AminNo ratings yet
- Neurological Examination 3Document46 pagesNeurological Examination 3VIKAS PUNIANo ratings yet
- Amyotrophic Lateral SclerosisDocument12 pagesAmyotrophic Lateral SclerosisdescalzotahNo ratings yet
- Motor TestingDocument58 pagesMotor Testingsarguss14100% (2)
- Claw HandDocument16 pagesClaw HandArum MaharaniNo ratings yet
- Cns Examination: BY Chris VictorDocument35 pagesCns Examination: BY Chris VictorRwabugili ChrisNo ratings yet
- Nerve Injuries Diagnosis, Evaluation and ManagementDocument80 pagesNerve Injuries Diagnosis, Evaluation and ManagementjothiNo ratings yet
- General Neurological Assessment: Shemjaz Arakkal MDocument54 pagesGeneral Neurological Assessment: Shemjaz Arakkal MRaghu NadhNo ratings yet
- MMN Vs NEDocument6 pagesMMN Vs NESBR249No ratings yet
- Carpal Tunnel - Merten (Seminar)Document14 pagesCarpal Tunnel - Merten (Seminar)Adina BotezNo ratings yet
- MNs and MTsDocument32 pagesMNs and MTsJoanna RiveraNo ratings yet
- Seminar-Quadripplegia, Paraplegia, MNDDocument107 pagesSeminar-Quadripplegia, Paraplegia, MNDSalsabila Al-BasheerNo ratings yet
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNo ratings yet
- Motor System: ZHAO Xinyu Department of Neurology The First Affiliated Hospital of Zhengzhou UniversityDocument29 pagesMotor System: ZHAO Xinyu Department of Neurology The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- P9 Disorders of The CerebellumDocument29 pagesP9 Disorders of The CerebellumHomeground entertainmentNo ratings yet
- Lees Testing The ReflexesDocument6 pagesLees Testing The ReflexesIsnan AnshariNo ratings yet
- Polyneuropathies 1Document74 pagesPolyneuropathies 1Bushra EjazNo ratings yet
- Demonstration ReflexDocument40 pagesDemonstration Reflexnikita jainNo ratings yet
- Chapter 29Document93 pagesChapter 29api-3743202No ratings yet
- PTH 645 Ebp Modalities AssignmentDocument12 pagesPTH 645 Ebp Modalities Assignmentapi-680119126No ratings yet
- Brachial Plexus InjuriesDocument64 pagesBrachial Plexus Injuriesprashanth naikNo ratings yet
- Neuromuscular Disorders 2016Document68 pagesNeuromuscular Disorders 2016Alberto MayorgaNo ratings yet
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocument59 pagesWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNo ratings yet
- Appendix: Field Neurological AssessmentDocument10 pagesAppendix: Field Neurological AssessmentLeon LellaNo ratings yet
- Wrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NDocument46 pagesWrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NMurali KarthikkNo ratings yet
- Chapter 10Document45 pagesChapter 10Francisco GaniNo ratings yet
- Assessment: The Neurologic Exam: InterviewDocument10 pagesAssessment: The Neurologic Exam: InterviewJun ManNo ratings yet
- Motor Neuron Signs UMN and LMNDocument2 pagesMotor Neuron Signs UMN and LMNjainlakshay1471No ratings yet
- Professional Skills Review Central Nervous System (CNS)Document25 pagesProfessional Skills Review Central Nervous System (CNS)Noora AlmuailiNo ratings yet
- Examination of The Motor System: Practical Physiology LabDocument20 pagesExamination of The Motor System: Practical Physiology Labحسين سعد حاتم خضيرNo ratings yet
- Hand Assessment - 3rd YrDocument54 pagesHand Assessment - 3rd YrSURBHI AGRAWALNo ratings yet
- Pembekalan BPI Sem 5Document40 pagesPembekalan BPI Sem 5Mukhtar Ali MuktiNo ratings yet
- Clinical and PT OrthopaedicsDocument113 pagesClinical and PT OrthopaedicsVIRESH VNo ratings yet
- 3motor TestingDocument74 pages3motor Testing2013SecBNo ratings yet
- Carpal Tunnel Syndrome-AbiDocument34 pagesCarpal Tunnel Syndrome-AbiSri MahadhanaNo ratings yet
- Manual Therapy: DR - DharmavatiDocument78 pagesManual Therapy: DR - DharmavatiHitesh RohitNo ratings yet
- 9 JosephsonDocument19 pages9 JosephsonTizazu BayihNo ratings yet
- The Spinal Cord,, and Blood Supply To The BrainDocument78 pagesThe Spinal Cord,, and Blood Supply To The BrainMartha MulusaNo ratings yet
- Neurology: by Dennis Jason Alcantara, RN, USRN, MAN CanDocument213 pagesNeurology: by Dennis Jason Alcantara, RN, USRN, MAN CanKristel-Mia Dimalanta RamosNo ratings yet
- Chapter 18: NeurologyDocument22 pagesChapter 18: NeurologypoddataNo ratings yet
- Neurological ExaminationDocument7 pagesNeurological ExaminationKalashini SenadheeraNo ratings yet
- Peripheral Nerve InjuryDocument26 pagesPeripheral Nerve InjuryMercy MercyNo ratings yet
- Examination of The Hand: o o o oDocument5 pagesExamination of The Hand: o o o oGurunadh OrthoNo ratings yet
- NeckDocument67 pagesNeckdr_asaleh100% (1)
- Carpal Tunnel SyndromeDocument33 pagesCarpal Tunnel SyndromeRasYa DINo ratings yet
- Spinal Surgery in The DogDocument38 pagesSpinal Surgery in The Doglovefriends_845661No ratings yet
- Superficial and Deep ReflexesDocument28 pagesSuperficial and Deep ReflexesShilpa SNo ratings yet
- Neural MobilizationDocument50 pagesNeural MobilizationPRIYAM XEROXNo ratings yet
- Motor TestingDocument57 pagesMotor TestinghemaanandhyNo ratings yet
- Carpal Tunnel SyndromeDocument23 pagesCarpal Tunnel Syndromeanon_312039754No ratings yet
- Kuliah UMN - LMN DR - VaniaDocument22 pagesKuliah UMN - LMN DR - Vania22p20015No ratings yet
- SCIENCEDocument51 pagesSCIENCEDrmohamed Kamel MahranNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Cubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- TOP ClinicDocument2 pagesTOP ClinicShan PatelNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- Recap WeekDocument1 pageRecap WeekShan PatelNo ratings yet
- Case 4 HIV MLTC Y3 EDI in Medicine ScenariosDocument1 pageCase 4 HIV MLTC Y3 EDI in Medicine ScenariosShan PatelNo ratings yet
- Case 3 Hot or Cold Food MLTC Y3 EDI in Medicine ScenariosDocument2 pagesCase 3 Hot or Cold Food MLTC Y3 EDI in Medicine ScenariosShan PatelNo ratings yet
- 1b. Epilepsy Role PlayDocument3 pages1b. Epilepsy Role PlayShan PatelNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- Madhus Mayfair Main Menu Nov 21Document2 pagesMadhus Mayfair Main Menu Nov 21Shan PatelNo ratings yet
- 1b Neurology Referrals TaskDocument3 pages1b Neurology Referrals TaskShan PatelNo ratings yet
- PCCT Mens Health - Urology Day 1 SummaryDocument2 pagesPCCT Mens Health - Urology Day 1 SummaryShan PatelNo ratings yet
- 2a Asthma - COPD Role PlaysDocument13 pages2a Asthma - COPD Role PlaysShan PatelNo ratings yet
- EC Workbook - StudentDocument3 pagesEC Workbook - StudentShan PatelNo ratings yet
- PCCT Mens Health - Urology Day 1 Pre-ReadingDocument1 pagePCCT Mens Health - Urology Day 1 Pre-ReadingShan PatelNo ratings yet
- OBSTETRIC History Template V4Document2 pagesOBSTETRIC History Template V4Shan PatelNo ratings yet
- GP Gynae Scenarios - StudentDocument3 pagesGP Gynae Scenarios - StudentShan PatelNo ratings yet
- Role Plays - A Positive Pregnancy Test - StudentDocument1 pageRole Plays - A Positive Pregnancy Test - StudentShan PatelNo ratings yet
- Animal Farm Revision BookletDocument152 pagesAnimal Farm Revision BookletShan PatelNo ratings yet
- 1.0 Functional Classification of Muscles: Agonist (Prime Mover)Document44 pages1.0 Functional Classification of Muscles: Agonist (Prime Mover)Tan Zhen XinNo ratings yet
- PEH 4 - Learning Content - Safety and First Aid (Bandaging) Part 1Document10 pagesPEH 4 - Learning Content - Safety and First Aid (Bandaging) Part 1NiGaPhill OvONo ratings yet
- Mulligan MobilizationDocument70 pagesMulligan MobilizationjayadevanNo ratings yet
- Schneider, 1997Document6 pagesSchneider, 1997fernandaNo ratings yet
- GOOD ONE-tennis and Golfer Elbow - 7 ExDocument1 pageGOOD ONE-tennis and Golfer Elbow - 7 ExSylvia GraceNo ratings yet
- Proximal Humeral Fracture Post-Surgical Rehabilitation ProtocolDocument2 pagesProximal Humeral Fracture Post-Surgical Rehabilitation ProtocolnikithaNo ratings yet
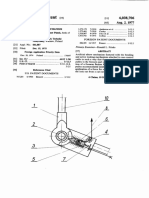
- 1977 - Artificial Elbow Mechanism - Us4038706Document7 pages1977 - Artificial Elbow Mechanism - Us4038706Arturo VaineNo ratings yet
- Yoga Teacher Training Anatomy of Movement For Yoga TeachersDocument22 pagesYoga Teacher Training Anatomy of Movement For Yoga TeachersMarkusNo ratings yet
- Physical Assessment Guide: Part Iii - Musculoskeletal & Neurological Assessment NotesDocument2 pagesPhysical Assessment Guide: Part Iii - Musculoskeletal & Neurological Assessment NotesRue Cheng MaNo ratings yet
- US Marine Corps Daily 16 ProgramDocument12 pagesUS Marine Corps Daily 16 ProgramHip Hop 1919No ratings yet
- Neurological AssessmentDocument12 pagesNeurological AssessmentMushtaha Ibrahim100% (1)
- Continuous Passive Motion: Skate Board/Powder BoardDocument7 pagesContinuous Passive Motion: Skate Board/Powder BoardRahmat DarmawantoroNo ratings yet
- L6. Muscular System (2021-22)Document32 pagesL6. Muscular System (2021-22)Ahmed AfashNo ratings yet
- MAPEH - Physical Education: Quarter 4 - Module 2Document21 pagesMAPEH - Physical Education: Quarter 4 - Module 2Josephine Acio100% (4)
- 14Document28 pages14BrunoNo ratings yet
- Brachial Plexus BookDocument21 pagesBrachial Plexus BookCiro Albuquerque100% (1)
- 5 Basic Barbell LiftsDocument11 pages5 Basic Barbell Liftsmichelletabor100% (1)
- REVIEWER Musculoskeletal SystemDocument8 pagesREVIEWER Musculoskeletal SystemKeren GaciasNo ratings yet





































































































Download as pdf or txt
You might also like
- Answer Key: Introduction To Clinical CodingDocument101 pagesAnswer Key: Introduction To Clinical Codingthamizh555100% (1)
- 100 Diseases Treated by Single Point of AcupunctureDocument209 pages100 Diseases Treated by Single Point of AcupunctureAgeng Rikhmawan100% (32)
- Home Exercise Programs For Musculoskeletal and Sports InjuriesDocument265 pagesHome Exercise Programs For Musculoskeletal and Sports Injuriesvitor flenik100% (5)
- Surface & Radiological Anatomy (3rd Ed) (Gnv64)Document226 pagesSurface & Radiological Anatomy (3rd Ed) (Gnv64)muzaqin100% (2)
- AnatomicalTermsWorksheet NewDocument2 pagesAnatomicalTermsWorksheet NewMark Benedict100% (1)
- The Home Gym Workout BookDocument68 pagesThe Home Gym Workout BookMatthew Dodd100% (3)
- Fit Mamaml - Resistance Tubes Workout GuideDocument57 pagesFit Mamaml - Resistance Tubes Workout GuideGîrï Göwðâ0% (1)
- J-Bands JR Exercise ManualDocument16 pagesJ-Bands JR Exercise Manualca r aNo ratings yet
- Trauma CompleteDocument128 pagesTrauma Completeashvin_7No ratings yet
- Soccer Exercise Library PDFDocument89 pagesSoccer Exercise Library PDFBruno Oliveira Do Nascimento100% (1)
- Sound Healing e BookDocument44 pagesSound Healing e Bookgusperreas7280100% (12)
- 3 PARTS 2 Technical EnglishDocument21 pages3 PARTS 2 Technical EnglishMirian Puma100% (1)
- Lesions of Upper Motor Neurons and Lower Motor NeuronsDocument9 pagesLesions of Upper Motor Neurons and Lower Motor NeuronsJessy Ahmed El DamacyNo ratings yet
- Umn LMN Adn2015Document65 pagesUmn LMN Adn2015Kunal KatyayanNo ratings yet
- NEURO - Retdem: A. Testing For Corneal Reflex (CN5 & CN7 Test)Document1 pageNEURO - Retdem: A. Testing For Corneal Reflex (CN5 & CN7 Test)Peter GirasolNo ratings yet
- Peripheral Nerve InjuriesDocument112 pagesPeripheral Nerve InjuriesManmeet Kaur100% (1)
- Ingles Resumen FinalDocument26 pagesIngles Resumen FinalKarli ValentineNo ratings yet
- Evaluation of Low Back Pain (Ray)Document81 pagesEvaluation of Low Back Pain (Ray)Naeem AminNo ratings yet
- Neurological Examination 3Document46 pagesNeurological Examination 3VIKAS PUNIANo ratings yet
- Amyotrophic Lateral SclerosisDocument12 pagesAmyotrophic Lateral SclerosisdescalzotahNo ratings yet
- Motor TestingDocument58 pagesMotor Testingsarguss14100% (2)
- Claw HandDocument16 pagesClaw HandArum MaharaniNo ratings yet
- Cns Examination: BY Chris VictorDocument35 pagesCns Examination: BY Chris VictorRwabugili ChrisNo ratings yet
- Nerve Injuries Diagnosis, Evaluation and ManagementDocument80 pagesNerve Injuries Diagnosis, Evaluation and ManagementjothiNo ratings yet
- General Neurological Assessment: Shemjaz Arakkal MDocument54 pagesGeneral Neurological Assessment: Shemjaz Arakkal MRaghu NadhNo ratings yet
- MMN Vs NEDocument6 pagesMMN Vs NESBR249No ratings yet
- Carpal Tunnel - Merten (Seminar)Document14 pagesCarpal Tunnel - Merten (Seminar)Adina BotezNo ratings yet
- MNs and MTsDocument32 pagesMNs and MTsJoanna RiveraNo ratings yet
- Seminar-Quadripplegia, Paraplegia, MNDDocument107 pagesSeminar-Quadripplegia, Paraplegia, MNDSalsabila Al-BasheerNo ratings yet
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNo ratings yet
- Motor System: ZHAO Xinyu Department of Neurology The First Affiliated Hospital of Zhengzhou UniversityDocument29 pagesMotor System: ZHAO Xinyu Department of Neurology The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- P9 Disorders of The CerebellumDocument29 pagesP9 Disorders of The CerebellumHomeground entertainmentNo ratings yet
- Lees Testing The ReflexesDocument6 pagesLees Testing The ReflexesIsnan AnshariNo ratings yet
- Polyneuropathies 1Document74 pagesPolyneuropathies 1Bushra EjazNo ratings yet
- Demonstration ReflexDocument40 pagesDemonstration Reflexnikita jainNo ratings yet
- Chapter 29Document93 pagesChapter 29api-3743202No ratings yet
- PTH 645 Ebp Modalities AssignmentDocument12 pagesPTH 645 Ebp Modalities Assignmentapi-680119126No ratings yet
- Brachial Plexus InjuriesDocument64 pagesBrachial Plexus Injuriesprashanth naikNo ratings yet
- Neuromuscular Disorders 2016Document68 pagesNeuromuscular Disorders 2016Alberto MayorgaNo ratings yet
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocument59 pagesWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNo ratings yet
- Appendix: Field Neurological AssessmentDocument10 pagesAppendix: Field Neurological AssessmentLeon LellaNo ratings yet
- Wrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NDocument46 pagesWrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NMurali KarthikkNo ratings yet
- Chapter 10Document45 pagesChapter 10Francisco GaniNo ratings yet
- Assessment: The Neurologic Exam: InterviewDocument10 pagesAssessment: The Neurologic Exam: InterviewJun ManNo ratings yet
- Motor Neuron Signs UMN and LMNDocument2 pagesMotor Neuron Signs UMN and LMNjainlakshay1471No ratings yet
- Professional Skills Review Central Nervous System (CNS)Document25 pagesProfessional Skills Review Central Nervous System (CNS)Noora AlmuailiNo ratings yet
- Examination of The Motor System: Practical Physiology LabDocument20 pagesExamination of The Motor System: Practical Physiology Labحسين سعد حاتم خضيرNo ratings yet
- Hand Assessment - 3rd YrDocument54 pagesHand Assessment - 3rd YrSURBHI AGRAWALNo ratings yet
- Pembekalan BPI Sem 5Document40 pagesPembekalan BPI Sem 5Mukhtar Ali MuktiNo ratings yet
- Clinical and PT OrthopaedicsDocument113 pagesClinical and PT OrthopaedicsVIRESH VNo ratings yet
- 3motor TestingDocument74 pages3motor Testing2013SecBNo ratings yet
- Carpal Tunnel Syndrome-AbiDocument34 pagesCarpal Tunnel Syndrome-AbiSri MahadhanaNo ratings yet
- Manual Therapy: DR - DharmavatiDocument78 pagesManual Therapy: DR - DharmavatiHitesh RohitNo ratings yet
- 9 JosephsonDocument19 pages9 JosephsonTizazu BayihNo ratings yet
- The Spinal Cord,, and Blood Supply To The BrainDocument78 pagesThe Spinal Cord,, and Blood Supply To The BrainMartha MulusaNo ratings yet
- Neurology: by Dennis Jason Alcantara, RN, USRN, MAN CanDocument213 pagesNeurology: by Dennis Jason Alcantara, RN, USRN, MAN CanKristel-Mia Dimalanta RamosNo ratings yet
- Chapter 18: NeurologyDocument22 pagesChapter 18: NeurologypoddataNo ratings yet
- Neurological ExaminationDocument7 pagesNeurological ExaminationKalashini SenadheeraNo ratings yet
- Peripheral Nerve InjuryDocument26 pagesPeripheral Nerve InjuryMercy MercyNo ratings yet
- Examination of The Hand: o o o oDocument5 pagesExamination of The Hand: o o o oGurunadh OrthoNo ratings yet
- NeckDocument67 pagesNeckdr_asaleh100% (1)
- Carpal Tunnel SyndromeDocument33 pagesCarpal Tunnel SyndromeRasYa DINo ratings yet
- Spinal Surgery in The DogDocument38 pagesSpinal Surgery in The Doglovefriends_845661No ratings yet
- Superficial and Deep ReflexesDocument28 pagesSuperficial and Deep ReflexesShilpa SNo ratings yet
- Neural MobilizationDocument50 pagesNeural MobilizationPRIYAM XEROXNo ratings yet
- Motor TestingDocument57 pagesMotor TestinghemaanandhyNo ratings yet
- Carpal Tunnel SyndromeDocument23 pagesCarpal Tunnel Syndromeanon_312039754No ratings yet
- Kuliah UMN - LMN DR - VaniaDocument22 pagesKuliah UMN - LMN DR - Vania22p20015No ratings yet
- SCIENCEDocument51 pagesSCIENCEDrmohamed Kamel MahranNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Cubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- TOP ClinicDocument2 pagesTOP ClinicShan PatelNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- Recap WeekDocument1 pageRecap WeekShan PatelNo ratings yet
- Case 4 HIV MLTC Y3 EDI in Medicine ScenariosDocument1 pageCase 4 HIV MLTC Y3 EDI in Medicine ScenariosShan PatelNo ratings yet
- Case 3 Hot or Cold Food MLTC Y3 EDI in Medicine ScenariosDocument2 pagesCase 3 Hot or Cold Food MLTC Y3 EDI in Medicine ScenariosShan PatelNo ratings yet
- 1b. Epilepsy Role PlayDocument3 pages1b. Epilepsy Role PlayShan PatelNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- Madhus Mayfair Main Menu Nov 21Document2 pagesMadhus Mayfair Main Menu Nov 21Shan PatelNo ratings yet
- 1b Neurology Referrals TaskDocument3 pages1b Neurology Referrals TaskShan PatelNo ratings yet
- PCCT Mens Health - Urology Day 1 SummaryDocument2 pagesPCCT Mens Health - Urology Day 1 SummaryShan PatelNo ratings yet
- 2a Asthma - COPD Role PlaysDocument13 pages2a Asthma - COPD Role PlaysShan PatelNo ratings yet
- EC Workbook - StudentDocument3 pagesEC Workbook - StudentShan PatelNo ratings yet
- PCCT Mens Health - Urology Day 1 Pre-ReadingDocument1 pagePCCT Mens Health - Urology Day 1 Pre-ReadingShan PatelNo ratings yet
- OBSTETRIC History Template V4Document2 pagesOBSTETRIC History Template V4Shan PatelNo ratings yet
- GP Gynae Scenarios - StudentDocument3 pagesGP Gynae Scenarios - StudentShan PatelNo ratings yet
- Role Plays - A Positive Pregnancy Test - StudentDocument1 pageRole Plays - A Positive Pregnancy Test - StudentShan PatelNo ratings yet
- Animal Farm Revision BookletDocument152 pagesAnimal Farm Revision BookletShan PatelNo ratings yet
- 1.0 Functional Classification of Muscles: Agonist (Prime Mover)Document44 pages1.0 Functional Classification of Muscles: Agonist (Prime Mover)Tan Zhen XinNo ratings yet
- PEH 4 - Learning Content - Safety and First Aid (Bandaging) Part 1Document10 pagesPEH 4 - Learning Content - Safety and First Aid (Bandaging) Part 1NiGaPhill OvONo ratings yet
- Mulligan MobilizationDocument70 pagesMulligan MobilizationjayadevanNo ratings yet
- Schneider, 1997Document6 pagesSchneider, 1997fernandaNo ratings yet
- GOOD ONE-tennis and Golfer Elbow - 7 ExDocument1 pageGOOD ONE-tennis and Golfer Elbow - 7 ExSylvia GraceNo ratings yet
- Proximal Humeral Fracture Post-Surgical Rehabilitation ProtocolDocument2 pagesProximal Humeral Fracture Post-Surgical Rehabilitation ProtocolnikithaNo ratings yet
- 1977 - Artificial Elbow Mechanism - Us4038706Document7 pages1977 - Artificial Elbow Mechanism - Us4038706Arturo VaineNo ratings yet
- Yoga Teacher Training Anatomy of Movement For Yoga TeachersDocument22 pagesYoga Teacher Training Anatomy of Movement For Yoga TeachersMarkusNo ratings yet
- Physical Assessment Guide: Part Iii - Musculoskeletal & Neurological Assessment NotesDocument2 pagesPhysical Assessment Guide: Part Iii - Musculoskeletal & Neurological Assessment NotesRue Cheng MaNo ratings yet
- US Marine Corps Daily 16 ProgramDocument12 pagesUS Marine Corps Daily 16 ProgramHip Hop 1919No ratings yet
- Neurological AssessmentDocument12 pagesNeurological AssessmentMushtaha Ibrahim100% (1)
- Continuous Passive Motion: Skate Board/Powder BoardDocument7 pagesContinuous Passive Motion: Skate Board/Powder BoardRahmat DarmawantoroNo ratings yet
- L6. Muscular System (2021-22)Document32 pagesL6. Muscular System (2021-22)Ahmed AfashNo ratings yet
- MAPEH - Physical Education: Quarter 4 - Module 2Document21 pagesMAPEH - Physical Education: Quarter 4 - Module 2Josephine Acio100% (4)
- 14Document28 pages14BrunoNo ratings yet
- Brachial Plexus BookDocument21 pagesBrachial Plexus BookCiro Albuquerque100% (1)
- 5 Basic Barbell LiftsDocument11 pages5 Basic Barbell Liftsmichelletabor100% (1)
- REVIEWER Musculoskeletal SystemDocument8 pagesREVIEWER Musculoskeletal SystemKeren GaciasNo ratings yet