Download as pdf or txt
You might also like
- PE 06 Seepage FlownetsDocument22 pagesPE 06 Seepage FlownetsIshmam Shahid100% (1)
- TESCO Systems Integration BrochureDocument2 pagesTESCO Systems Integration Brochuredavev2005No ratings yet
- Exam (Q) Set ADocument13 pagesExam (Q) Set Aflowerpot321100% (1)
- How To Create and Configure DME FileDocument3 pagesHow To Create and Configure DME FilesairamsapNo ratings yet
- Qin 2018Document5 pagesQin 2018sadNo ratings yet
- LungSEEK - 3D Selective Kernel Residual Network For Pulmonary Nodule DiagnosisDocument14 pagesLungSEEK - 3D Selective Kernel Residual Network For Pulmonary Nodule DiagnosisRonald BbosaNo ratings yet
- Lung Cancer DetectionDocument5 pagesLung Cancer Detectionkoushikraj900No ratings yet
- 2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesDocument9 pages2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesgraythomasinNo ratings yet
- 3d-Detection Clasification 01Document10 pages3d-Detection Clasification 01sadNo ratings yet
- 21pami LungnoduleDocument13 pages21pami Lungnoduledreadrebirth2342No ratings yet
- MEDS-Net - Multi-Encoder Based Self-Distilled Network With Bidirectional Maximum Intensity Projections Fusion For Lung Nodule DetectionDocument15 pagesMEDS-Net - Multi-Encoder Based Self-Distilled Network With Bidirectional Maximum Intensity Projections Fusion For Lung Nodule Detection무하마드 / 학생 / 컴퓨터공학부No ratings yet
- Accepted For Publication in IEEE International Symposium On Biomedical Imaging (ISBI) 2017Document4 pagesAccepted For Publication in IEEE International Symposium On Biomedical Imaging (ISBI) 2017Rekka MastouriNo ratings yet
- 10 1002@ima 22445Document13 pages10 1002@ima 22445barti koksNo ratings yet
- 10 1109@iccsp48568 2020 9182258Document4 pages10 1109@iccsp48568 2020 9182258mindaNo ratings yet
- 2D3D Clasification 01Document11 pages2D3D Clasification 01sadNo ratings yet
- Multi-Branch Ensemble Learning Architecture Based On 3D CNN For False Positive Reduction in Lung Nodule DetectionDocument12 pagesMulti-Branch Ensemble Learning Architecture Based On 3D CNN For False Positive Reduction in Lung Nodule DetectionRonald BbosaNo ratings yet
- A Review of Convolutional Neural Network-Based Computer Aided Lung Nodule Detection SystemDocument18 pagesA Review of Convolutional Neural Network-Based Computer Aided Lung Nodule Detection SystemIAES IJAINo ratings yet
- Lung CancerDocument10 pagesLung Cancerbvkarthik2711No ratings yet
- IEEE PAPER BATCH NO-03 A NOVEL OBJECT DETECTION MODEL (YOLOv5) FOR IMPROVED LUNG NODULE IDENTIFICATION IN MEDICAL IMAGESDocument7 pagesIEEE PAPER BATCH NO-03 A NOVEL OBJECT DETECTION MODEL (YOLOv5) FOR IMPROVED LUNG NODULE IDENTIFICATION IN MEDICAL IMAGESS.GOPINATH5035No ratings yet
- LDNNET Towards Robust Classification of Lung Nodule and Cancer Using Lung Dense Neural NetworkDocument20 pagesLDNNET Towards Robust Classification of Lung Nodule and Cancer Using Lung Dense Neural Networkswathi sNo ratings yet
- Evaluate The Malignancy of Pulmonary Nodules Using The 3-D Deep Leaky Noisy-OR NetworkDocument13 pagesEvaluate The Malignancy of Pulmonary Nodules Using The 3-D Deep Leaky Noisy-OR NetworkTeam2 ResearchNo ratings yet
- Deep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule IdentificationDocument9 pagesDeep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule Identificationdreadrebirth2342No ratings yet
- A New Framework For Multi Scale CNN Based Malignancy Classification of Pulmonary Lung NodulesDocument9 pagesA New Framework For Multi Scale CNN Based Malignancy Classification of Pulmonary Lung NodulesFahad SherwaniNo ratings yet
- Lung Tumor Classification and Detection From CTDocument6 pagesLung Tumor Classification and Detection From CTAatmaja JoshiNo ratings yet
- Lung Nodule Detection Via 3D U-Net and Contextual Convolutional Neural NetworkDocument7 pagesLung Nodule Detection Via 3D U-Net and Contextual Convolutional Neural Networkdreadrebirth2342No ratings yet
- A Hybrid Approach To Detect and Classify Pulmonary Carcinoma Nodules in Computed Tomography ScansDocument7 pagesA Hybrid Approach To Detect and Classify Pulmonary Carcinoma Nodules in Computed Tomography ScansselvaNo ratings yet
- Smart Hand Report ContentDocument26 pagesSmart Hand Report Contentproxyone taskNo ratings yet
- Article 1Document4 pagesArticle 1Tashu SardaNo ratings yet
- A Comparative Study of Tuberculosis DetectionDocument5 pagesA Comparative Study of Tuberculosis DetectionMehera Binte MizanNo ratings yet
- A Novel Object Detection Model (Yolov5) For Improved Lung Nodule Identification in Medical ImagesDocument8 pagesA Novel Object Detection Model (Yolov5) For Improved Lung Nodule Identification in Medical ImagesS.GOPINATH5035No ratings yet
- Deepln: An Artificial Intelligence-Based Automated System For Lung Cancer ScreeningDocument12 pagesDeepln: An Artificial Intelligence-Based Automated System For Lung Cancer ScreeningNexgen TechnologyNo ratings yet
- 1015 2178 3 RVDocument10 pages1015 2178 3 RVd PrayamaNo ratings yet
- Transfer Learning Based Deep Learning Framework For Identification of Type of Brain TumorDocument6 pagesTransfer Learning Based Deep Learning Framework For Identification of Type of Brain TumorTole SutiknoNo ratings yet
- 2023 A Literature Review On "Lung Cancer Detection Approaches Using Medical Images"Document9 pages2023 A Literature Review On "Lung Cancer Detection Approaches Using Medical Images"graythomasinNo ratings yet
- Efficacy of Algorithms in Deep Learning On Brain Tumor Cancer Detection (Topic Area Deep Learning)Document8 pagesEfficacy of Algorithms in Deep Learning On Brain Tumor Cancer Detection (Topic Area Deep Learning)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Pneumonia Detection With Deep Convolutional Architecture: Abstract - Pneumonia Is A Respiratory Disease Caused by AnDocument4 pagesPneumonia Detection With Deep Convolutional Architecture: Abstract - Pneumonia Is A Respiratory Disease Caused by AnMoynul Hasan RonyNo ratings yet
- Lung Paper - ModifiedDocument12 pagesLung Paper - ModifiedMaheswari VutukuriNo ratings yet
- Pulmonary Tuberculosis Detection Using Deep LearningConvolutional Neural NetworksDocument5 pagesPulmonary Tuberculosis Detection Using Deep LearningConvolutional Neural NetworksShoumik MuhtasimNo ratings yet
- Computer Aided Diagnosis System For Detection of Lung Cancer in CT Scan ImagesDocument5 pagesComputer Aided Diagnosis System For Detection of Lung Cancer in CT Scan Imagesprabhabathi deviNo ratings yet
- A NOVEL OBJECT DETECTION MODEL (YOLOv5) FOR IMPROVED LUNG NODULE IDENTIFICATION IN MEDICAL IMAGESDocument8 pagesA NOVEL OBJECT DETECTION MODEL (YOLOv5) FOR IMPROVED LUNG NODULE IDENTIFICATION IN MEDICAL IMAGESS.GOPINATH5035No ratings yet
- Deep Learning Approach For Unprecedented Lung Disease PrognosisDocument5 pagesDeep Learning Approach For Unprecedented Lung Disease PrognosisMulla Abdul FaheemNo ratings yet
- Impact of Local Histogram Equalization On Deep Learning Architectures For Diagnosis Ofcovid-19 On Chest X-RaysDocument5 pagesImpact of Local Histogram Equalization On Deep Learning Architectures For Diagnosis Ofcovid-19 On Chest X-RaysSerhanNarliNo ratings yet
- Detecting and Recognising Lung Cancer: Using Convolutional Neural NetworksDocument25 pagesDetecting and Recognising Lung Cancer: Using Convolutional Neural NetworksRAJU MAURYANo ratings yet
- TB Detection in Chest Radiograph Using Deep Learning ArchitectureDocument12 pagesTB Detection in Chest Radiograph Using Deep Learning ArchitectureYazid BastomiNo ratings yet
- TB Detection in Chest Radiograph Using Deep Learning ArchitectureDocument12 pagesTB Detection in Chest Radiograph Using Deep Learning ArchitectureYazid BastomiNo ratings yet
- 1705 09435Document9 pages1705 09435ShivamKapoorNo ratings yet
- Batch-3 Lung Nodule Detection (Ieee Paper)Document3 pagesBatch-3 Lung Nodule Detection (Ieee Paper)S.GOPINATH5035No ratings yet
- A Literature Review On Techniques For Detection of Lung DiseasesDocument8 pagesA Literature Review On Techniques For Detection of Lung DiseasesIJRASETPublicationsNo ratings yet
- Measurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDocument8 pagesMeasurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDiego Alejandro Betancourt PradaNo ratings yet
- A Novel Data Augmentation Method Using Style-Based GAN For Robust Pulmonary Nodule SegmentationDocument6 pagesA Novel Data Augmentation Method Using Style-Based GAN For Robust Pulmonary Nodule Segmentationnavneet prabhakarNo ratings yet
- Paper 48-Lung Cancer DetectionDocument7 pagesPaper 48-Lung Cancer DetectionSushmaNo ratings yet
- Pneumonia Detection in X-Ray Chest Images BasedDocument7 pagesPneumonia Detection in X-Ray Chest Images BasedyuniNo ratings yet
- Development of Hybrid Convolutional Neural Network and Autoregressive Integrated Moving Average On Computed Tomography Image ClassificationDocument9 pagesDevelopment of Hybrid Convolutional Neural Network and Autoregressive Integrated Moving Average On Computed Tomography Image ClassificationIAES IJAINo ratings yet
- Efficient Lung Infection Detection Using Machine Learning ApproachDocument9 pagesEfficient Lung Infection Detection Using Machine Learning ApproachIJRASETPublicationsNo ratings yet
- Lung Nodule Detection and Classification From Thorax CT-scan Using RetinaNet With Transfer LearningDocument11 pagesLung Nodule Detection and Classification From Thorax CT-scan Using RetinaNet With Transfer LearningIvan WilsonoNo ratings yet
- EasyChair Preprint 545Document6 pagesEasyChair Preprint 545Greeni MarcoNo ratings yet
- 12 III March 2024Document9 pages12 III March 2024ychennupalliNo ratings yet
- Research PaperDocument5 pagesResearch PaperCSE HODNo ratings yet
- Dong PDFDocument8 pagesDong PDFFikri HaekalNo ratings yet
- Improved Accuracy of Brain Tumor Detection Using VGG16Document9 pagesImproved Accuracy of Brain Tumor Detection Using VGG16IJRASETPublicationsNo ratings yet
- Anapub Paper TemplateDocument10 pagesAnapub Paper Templatebdhiyanu87No ratings yet
- Zhao2018 AGILE CNNDocument11 pagesZhao2018 AGILE CNNrekka mastouriNo ratings yet
- Lung Nodule Classification Using Deep Features in CT ImagesDocument6 pagesLung Nodule Classification Using Deep Features in CT Imagesthereviewer185No ratings yet
- Textbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationFrom EverandTextbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationNo ratings yet
- Qin 2018Document5 pagesQin 2018sadNo ratings yet
- 2D3D Clasification 01Document11 pages2D3D Clasification 01sadNo ratings yet
- Tang 2019Document4 pagesTang 2019sadNo ratings yet
- Detection of Pulmonary Nodules From CT Scans: Martin Dolej S IDocument65 pagesDetection of Pulmonary Nodules From CT Scans: Martin Dolej S IsadNo ratings yet
- Luna16 01Document7 pagesLuna16 01sadNo ratings yet
- Antoine 2018Document43 pagesAntoine 2018sadNo ratings yet
- 3d-Detection Clasification 01Document10 pages3d-Detection Clasification 01sadNo ratings yet
- Dou 2017 AutomatedDocument10 pagesDou 2017 AutomatedsadNo ratings yet
- Your Canadian Arrival GuideDocument24 pagesYour Canadian Arrival GuidesadNo ratings yet
- TADANO Gr300ex3Document157 pagesTADANO Gr300ex3Abi Jith100% (1)
- Direccion 1Document62 pagesDireccion 1Jesús RoseroNo ratings yet
- Yarn Examining MachineDocument3 pagesYarn Examining MachineAbrõ Wazir100% (1)
- Ultra DTMR m08 Ing r2Document4 pagesUltra DTMR m08 Ing r2Cerduardo Chanchisco Roga RojasNo ratings yet
- According To Use: Main Auxiliary According To Passage of Flue GasesDocument11 pagesAccording To Use: Main Auxiliary According To Passage of Flue GasesAbdallah MansourNo ratings yet
- VTK File FormatsDocument19 pagesVTK File FormatshamishlewisNo ratings yet
- The Lava LampDocument5 pagesThe Lava LampMathew DegamoNo ratings yet
- Annex A - Scope of WorkDocument4 pagesAnnex A - Scope of Workمهيب سعيد الشميريNo ratings yet
- Worksheet 9Document4 pagesWorksheet 9Regina CunninghamNo ratings yet
- Resolute - Fanuc - L 9517 9442 04 C (En) PDFDocument7 pagesResolute - Fanuc - L 9517 9442 04 C (En) PDFeletropaulomococaNo ratings yet
- Two Kinds of ReasoningDocument11 pagesTwo Kinds of ReasoningRipleyrose19100% (1)
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- LT-951 FR-320 Installation and Operation ManualDocument88 pagesLT-951 FR-320 Installation and Operation ManualkumaraguruNo ratings yet
- Nuvoton ISP-ICP Gang Programmer: User ManualDocument14 pagesNuvoton ISP-ICP Gang Programmer: User ManualTony KututoNo ratings yet
- 3 The MPEG Data StreamDocument12 pages3 The MPEG Data Streamanshab bedariNo ratings yet
- ISA RP3.2-1960 Flange Mounted Sharp Edged Orifice Plate For Flow Measurement PDFDocument8 pagesISA RP3.2-1960 Flange Mounted Sharp Edged Orifice Plate For Flow Measurement PDFamshahNo ratings yet
- Object Oriented Software Engineering 3rd Edition 614 817Document204 pagesObject Oriented Software Engineering 3rd Edition 614 817JUAN ABEL CALLUPE CUEVANo ratings yet
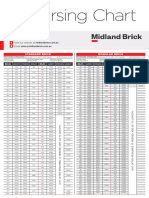
- Midland Brick Coursing ChartDocument2 pagesMidland Brick Coursing ChartMichael Slater100% (1)
- Dtu, Department of Energy Engineering S in (KJ/ (KG K) ) - V in (M 3/Kg) - T in (ºc) M.J. Skovrup & H.J.H Knudsen. 19-11-29 Ref:Dupont Suva Hp62Document1 pageDtu, Department of Energy Engineering S in (KJ/ (KG K) ) - V in (M 3/Kg) - T in (ºc) M.J. Skovrup & H.J.H Knudsen. 19-11-29 Ref:Dupont Suva Hp62Diego RamirezNo ratings yet
- Introduction To Data Analytics For Business - AnswersDocument8 pagesIntroduction To Data Analytics For Business - AnswersShabaan HossainNo ratings yet
- (Tex Ebook) - Advanced LatexDocument23 pages(Tex Ebook) - Advanced LatexenricosirolaNo ratings yet
- Machine Learning The BasicsDocument158 pagesMachine Learning The BasicsDomNo ratings yet
- Modeling and Applications of 3D Flow in Orifice Plate at Low Turbulent Reynolds NumbersDocument7 pagesModeling and Applications of 3D Flow in Orifice Plate at Low Turbulent Reynolds NumbersLucas BomfimNo ratings yet
- Fiery Color Test Page: PMS 640CDocument3 pagesFiery Color Test Page: PMS 640CElvÏs ElvÏs100% (1)
- Hendrickson Assignment4Document11 pagesHendrickson Assignment4Angel Nicole SorianoNo ratings yet
- Selection, Design, and Installation of Thermoplastic Water-Pressure Piping SystemsDocument8 pagesSelection, Design, and Installation of Thermoplastic Water-Pressure Piping SystemsAcácio AlvesNo ratings yet