Download as pdf or txt
You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
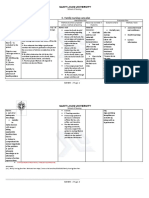
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 pagesC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Expanded 3P Study Guide YasminaIrinaDocument79 pagesExpanded 3P Study Guide YasminaIrinaikNo ratings yet
- Suppurative Lung DiseaseDocument45 pagesSuppurative Lung DiseasemusabNo ratings yet
- Munity Acquired PneumoniaDocument4 pagesMunity Acquired PneumoniaDIVEN SolvonNo ratings yet
- Lung Parasitic InfectionsDocument71 pagesLung Parasitic InfectionswaheedaNo ratings yet
- PneumoniaDocument27 pagesPneumoniasebghatullah mubarezNo ratings yet
- Chronic Cough Differential DiagnosisDocument6 pagesChronic Cough Differential DiagnosisUbaidillah HafidzNo ratings yet
- He Pat Ology 2016Document26 pagesHe Pat Ology 2016Kay BristolNo ratings yet
- Paediatric-Chronic CoughDocument66 pagesPaediatric-Chronic CoughIzyan NadhirahNo ratings yet
- Sumbul Parveen PneumoniaDocument27 pagesSumbul Parveen Pneumoniaabhishekchoudhary81689No ratings yet
- Oxygen Saturation (If Available) : IagnosisDocument3 pagesOxygen Saturation (If Available) : Iagnosisrezairfan221No ratings yet
- 6.pneumonia (New)Document104 pages6.pneumonia (New)sallykartikaNo ratings yet
- W1 L2 PneumoniaDocument57 pagesW1 L2 PneumoniaAnas FikriNo ratings yet
- Respiratory System2Document134 pagesRespiratory System2Darell M. BookNo ratings yet
- Lu Lu Waterhouse, MD PGY-3 July 13, 2012Document12 pagesLu Lu Waterhouse, MD PGY-3 July 13, 2012Emily EresumaNo ratings yet
- Pulmonary ConditionsDocument42 pagesPulmonary ConditionsMinetteNo ratings yet
- 3 - Suppurative Lung Diseases Dr. RehabDocument2 pages3 - Suppurative Lung Diseases Dr. RehabMayar JaradNo ratings yet
- Pneumonia: Arto Yuwono Soeroto Sub Bag Pulmonologi Bagian Ilmu Penyakit Dalam FK UNPAD / RSUP Dr. Hasan Sadikin BandungDocument28 pagesPneumonia: Arto Yuwono Soeroto Sub Bag Pulmonologi Bagian Ilmu Penyakit Dalam FK UNPAD / RSUP Dr. Hasan Sadikin BandungMochamad HuseinNo ratings yet
- Pediatric PneumoniaDocument58 pagesPediatric PneumoniaJohn Christopher LucesNo ratings yet
- 1-Ammar Notes (Med & Pedia)Document23 pages1-Ammar Notes (Med & Pedia)anmar alkhudhri100% (1)
- Tuberculosis in Infancy and ChildhoodDocument8 pagesTuberculosis in Infancy and ChildhoodsamioNo ratings yet
- 12lower Respiratory Tract InfectionDocument44 pages12lower Respiratory Tract Infectionmehdikhalid09No ratings yet
- AMK DiseasesDocument384 pagesAMK Diseaseshanif ahmadNo ratings yet
- BPNDocument49 pagesBPNlovelots1234100% (1)
- Pneumonia: Shervin GolbariDocument24 pagesPneumonia: Shervin GolbarisgolbariNo ratings yet
- Pulmonar y TuberculosisDocument35 pagesPulmonar y TuberculosistuyalimonNo ratings yet
- Aspiration PneumoniaDocument22 pagesAspiration PneumoniaAya AlamsjahNo ratings yet
- Respiratory Disorders in ChildrenDocument77 pagesRespiratory Disorders in ChildrenJharaNo ratings yet
- COUGHDocument3 pagesCOUGHnathanaellee92No ratings yet
- 13-Community Acquired PneumoniaDocument50 pages13-Community Acquired PneumoniaRubina MasihNo ratings yet
- Respiratory MedicineDocument9 pagesRespiratory MedicineroseNo ratings yet
- PneumoniaDocument38 pagesPneumoniaAzhar GhoriNo ratings yet
- Suppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversityDocument65 pagesSuppurative Lung Diseases: DR Taher El Naggar Prof of Pulmonary Medicine Ain Shams UniversitykingmedicNo ratings yet
- L23 - Pneumonia MedDocument51 pagesL23 - Pneumonia MedAL-ashai MohammedNo ratings yet
- NCP PneumoniaDocument2 pagesNCP Pneumoniajulz_otso6359No ratings yet
- Uworld Peds MicroDocument5 pagesUworld Peds MicroJoan ChoiNo ratings yet
- Board Review: PediatricsDocument215 pagesBoard Review: Pediatricsokurimkuri94% (16)
- Miliary TBDocument20 pagesMiliary TBIvan SeligNo ratings yet
- Respiratory Pathology: Dr. Okon MRCSDocument38 pagesRespiratory Pathology: Dr. Okon MRCSEdwin OkonNo ratings yet
- 6.pneumonia (New)Document104 pages6.pneumonia (New)Ryana Fitriana IINo ratings yet
- San Lazaro Question Bank SouthPark 2Document9 pagesSan Lazaro Question Bank SouthPark 2Kenneth MiguelNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Lab 4 LRTI Part OneDocument27 pagesLab 4 LRTI Part OnenohaNo ratings yet
- Pleural EffusionDocument22 pagesPleural EffusionNARUTONo ratings yet
- Upper and Lower Respiratory Tract Infections Including Infections in Immunocompromised Patients (Adam Hunt's Conflicted Copy 2014-12-08)Document5 pagesUpper and Lower Respiratory Tract Infections Including Infections in Immunocompromised Patients (Adam Hunt's Conflicted Copy 2014-12-08)Adam HuntNo ratings yet
- Pulmo Viewboxes BLOCK 8Document251 pagesPulmo Viewboxes BLOCK 8U.P. College of Medicine Class 2014100% (2)
- P E: R F: Aediatric Mergencies Espiratory AilureDocument38 pagesP E: R F: Aediatric Mergencies Espiratory AilureAfiqah So Jasmi100% (1)
- W1 L1 URTI (Outdated)Document41 pagesW1 L1 URTI (Outdated)Anas FikriNo ratings yet
- Upper Airway Obstruction: Croup and Its DifferentialDocument36 pagesUpper Airway Obstruction: Croup and Its DifferentialJoseph Stans KasiryeNo ratings yet
- PertussisDocument17 pagesPertussisAbduraman NazifNo ratings yet
- Stridor, Aspiration, and Cough in ChildrenDocument41 pagesStridor, Aspiration, and Cough in ChildrenArif Rahman DmNo ratings yet
- HemoptysisDocument32 pagesHemoptysisbudiNo ratings yet
- SS Visser, Pulmonology Internal Medicine UPDocument33 pagesSS Visser, Pulmonology Internal Medicine UPRonnie JaderNo ratings yet
- Emergency in Respiratory MedicineDocument73 pagesEmergency in Respiratory MedicineIndra MahaputraNo ratings yet
- Pneumonia: H. Ridwan M. Daulay Wisman Dalimunthe Rini S. DaulayDocument49 pagesPneumonia: H. Ridwan M. Daulay Wisman Dalimunthe Rini S. DaulayKhairani PutriNo ratings yet
- L2 PneumoniaDocument12 pagesL2 Pneumoniajojoanoo15No ratings yet
- Lung AbscessDocument28 pagesLung AbscessBobet ReñaNo ratings yet
- EmpyemaDocument18 pagesEmpyemaRomMy WiEn MicKhoNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Rule: Human Drugs: Vaginal Contraceptive and Spermicide Products (OTC) Containing Nonoxynol 9 Label RequirementsDocument17 pagesRule: Human Drugs: Vaginal Contraceptive and Spermicide Products (OTC) Containing Nonoxynol 9 Label RequirementsJustia.comNo ratings yet
- Chapter 1Document19 pagesChapter 1Sanjaya PoudelNo ratings yet
- Pioneers in MicrobiologyDocument34 pagesPioneers in MicrobiologyJasmin Pearl AndayaNo ratings yet
- Dip HIV Man (SA) Regulations 24-1-2017Document9 pagesDip HIV Man (SA) Regulations 24-1-2017matentenNo ratings yet
- Individuals at Risk From Poor Nutritional IntakeDocument24 pagesIndividuals at Risk From Poor Nutritional IntakeaibutyNo ratings yet
- BPH Fourth Year Curriculum of Purbanchal University PDFDocument41 pagesBPH Fourth Year Curriculum of Purbanchal University PDFPawan MahtoNo ratings yet
- 10 Diagnosa TerbanyakDocument6 pages10 Diagnosa TerbanyakErnyNo ratings yet
- Case Study: ScenarioDocument4 pagesCase Study: ScenarioCheska PalomaNo ratings yet
- What Is The Difference Between Disease and Disorder - A Guide PDFDocument8 pagesWhat Is The Difference Between Disease and Disorder - A Guide PDFDanish505No ratings yet
- Edukasi Dan Demonstrasi Pedoman Gizi Seimbang Untuk Anak Sehat Dan BerprestasiDocument12 pagesEdukasi Dan Demonstrasi Pedoman Gizi Seimbang Untuk Anak Sehat Dan BerprestasiSiti Aysyah SiregarNo ratings yet
- Laws On Notifiable DiseaseDocument43 pagesLaws On Notifiable DiseaseKenji ToleroNo ratings yet
- The Impact of Nutrition and Lifestyle Habits On The Health of Undergraduate University StudentsDocument5 pagesThe Impact of Nutrition and Lifestyle Habits On The Health of Undergraduate University StudentsAyanda KakazaNo ratings yet
- Pelvic Inflammatory DiseaseDocument10 pagesPelvic Inflammatory DiseaseSusana Soto López100% (2)
- Being Healthy and Fit in Simple Terms Means Taking Good Care of The Body PDFDocument3 pagesBeing Healthy and Fit in Simple Terms Means Taking Good Care of The Body PDFolympianbestNo ratings yet
- 1.AMSP StrategiesDocument57 pages1.AMSP StrategiesVeera RaghavanNo ratings yet
- Types of VaccinesDocument21 pagesTypes of VaccinesAtoillah IsvandiaryNo ratings yet
- Daftar Pustaka: Raka, L, 2010Document2 pagesDaftar Pustaka: Raka, L, 2010dnoksNo ratings yet
- Self-Declaration / Undertaking by Day Scholars-Students / Post Docs/ Project Staff (Returning To IIT Madras Laboratories)Document3 pagesSelf-Declaration / Undertaking by Day Scholars-Students / Post Docs/ Project Staff (Returning To IIT Madras Laboratories)akruNo ratings yet
- Zanamivir (Relenza)Document2 pagesZanamivir (Relenza)Rafael MusicasNo ratings yet
- Nursing Seminar 1 SAS Session 3Document7 pagesNursing Seminar 1 SAS Session 3Ven SemillaNo ratings yet
- Project Proposal Portable Handwashing DeviceDocument2 pagesProject Proposal Portable Handwashing DeviceChris100% (1)
- Wins EnablersDocument8 pagesWins Enablersireniomadayag100% (1)
- Reading Comprehension: 1. Are The Following Statements True or False ? Justify!Document2 pagesReading Comprehension: 1. Are The Following Statements True or False ? Justify!anaNo ratings yet
- National Health PolicyDocument31 pagesNational Health PolicyGayathri R0% (1)
- Handwashing Lesson LogDocument4 pagesHandwashing Lesson LogJoseph Bahian-AbangNo ratings yet
- English Presentation!Document13 pagesEnglish Presentation!German AcostaNo ratings yet
- TSA WinS Booklet Sanitation FINAL WEB 20181105Document68 pagesTSA WinS Booklet Sanitation FINAL WEB 20181105Reg Sevilla SibalNo ratings yet
- WJ Ms Paper Sir 2013Document13 pagesWJ Ms Paper Sir 2013Rohan sharmaNo ratings yet
- STD Treatment ChartDocument5 pagesSTD Treatment ChartIYERBK100% (1)