Professional Documents
Culture Documents
Articulo 6
Articulo 6
Uploaded by
Carol RuizCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Articulo 6
Articulo 6
Uploaded by
Carol RuizCopyright:
Available Formats
PLOS ONE
RESEARCH ARTICLE
Comparison of antibiotic use and antibiotic
resistance between a community hospital and
tertiary care hospital for evaluation of the
antimicrobial stewardship program in Japan
Mika Morosawa1,2, Takashi Ueda ID3, Kazuhiko Nakajima3, Tomoko Inoue4,
Masanobu Toyama4, Hitoshi Ogasiwa5, Miki Doi5, Yasuhiro Nozaki2, Yasushi Murakami2,
Makoto Ishii1, Yoshio Takesue ID3,6*
a1111111111
1 Department of Respiratory Medicine, Nagoya University Graduate School of Medicine, Nagoya, Japan,
a1111111111
2 Department of Respiratory Medicine, Tokoname City Hospital, Tokoname, Aichi, Japan, 3 Department of
a1111111111 Infection Control and Prevention, Hyogo College of Medicine, Nishinomiya, Japan, 4 Department of
a1111111111 Pharmacy, Tokoname City Hospital, Tokoname, Aichi, Japan, 5 Department of Clinical Technology,
a1111111111 Tokoname City Hospital, Tokoname, Aichi, Japan, 6 Department of Clinical Infectious Diseases, Tokoname
City Hospital, Tokoname, Japan
* takesuey@hyo-med.ac.jp
OPEN ACCESS
Citation: Morosawa M, Ueda T, Nakajima K, Inoue Abstract
T, Toyama M, Ogasiwa H, et al. (2023) Comparison
of antibiotic use and antibiotic resistance between a Assessment of risk-adjusted antibiotic use (AU) is recommended to evaluate antimicrobial
community hospital and tertiary care hospital for stewardship programs (ASPs). We aimed to compare the amount and diversity of AU and
evaluation of the antimicrobial stewardship antimicrobial susceptibility of nosocomial isolates between a 266-bed community hospital
program in Japan. PLoS ONE 18(4): e0284806.
(CH) and a 963-bed tertiary care hospital (TCH) in Japan. The days of therapy/100 bed days
https://doi.org/10.1371/journal.pone.0284806
(DOT) was measured for four classes of broad-spectrum antibiotics predominantly used for
Editor: Kwame Kumi Asare, University of Cape
hospital-onset infections. The diversity of AU was evaluated using the modified antibiotic
Coast, GHANA
heterogeneity index (AHI). With 10% relative DOT for fluoroquinolones and 30% for each of
Received: November 7, 2022
the remaining three classes, the modified AHI equals 1. Multidrug resistance (MDR) was
Accepted: April 6, 2023 defined as resistance to � 3 anti-Pseudomonas antibiotic classes. The DOT was signifi-
Published: April 24, 2023 cantly higher in the TCH than in the CH (10.85 ± 1.32 vs. 3.89 ± 0.93, p < 0.001). For risk-
Peer Review History: PLOS recognizes the adjusted AU, the DOT was 6.90 ± 1.50 for acute-phase medical wards in the CH, and 8.35 ±
benefits of transparency in the peer review 1.05 in the TCH excluding the hematology department. In contrast, the DOT of antibiotics
process; therefore, we enable the publication of for community-acquired infections was higher in the CH than that in the TCH. As quality
all of the content of peer review and author
assessment of AU, higher modified AHI was observed in the TCH than in the CH (0.832 ±
responses alongside final, published articles. The
editorial history of this article is available here: 0.044 vs. 0.721 ± 0.106, p = 0.003), indicating more diverse use in the TCH. The MDR rate
https://doi.org/10.1371/journal.pone.0284806 in gram-negative rods was 5.1% in the TCH and 3.4% in the CH (p = 0.453). No significant
Copyright: © 2023 Morosawa et al. This is an open difference was demonstrated in the MDR rate for Pseudomonas aeruginosa and Enterobac-
access article distributed under the terms of the teriaceae species between hospitals. Broad-spectrum antibiotics were used differently in
Creative Commons Attribution License, which the TCH and CH. However, an increased antibiotic burden in the TCH did not cause poor
permits unrestricted use, distribution, and
reproduction in any medium, provided the original
susceptibility, possibly because of diversified AU. Considering the different patient popula-
author and source are credited. tions, benchmarking AU according to the facility type is promising for inter-hospital compari-
Data Availability Statement: All relevant data are
sons of ASPs.
within the paper and its Supporting Information
files.
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 1 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Funding: The author(s) received no specific Introduction
funding for this work.
In the era of global antimicrobial resistance (AMR), antimicrobial stewardship (AS) programs
Competing interests: Y. Takesue received grant
have become common in most institutions to reduce antimicrobial selective pressure [1–4].
support from Shionogi & Co., Ltd. and payment for
lectures from Astellas Pharma Inc. and MSD
Concomitant with adequate infection control, AS programs reduce AMR rates at individual
Japan. The other authors have no conflict of institutions [3–6]. AS programs, including prospective audits and feedback as well as formu-
interest to declare. lary restrictions and preauthorization, can effectively decrease antibiotic use in comparison
with the pre-intervention phase [7–10]. In general, the relative intra-hospital change in antibi-
otic use is monitored in the evaluation of AS programs in each hospital. However, chronic
excess use of antibiotics can be overlooked until AMR develops only with the monitoring of
intra-hospital trend. On the other hand, further decreases in hospital antibiotic use may not be
feasible in institutions where comprehensive AS activity has been ongoing for several years.
Hence, establishment of uniform standards for the target level of antibiotic use is required.
Without proper benchmarks, the implementation of AS programs cannot effectively promote
the optimal use of antimicrobials in health care facilities.
Patient populations at tertiary care hospitals (TCHs) have higher degrees of disease severity
and are more severely immunocompromised, which together result in more complicated
infections in comparison with patients in community hospitals (CHs) [11]. Thus, a greater
degree of antibiotic use is imperative in TCHs than in CHs, even with adjustment for bed
number. In addition, beds are shared for convalescent phase rehabilitation care in some CHs.
Hence, different benchmarks should be determined for TCHs and CHs. Inter-hospital com-
parisons of risk-adjusted antibiotic use are recommended [12]. To provide a risk-adjusted
benchmark of antibiotic use, the Centers for Disease Control and Prevention (CDC) developed
the standardized antimicrobial administration ratio (SAAR) [13]. The SAAR is a novel AS
metric that compares actual to expected antimicrobial use. However, the SAAR cannot be used
worldwide owing to different backgrounds of hospitalized patients in the United States (US) in
comparison with patients in other countries, including Japan, as well as different systems of
health care and health insurance [14]. Although a Korean SAAR [15] has been developed, such
a risk-adjusted benchmark is not available in many countries and this is somewhat complex to
calculate for universal use.
In addition to the amount of antibiotic use, several authors have reported the usefulness of
antibiotic diversity to prevent AMR [16–19]. Recently, Ueda et al. [20] evaluated balanced use
of broad-spectrum antibiotics using the antibiotic heterogeneity indices (AHIs). The authors
found a negative correlation between the indices and rate of AMR in Pseudomonas aeruginosa
and Klebsiella pneumoniae. The aim of this study was to compare the amount and diversity of
broad-spectrum antibiotic use to assess the performance of AS programs in a CH and a TCH
in Japan. The rates of AMR of clinical isolates in these hospitals were also evaluated as out-
comes of the respective AS programs. This study represents an early step in developing risk-
adjusted benchmarks for antimicrobial use in Japan.
Methods
This study was conducted at Tokoname City Hospital and Hyogo Medical University Hospital.
Tokoname City Hospital is a 266-bed CH (136 beds for acute-phase medical wards) where no
intensive care unit (ICU) is present and is one of four designated medical institutions for spec-
ified infectious diseases certified by the Japanese government. Hyogo Medical University Hos-
pital is a 963-bed TCH with an ICU and departments that perform organ transplantation
procedures including hematopoietic stem cell transplantation, as well as other highly special-
ized services. The departments in each hospital are listed in S1 Table.
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 2 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Data were collected from April 2021 to March 2022. This is a retrospective study of medical
records or archived samples, and all data were fully anonymized before we accessed them. This
study was approved by the institutional review boards at Hyogo Medical University (No. 4194)
and Tokoname City Hospital (No 2022–1). Ethics committee waived the requirement for
informed consent.
The previous AS team in the CH comprised one pharmacist and two medical technologists
in clinical microbiology with 25% full-time equivalent each, with the support of a physician
from another hospital who joined AS meetings held once a week. Interventions were carried
out for patients with bloodstream infection or meningitis, isolation of multidrug-resistant
organisms, and use of antibiotics for longer than 14 days. With the launch of the Department
of Infectious Disease, a new multidisciplinary AS program was established in April 2021 at
Tokoname City Hospital. The new AS team in this CH comprised one infectious disease physi-
cian, one pulmonologist, two pharmacists with 30% full-time equivalent each, three nurses,
and two medical technologists in clinical microbiology. Although AS meetings were held twice
a week at this CH, an infectious disease physician checked the medical chart every weekday as
needed for patients with bacteremia or those with serious infections for whom frequent time-
outs were required.
An infection prevention and control department was established in 2006 at Hyogo Medical
University Hospital, the TCH in this study. During the study period, the AS program was con-
ducted by one infectious disease physician, a pharmacist dedicated to the AS program, and an
infection control nurse, with additional input from a microbiologist. AS rounds were con-
ducted every weekday in this TCH. Prospective audits, feedback, and consultation service with
antibiotic timeouts were the main components of the AS programs at both hospitals. Interven-
tions occurred in the following situations: 1) in both hospitals, when input was received from
the microbiology laboratory that a patient had bloodstream infection or meningitis or when
multidrug-resistant organisms were isolated; 2) when input was received from the pharmaceu-
tical department that broad-spectrum antibiotics with anti-Pseudomonas activity were started
(TCH: piperacillin/tazobactam and carbapenems; CH: piperacillin/tazobactam, carbapenems,
fluoroquinolone, fourth-generation cephems/ceftazidime/aztreonam, and aminoglycosides) or
with prolonged use of antimicrobials (TCH: longer than 10 days for carbapenems and pipera-
cillin/tazobactam and longer than 14 days for the remaining intravenous antimicrobial agents;
CH: longer than 7 days for all intravenous and oral antimicrobial agents). Additionally, the AS
program in the CH intervened with the use of anti-methicillin-resistant Staphylococcus aureus
drugs, antifungal, or antiviral drugs, or drugs needing therapeutic drug monitoring. AS teams
in both hospitals supervised antibiotic therapy when clinicians contacted them for advice.
Days of therapy (DOTs)/100 bed days (DOT) were used for the comparison of antibiotic
use. We compared DOT values for common intravenous broad-spectrum antibiotics with
anti-Pseudomonas activity, which were predominantly used for hospital-onset infections
including carbapenems, piperacillin/tazobactam, fourth-generation cephalosporins (i.e., cefe-
pime and cefozopran)/ceftazidime/aztreonam, and fluoroquinolones. This category of antibi-
otics was defined as broad-spectrum antibiotics in this study. The TCH is a high-volume
center for allogeneic hematopoietic stem cell transplantation. To decrease the bias in antibiotic
use, the DOT at the TCH excluding the division of hematology was also evaluated. Because
beds in the CH are shared for acute-phase medical care, convalescent phase rehabilitation care,
and community-based integrated care, DOT only for acute-phase medical care wards in the
CH was also compared with DOT in the TCH.
In addition to comparisons between the two hospitals, changes in broad-spectrum antibi-
otic use were determined in the CH to evaluate the impact of the new AS team. Thus, the pre-
(April 2018 to March 2021) and post-intervention periods were compared. The primary study
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 3 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
period compared with the TCH (April 2021 to March 2022) was considered term 1 and the fol-
low-up period after the introduction of the new antibiotic use policy (April 2022 to September
2022) which was proposed based on the previous one year antibiotic use pattern in term 1 was
considered term 2. Because the DOT [6] calculation system was not available until March 2021
in the CH, the comparison between pre- and post-establishment of the new AS team was made
using the defined daily dose (DDDs)/100 bed days (DDD) [5]. The new assumed average
maintenance dose [21] per day for each drug was used for calculation of DDDs.
Using modified categories of intravenous antimicrobial agents reported by the National
Healthcare Safety Network [6], we also compared antibiotic use in the TCH and the CH with
respect to the following: antibiotics predominantly used for community-acquired infections,
including ampicillin/sulbactam, ceftriaxone/cefotaxime, and macrolides; first- and second-
generation cephalosporins mainly used for surgical prophylaxis; antibiotics predominantly
used for infections with extensively antibiotic-resistant gram-negative organisms; intravenous
antibiotics predominantly used for resistant gram-positive infections; intravenous antibiotics
with antifungal activity; and antiviral agents.
To assess the heterogeneous use of the four classes of broad-spectrum antibiotics used for
hospital-onset infections, we evaluated the relative DOT (% DOT) and the AHIs. The % DOT
was calculated as the DOT of one class of antibiotic divided by the DOT of all four classes of
broad-spectrum antibiotics. The method of calculating AHIs were demonstrated in S1 Fig.
The AHI [18, 22, 23] was calculated as follows:
AHI ¼ 1 fn=ð2 � ½n 1�Þg � Sjai bi j
where n = 4 (the number of antimicrobial classes); ai = 0.25 for each antibiotic class; and bi =
observed proportion of the DOT for each antibiotic class. The AHI is the index when all antibi-
otic classes are equally used (% DOT = 25%). When 25% of the relative DOT in each antibiotic
class is achieved, the AHI is 1. The modified AHI, which is a new indicator of balanced antibi-
otic use, was also calculated by defining ai as 0.1 for fluoroquinolones and 0.3 for each of the
remaining three antibiotic class [20]. The modified AHI is the index when each antibiotic class
(% DOT = 30%) except for fluoroquinolones (% DOT = 10%) is equally used.
The evaluated organisms were glucose non-fermenting gram-negative rods including P.
aeruginosa and Acinetobacter spp.; Enterobacteriaceae species including Escherichia coli, Kleb-
siella pneumoniae, K. oxytoca, K. aerogenes, Enterobacter cloacae, Enterobacter spp., Citrobacter
freundii, Proteus mirabillis, P. vulgaris, Serratia marcescens, and Morganella morganii. Clinical
isolates from all specimens except stool were used in this study to exclude the influence of sur-
veillance cultures for AMR organisms. The following sampling techniques were recommended
in both hospitals. Specimens were collected using strict aseptic technique. Specimens were col-
lected prior to the administration of antimicrobial agents, avoiding contamination with indig-
enous flora. Swab specimens were unacceptable, with a few exceptions. Specimens were to be
delivered at room temperature to the laboratory as soon as possible. If delayed transport was
anticipated, urine, stool, and respiratory specimens were refrigerated (not blood specimens). If
anaerobic culture was required, anaerobic collection containers were used. Additionally, the
following procedures were recommended for blood culture collection. Peripheral blood was
collected via venipuncture rather than via indwelling vascular catheter. Blood culture bottle
tops were cleaned with antiseptic. Chlorhexidine alcohol was used for skin preparation, allow-
ing the site to dry for at least 30 seconds before venipuncture. Sufficient blood (20–30 mL) was
drawn and each bottle was inoculated with 10 mL of the sample; at least two sets were required.
Changing needles prior to inoculating blood culture bottles was not recommended because of
the risk for needle-stick injury.
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 4 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Organisms isolated from specimens obtained later than 48 hours after admission were
defined as nosocomial isolates. If two or more strains of the same bacterial species were iso-
lated from an individual patient, the most resistant strain was selected for the analysis. Antibi-
otic susceptibility was determined according to criteria of the European Committee on
Antimicrobial Susceptibility Testing (EUCAST) [24] and the Clinical and Laboratory Stan-
dards Institute (CLSI) [25] (S2 Table). Resistance according to EUCAST and resistance/inter-
mediate susceptibility according to CLSI for at least two of the following antibiotic classes were
analyzed: ciprofloxacin, cefepime, tazobactam/piperacillin, meropenem, and gentamycin/ami-
kacin. MDR was defined as resistant gram-negative rods according to EUCAST (or resistance/
intermediate susceptibility according to CLSI) for at least three of the antibiotics listed above.
Isolates of carbapenemase and extended-spectrum β-lactamase (ESBL)-producing Entero-
bacteriaceae were also compared. A nitrocefin disk (cefinase; BD, Tokyo, Japan) was used to
detect β-lactamase production by gram-negative bacteria, according to the manufacturer’s
instructions. The Cica-Beta Test (Kanto Chemical, Tokyo, Japan) was used to detect ESBL-
and metallo-β-lactamase-producing gram-negative bacteria by directly scraping the colony
and applying it to the disk. Multiplex nested PCR (BioFire FilmArray panel, Biomerieux
Japan, Tokyo) was used to determine the production of carbapenemase.
Categorical variables were compared using chi-squared or Fisher’s exact tests. Continuous
variables are expressed as mean (standard deviation) and were compared using t-tests or
Mann–Whitney U tests. Although the DOT or DDD during the period of interest (e.g., one cal-
endar year) was usually monitored, the mean monthly DOT or DDD during a specific time
frame was also evaluated for the statistical analysis. The level of statistical significance was set at
p < 0.05. IBM SPSS ver. 24 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
Results
Comparison between the TCH and CH regarding antibiotic use and
antibiotic resistant rate in gram-negative rods
During the 1-year study period, there were 256,377 patient days in the TCH and 63,033 in the
CH. The rates of AS events eliciting input from the microbiology laboratory and from the
pharmaceutical department were 59.3% and 29.2%, respectively, in the CH and 17.7% and
27.7%, respectively, in the TCH. The remaining events were consultations from physicians; the
rates were 11.5% in the CH and 54.6% in the TCH. Because of a smaller number of hospital-
ized patients in the CH, wider indications for AS interventions were adopted in the CH than
in the TCH; the number of interventions per 100 patient days was 1.25 events in the CH and
0.48 events in the TCH. Timeouts between the initiation and completion of antimicrobial ther-
apy were more frequent in the TCH than in the CH (cumulative number of timeouts per one
event: 8.6 and 2.5, respectively), indicating that complicated or refractory infections were
treated more often in the TCH.
The mean monthly DOT of the broad-spectrum antibiotics predominantly used for hospi-
tal-onset infections was 10.85 ± 1.31 in the TCH, 8.35 ± 1.05 in the TCH excluding the division
of hematology, 3.89 ± 0.93 in the CH, and 6.90 ± 1.50 in the acute-phase medical wards of the
CH (Table 1). The DOT was significantly higher in the TCH than those in the CH (p < 0.001)
and acute-phase medical wards in the CH (p < 0.001). Even when the division of hematology
was excluded in the TCH, the difference was still significant when compared with the CH
(p < 0.001) and acute-phase medical wards in the CH (p = 0.012). The mean monthly DOT of
antibiotics used for resistant gram-positive infections and that of anti-fungal agents were also
significantly higher in the TCH than those in the CH (Table 1). In contrast, the DOT of antibi-
otics predominantly used for community-acquired infections was significantly smaller in the
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 5 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Table 1. Day of therapy of each category of intravenous antimicrobials in the tertiary care hospital and the community hospital between April 2021 and March
2022.
Category of intravenous antimicrobial agents Day of therapy
Tertiary care Tertiary care hospital, excluding the Community Community hospital (acute-
hospital division of hematology hospital phase medical wards)
Broad-spectrum antibiotics predominantly used 10.85 ± 1.31 8.35 ± 1.05 3.89 ± 0.93*, § 6.90 ± 1.50*, ‡
for hospital-onset infections
Antibiotics predominantly used for community- 5.12 ± 0.62 5.39 ± 0.66 6.27 ± 1.21†, ¶ 11.74 ± 2.50*, §
acquired infections
Antibiotics used for resistant gram-positive 2.51 ± 0.47 1.99 ± 0.33 0.38 ± 0.31 *, § 0.63 ± 0.59*, §
infections
Anti-fungal agents 1.89 ± 0.46 0.52 ± 0.22 0.17 ± 0.16 *, § 0.36 ± 0.35*
* <0.001
†
p = 0.008 (vs. tertiary care hospital)
§
<0.001
‡
p = 0.012
¶
p = 0.038 (vs. tertiary care hospital, excluding division of hematology)
https://doi.org/10.1371/journal.pone.0284806.t001
TCH (5.12 ± 0.62) than those in the CH (6.27 ± 1.21, p = 0.008) and acute-phase medical
wards in the CH (11.74 ± 2.50, p < 0.001). The DOT throughout the 1-year study period for
each category of intravenous antimicrobial agent is presented in S3 Table.
The DOT of each broad-spectrum antibiotic predominantly used for hospital-onset infections
and the AHIs for this category of antibiotics are presented in Table 2. A significantly higher modi-
fied AHI was shown in the TCH than in the CH (0.832 ± 0.044 vs. 0.721 ± 0.106, p = 0.003), indi-
cating a more heterogeneous (balanced) use of these antibiotics in the TCH (the target of the
AHIs was 1). If the division of hematology was excluded in the TCH, a further increase in the
Table 2. Day of therapy (DOT) in each broad-spectrum antibiotic predominantly used for hospital-onset infections, and antibiotic heterogeneity indices (AHIs)
for this category antibiotics in the tertiary care hospital and community hospital.
Markers of antibiotic use Tertiary care Tertiary care hospital, excluding Community Community hospital (acute-
hospital the division of hematology hospital phase medical wards)
DOT of broad-spectrum antibiotics predominantly
used for hospital-onset infections (relative DOT)
Carbapenems 4.32 ± 0.48 2.53 ± 0.28 (30.3%) 1.13 ± 0.46 2.29 ± 1.04 (33.1%)
(39.8%) (29.1%)
Piperacillin/tazobactam 3.51 ± 0.55 2.93 ± 0.49 (35.1%) 1.76 ± 0.68 3.19 ± 1.12 (46.2%)
(32.3%) (45.3%)
Fourth-generation cephalosporins, ceftazidime, 2.20 ± 0.43 2.11 ± 0.44 (25.3%) 0.71 ± 0.35 1.05 ± 0.71 (15.2%)
aztreonam (20.3%) (18.3%)
Fluoroquinolone 0.82 ± 0.22 0.78 ± 0.15 (9.3%) 0.28 ± 0.20 (7.3%) 0.38 ± 0.37 (5.5%)
(7.5%)
AHI (for 25% use in each of the four classes) 0.704 ± 0.048 0.773 ± 0.031 0.636 ± 0.113*, ¶ 0.569 ± 0.148§, ¶
†, ¶
Modified AHI (for 30% use in three classes, except for 0.832±0.044 0.914±0.047 0.721±0.106 0.665±0.137 ‡, ¶
fluoroquinolones [10%])
Mean monthly DOT and AHIs between April 2021 and March 2022 were shown.
* p = 0.068
†
p = 0.003
§
p = 0.007
‡
p < 0.001 (vs. tertiary care hospital)
¶
p < 0.001 (vs. tertiary care hospital, excluding division of hematology)
https://doi.org/10.1371/journal.pone.0284806.t002
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 6 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
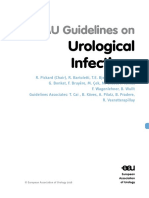
Fig 1. Resistant rate according to the European Committee on Antimicrobial Susceptibility Testing criteria in
nosocomial isolates of Gram-negative rods (GNRs), glucose-non-fermenting GNRs and Enterobacteriaceae species
between the tertiary care hospital and community hospital.
https://doi.org/10.1371/journal.pone.0284806.g001
AHIs was observed (AHI, 0.773 ± 0.031; and modified AHI, 0.914 ± 0.047). Excess use of pipera-
cillin/tazobactam (% DOT = 45.3%) caused lower AHIs in the CH. The % DOT of piperacillin/
tazobactam was 46.2% when acute-phase medical wards in the CH were evaluated.
In total, 2530 and 559 strains of gram-negative rods were isolated, and 1812 and 262 noso-
comial isolates were analyzed in the TCH and CH, respectively. The rate of nosocomial isolates
in the TCH was significantly higher than that in the CH (71.6% vs. 46.9%, p < 0.001). In other
words, community-acquired infections were treated more frequently in the CH. Resistance
rates in gram-negative rods among all nosocomial isolates were similar between the TCH and
CH (resistant to �2 classes: 15.8% vs. 12.6%, p = 0.174; and resistant to �3 classes: 5.1% vs.
3.4%, p = 0.458, respectively). There was no significant difference in the resistance rates
among glucose-non-fermenting gram-negative rods (resistant to � 2 classes: p = 0.452;
and � 3 classes: p = 0.207) and Enterobacteriaceae species (resistant to � 2 classes: p = 0.256;
and � 3 classes: p = 0.969) between these two hospitals (Fig 1).
The results of isolation of resistant strains of each organism according to EUCAST and of
non-susceptible strains according to CLSI criteria are shown in Table 3 and S4 Table, respec-
tively. No significant difference in the rate of resistance to � 2 classes (p = 0.413) and to � 3
classes (p = 0.147) was observed for P. aeruginosa between the TCH and CH. No Acinetobacter
spp. strains resistant to � 2 classes were isolated in either hospital. The isolation rates of ESBL-
producing E. coli were similar (26.7% in the TCH and 25.7% in the CH), and there was no sig-
nificant difference in the rates of resistance to � 2 classes (p = 0.196) and to � 3 classes
(p = 0.948) for E. coli between these hospitals. In contrast, the rate of ESBL-producing K. pneu-
moniae tended to be higher in the TCH than the rate in the CH (16.4% vs. 2.9%, p = 0.068).
However, the rate of MDR (� 3 classes) remained at 7.3% in the TCH.
Changes in the use of broad-spectrum antibiotics before and after
establishment of a new AS team in the CH
In the CH, the DDD decreased significantly, from 3.73 ± 0.87 (p = 0.003), 4.21 ± 0.79
(p < 0.001), and 3.59 ± 0.64 (p = 0.003) in the previous 3 consecutive years, respectively, before
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 7 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Table 3. Resistant rate according to the European Committee on Antimicrobial Susceptibility Testing criteria and beta-lactamase-producing rate in each organism
in the tertiary care hospital and community hospital.
Antibiotic resistant strains No of resistant strains or β-lactamase-producing strains among nosocomial isolates (%) p-value
Tertiary care hospital (n = 1812) Community hospital (n = 262)
Pseudomonas aeruginosa n = 296 n = 43
�2 classes resistance 61 (20.6%) 6 (14.0%) 0.413
�3 classes resistance 41 (13.9%) 2 (4.7%) 0.147
Acinetobacter spp. n = 68 n=5
�2 classes resistance 0 (0.0%) 0 (0%) –
�3 classes resistance 0 (0.0%) 0 (0%) –
Escherichia coli n = 561 n = 113
�2 classes resistance 152 (27.1%) 24 (21.2%) 0.196
�3 classes resistance 26 (4.6%) 6 (5.3%) 0.948
ESBL producing strains 144 (26.7%) 29 (25.7%) 0.999
carbapenemase producing strains 0 (0%) 0 (0%) –
Klebsiella pneumoniae n = 305 n = 34
�2 classes resistance 46 (15.1%) 1 (2.9%) 0.092
�3 classes resistance 22 (7.3%) 1 (2.9%) 0.562
ESBL-producing strains 50 (16.4%) 1 (2.9%) 0.068
carbapenemase-producing strains 0 (0%) 0 (0%) –
Klebsiella oxytoca n = 132 n = 14
�2 classes resistance 3 (2.3%) 0 (0%) 0.674
�3 classes resistance 1 (0.8%) 0 (0%) –
ESBL-producing strains 0 (0%) 0 (0%) –
carbapenemase-producing strains 0 (0%) 0 (0%) –
Klebsiella aerogenes n = 68 n=7
�2 classes resistance 2 (2.9%) 1 (14.2%) 0.656
�3 classes resistance 1 (1.5%) 0 (0%) –
ESBL-producing strains 0 (0%) 0 (0%) –
carbapenemase-producing strains 0 (0%) 0 (0%) –
Enterobacter spp.. n = 190 n = 21
�2 classes resistance 19 (10.0%) 1 (4.8%) 0.700
�3 classes resistance 1 (0.5%) 0 (0%) –
ESBL-producing strains 1 (0.5%) 0 (0%) –
carbapenemase-producing strains 0 (0%) 0 (0%) –
Other Enterobacteriaceae species n = 192 n = 25
�2 classes resistance 4 (2.1%) 0 (0%) 0.951
�3 classes resistance 1 (0.5%) 0 (0%) –
ESBL-producing strains 2 (1.0%) 0 (0%) –
carbapenemase-producing strains 1 (0.5%) 0 (0%) –
ESBL: extended spectrum β-lactamase
https://doi.org/10.1371/journal.pone.0284806.t003
the establishment of a new AS team, to 2.62 ± 0.78 in term 1 after establishment of a new AS
team (Fig 2). In the evaluation of DDD for acute phase medical wards, there were also signifi-
cant differences between the pre-establishment period (April 2019–March 2020 [p = 0.003];
and April 2020–March 2021 [p = 0.011]) and term-1 in the post-establishment period.
Frequent use of piperacillin/tazobactam (% DDD: 63.4% between April 2018 and March
2019, 60.6% between April 2019 and March 2020, and 48.2% between April 2020 and March
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 8 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Fig 2. Change of antibiotic use of broad-spectrum antibiotics before and after a new antimicrobial stewardship (AS) team in the community hospital.
DDD: defined daily dose; DOT: day of therapy. Grey bar showed mean monthly DDD and black bar showed mean monthly DOT during the corresponding
period.
https://doi.org/10.1371/journal.pone.0284806.g002
2021) and infrequent use of fourth-generation cephalosporins/ceftazidime/aztreonam (%
DDD: 8.8%, 10.4%, and 10.0%, respectively) were characterized as the antibiotic use pattern
before establishment of a new AS team (Table 4). Although the % DDD of fourth-generation
cephalosporins/ceftazidime/aztreonam increased to 17.6%, the % DDD of piperacillin/
Table 4. Defined daily dose (DDD) of each broad-spectrum antibiotic commonly used for hospital-onset infections and the antibiotic heterogeneity indices (AHIs)
before and after establishment of a new antimicrobial stewardship (AS) team in the community hospital.
Markers of antibiotic use for broad-spectrum antibiotics Before establishment of a new AS team After establishment of a new AS
predominantly used for hospital-onset infections team
Apr 2018–Mar Apr 2019–Mar Apr 2020–Mar Apr 2021–Mar 2022 Term 1
2019 2020 2021
DDD (relative Piperacillin/tazobactam 2.37 (63.4%) 2.63 (60.6%) 1.73 (48.2%) 1.17 (44.8%)
DDD) Fourth-generation cephalosporins, ceftazidime, 0.33 (8.8%) 0.45 (10.4%) 0.36 (10.0%) 0.46 (17.6%)
aztreonam
Carbapenems 0.93 (24.9%) 1.05 (24.2%) 1.24 (34.5%) 0.72 (27.6%)
Fluoroquinolones 0.10 (2.7%) 0.21 (4.8%) 0.26 (7.2%) 0.26 (10.0%)
AHIs AHI 0.460 ± 0.089* 0.547 ± 0.133 0.558 ± 0.089† 0.653 ± 0.128
§
Modified AHI 0.558 ± 0.108 0.619 ± 0.121 0.667 ± 0.079 0.713 ± 0.107
* p<0.001
†
p = 0.045
§
p = 0.002 (vs. AHIs after establishment of a new AS team)
https://doi.org/10.1371/journal.pone.0284806.t004
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 9 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Fig 3. Relative day of therapy of each broad-spectrum antibiotic commonly used for hospital-onset infections in term 1 and term 2 after establishment of
a new antibiotic stewardship team in the community hospital. Gray bar shows DOT in term 1 and black bar shows DOT in term 2.
https://doi.org/10.1371/journal.pone.0284806.g003
tazobactam remained high (44.8%) in term 1 after establishment of the new AS team. A signifi-
cant improvement in antibiotic heterogeneity was observed only for the AHI (0.653 ± 0.128 vs.
0.558 ± 0.089, p = 0.045) but not for the modified AHI during term 1 in comparison with the
preceding 1 year before establishment of a new AS team (Table 4). For the further improve-
ment of antibiotic heterogeneity, the use of piperacillin/tazobactam was discouraged by the AS
team and alternative use of fourth-generation cephalosporins was recommended after April
2022 if broad-spectrum antibiotics with anti-Pseudomonas activity were required. Interven-
tions by the AS team and the adherence rates in term 2 are presented in S5 Table. The cumula-
tive number of interventions was 344 in 192 events (1.79/event). Discontinuation of
antibiotics in patients with prolonged use or non-infectious conditions was a leading reason
for intervention (55.7%), followed by alteration of antibiotics other than de-escalation or intra-
venous to oral stepdown (40.1%). The overall adherence rate was 89.0% (306/344).
Following this policy, the % DOT for piperacillin/tazobactam decreased from
45.40 ± 11.72% in term 1 to 31.88 ± 9.76% in term 2 (p = 0.028), and the % DOT of fourth-gen-
eration cephalosporins/ceftazidime/aztreonam increased from 17.61 ± 6.45% to 26.03 ± 6.23%
(p = 0.018) (Fig 3), resulting in a significant increase in the AHI (from 0.636 ± 0.113 to
0.746 ± 0.050, p = 0.039) and modified AHI (from 0.721 ± 0.106 to 0.859 ± 0.107, p = 0.019)
(Table 5). In the evaluation of acute-phase medical wards in the CH, a significant decrease in
the % DOT of piperacillin-tazobactam (from 46.81 ± 15.13% to 31.27 ± 7.63% p = 0.032) and a
significant increase in the % DOT of fourth-generation cephalosporins/ceftazidime/aztreonam
(from 14.29 ± 8.19% to 25.33 ± 7.22%, p = 0.013) was also achieved in term 2 compared with
term 1 (S6 Table). No difference in the total DOT of broad-spectrum antibiotics was observed
between the two terms for all wards (term 1: 3.89 ± 0.93 and term 2: 3.79 ± 0.59, p = 0.820) and
acute-phase medical wards (term 1: 6.90 ± 1.50; and term 2: 6.85 ± 0.96, p = 0.949) (S6 Table).
Table 5. Antibiotic heterogeneity indices (AHIs) in term 1 and term 2 after the establishment of a new antibiotic stewardship team in the community hospital.
AHIs Term 1 (Apr 2021–Mar 2022) after establishment of a new AS team Term 2 (Apr 2022–Sep 2022) after establishment of a new AS team p-value
AHI 0.636 ± 0.113 0.746 ± 0.050 0.039
Modified 0.721 ± 0.106 0.859 ± 0.107 0.019
AHI
https://doi.org/10.1371/journal.pone.0284806.t005
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 10 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
Discussion
We compared AS programs, several markers for antibiotic use, and antibiotic susceptibility
between the CH and the TCH in this study. Because of a smaller number of admitted patients
in the CH, AS intervention could be more widely indicated in the CH than in the TCH; the
number of interventions per 100 patient days was 1.25 in the CH and 0.48 in the TCH, respec-
tively. Similarly, the odds ratio was 5.7 in small- to middle-sized hospitals for conducting inter-
ventions within 7 days after the initiation of broad-spectrum antimicrobials [1], compared
with large hospitals in Japan. In the present study, even with adjustment for patient days, intra-
venous antibiotic use was substantially different between the TCH and the CH. The DOT of
broad-spectrum antibiotics predominantly used for hospital-onset infections was 3.89 in the
CH and 10.85 in the TCH. For risk-adjusted antibiotic use, we also found that the DOT of
broad-spectrum antibiotics was 6.90 for acute-phase medical wards in the CH and 8.35 in the
TCH excluding the division of hematology.
In an analysis of 576 hospitals in the US (number of beds � 500, 14%), the DOT of anti-
Pseudomonas drugs was 24.5 [26]. Although oral fluoroquinolones and antibiotics for MDR
gram-negative rods were included in the study, a difference in antibiotic use might exist
between the US and Japan. The SAAR was developed by the CDC to provide a risk-adjusted
benchmark of antibiotic use. Ueda et al. [20] reported the SAAR of broad-spectrum antibiotics
predominantly used for hospital-onset infections in a Japanese TCH. Between 2015 and 2022,
the SAAR ranged from 1.10 to 1.82 in the ICU, from 0.50 to 1.03 in the department of respira-
tory medicine, and from 0.70 to 1.20 in the department of colorectal surgery.
In addition to broad-spectrum antibiotics for hospital-onset infections, a significantly
higher DOT of antibiotics used for resistant gram-positive infections and antifungal agents
was observed in the TCH in comparison with the CH in this study, suggesting frequent empir-
ical and targeted use of these antimicrobial agents for serious infections in the TCH. In con-
trast, antibiotics predominantly used for community-acquired infections were more
frequently used in the CH than in the TCH. These results demonstrate that the DOT in TCHs
do not represent the DOT in CHs. In preparation for the development of SAARs in Japan, a
nationwide surveillance study is needed to specify the DOT in each antibiotic category accord-
ing to the following types of hospital for assessment of the AS program in each hospital: small-
sized CHs (e.g., < 300 beds) without an ICU, CHs with an ICU, TCHs, and teaching hospitals.
The DOT for curative care beds, excluding convalescent rehabilitative care beds, would be use-
ful for standardized risk-adjusted assessment in CHs.
The homogeneous use of a single class of broad-spectrum antibiotics leads to a rapid increase
in resistance. Historically, a rotating/cycling empirical antibiotic schedule [27–29] or antimicro-
bial mixing [26–28] was conducted to achieve the heterogeneous use of broad-spectrum antibiot-
ics in ICUs. Periodic antibiotic monitoring and supervision [23] to facilitate hospital-wide
heterogeneous antibiotic use was associated with a decreased rate of resistant gram-negative
organisms. The policy of equal use of intravenous broad-spectrum antibiotics (25% in each of the
four antibiotic classes) has been reported by several authors [23, 27–29], and the AHI was devel-
oped to evaluate whether AS programs achieve the goal of diversified antibiotic use [18, 22, 23].
In a nationwide survey in the US [26], the % DOT of intravenous fluoroquinolones was
approximately 23% among the four classes of intravenous broad-spectrum antibiotics. In con-
trast, the rate of fluoroquinolones among intravenous broad-spectrum antibiotics ranged from
12.4% to 15.4% in an AS program conducted in Japan [23]. Fluoroquinolones were used only
in 12.5% of patients with bacteremia caused by difficult-to-treat gram-negative bacilli treated
with broad-spectrum antibiotics in a Japanese hospital [30]. Recently, Ueda et al. [20] reported
that the % DOT values obtained in a rigorous 7-year AS program were 34.8% for carbapenems,
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 11 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
32.1% for piperacillin/tazobactam, 24.3% for fourth-generation cephalosporins/ceftazidime/
aztreonam, and 8.9% for intravenous fluoroquinolones. From these results, a modified AHI
for achieving a % DOT of 10% for fluoroquinolones and 30% for each of the remaining three
broad-spectrum antibiotic classes was proposed, and an increased modified AHI value resulted
in lower antibiotic resistant rates for P. aeruginosa and K. pneumoniae [20]. The significant
cutoff of the modified AHI to discriminate the risk of antibiotic resistance was 0.899 for K.
pneumoniae [20].
Contrary to expectations, the widespread use of broad-spectrum antibiotics for hospital-
onset infections did not result in poor antibiotic susceptibility of clinical isolates in the TCH.
Effective infection control practices [31] and the diversified use of broad-spectrum antibiotics
in the AS program may have prevented the emergence and spread of AMR in the TCH. Gan-
dra et al. [32] also found that overall AMR rates in TCHs were not significantly higher than
those in small CHs. De-escalation or a rule of conversion to other antibiotics that are effective
against the causative organism within 10 days in patients who require prolonged use of carba-
penems or piperacillin/tazobactam might facilitate the heterogeneous use of broad-spectrum
antibiotics with anti-Pseudomonas activity in the TCH. These results indicate that not only
quantity assessment of the DOT for broad-spectrum antibiotics but also quality assessment
using the AHIs are useful for evaluating AS programs.
After establishing the new AS team in the CH, which included infectious disease physicians
dedicated to the AS program, the DOT for broad-spectrum antibiotics decreased compared
with the DOT in the pre-establishment term. According to antibiotic use patterns in the initial
1 year (term 1) after establishing the new AS, piperacillin/tazobactam use was discouraged and
cefepime was recommended as an alternative in term 2. This policy balanced the use of these
broad-spectrum antibiotics within half a year. Antibiotic use was improved in a short period
with implementation of a wide range of interventions by the new AS team; this pattern may
characterize AS programs in CHs with smaller patient numbers than TCHs if the target goal is
clearly specified and rigorous AS activity is conducted to achieve the target.
There are several limitations to this study. First, this was a retrospective study comparing
only one institution of each type. Second, this study was conducted during a period with a
high prevalence of infections owing to severe acute respiratory syndrome coronavirus 2, which
might have affected antibiotic use in the study hospitals [33], especially the CH, which is one
of four designated medical institutions for specified infectious diseases in Japan. Finally, few
infectious disease physicians who are specialists certified by the Japanese Association of Infec-
tious Diseases are dedicated to AS programs in CHs. Hence, the DOT and the AHIs in this
study may not represent small- or mid-sized CHs.
In conclusion, significant differences in antibiotic use in each antibiotic category were
found between the CH and TCH in this study. However, increased broad-spectrum antibiotic
use did not cause higher resistance rates in the TCH than those in the CH, possibly because of
antibiotic diversity. To evaluate the effectiveness of AS programs, applying benchmarks of
antibiotic use according to facility type and hospital size are a promising approach.
Supporting information
S1 Table. The comparison of patients days in each department between Hyogo medical
university hospital and Tokoname city hospital.
(PPTX)
S2 Table. MIC breakpoints based on EUCAST and CLSI for Pseudomonas aeruginosa, Aci-
netobacter spp., and Enterobacteriaceae species.
(PPTX)
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 12 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
S3 Table. Day of therapy (DOT) throughout the study period (April 2021 to March 2022)
of each category of intravenous antimicrobial agent in the tertiary care hospital and the
community hospital.
(PPTX)
S4 Table. Rate of non-susceptibility among nosocomial isolates according to the Clinical &
Laboratory Standards Institute criteria between the tertiary hospital and the community
hospital.
(PPTX)
S5 Table. Reasons for intervention by antimicrobial stewardship team and adherence rate
by physicians between April 2022 and September 2022.
(PPTX)
S6 Table. Days of therapy (DOT) and relative DOT and antibiotic heterogeneity indices
(AHIs) for broad-spectrum antibiotics commonly used for hospital-onset infections on the
acute-phase medical wards in the community hospital.
(PPTX)
S1 Fig. Method of calculating antibiotic heterogeneity indices (AHIs).
(PPTX)
Author Contributions
Conceptualization: Makoto Ishii.
Data curation: Yoshio Takesue.
Formal analysis: Takashi Ueda, Yoshio Takesue.
Funding acquisition: Yoshio Takesue.
Investigation: Mika Morosawa, Takashi Ueda, Kazuhiko Nakajima, Tomoko Inoue, Masa-
nobu Toyama, Hitoshi Ogasiwa, Miki Doi, Yasuhiro Nozaki, Yasushi Murakami.
Methodology: Yoshio Takesue.
Project administration: Takashi Ueda, Yoshio Takesue.
Resources: Yoshio Takesue.
Software: Yoshio Takesue.
Supervision: Makoto Ishii.
Validation: Yoshio Takesue.
Visualization: Yoshio Takesue.
Writing – original draft: Mika Morosawa, Takashi Ueda, Yoshio Takesue.
Writing – review & editing: Mika Morosawa, Takashi Ueda, Yoshio Takesue.
References
1. Moriyama Y, Ishikane M, Kusama Y, Matsunaga N, Tajima T, Hayakawa K et al. Nationwide cross-sec-
tional study of antimicrobial stewardship and antifungal stewardship programs in inpatient settings in
Japan. BMC Infect Dis. 2021; 21: 355. https://doi.org/10.1186/s12879-021-06035-5 PMID: 33858346
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 13 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
2. Akpan MR, Isemin NU, Udoh AE, Ashiru-Oredope D. Implementation of antimicrobial stewardship pro-
grammes in African countries: a systematic literature review. J Glob Antimicrob Resist. 2020; 22: 317–
324. https://doi.org/10.1016/j.jgar.2020.03.009 PMID: 32247077
3. Nathwani D, Varghese D, Stephens J, Ansari W, Martin S, Charbonneau C. Value of hospital antimicro-
bial stewardship programs [ASPs]: a systematic review. Antimicrob Resist Infect Control. 2019; 8: 35.
https://doi.org/10.1186/s13756-019-0471-0 PMID: 30805182
4. Schuts EC, Hulscher MEJL, Mouton JW, Verduin CM, Stuart JWTC, Overdiek HWPM, et al. Current
evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lan-
cet Infect Dis. 2016; 16: 847–856. https://doi.org/10.1016/S1473-3099(16)00065-7 PMID: 26947617
5. Takesue Y, Ohge H, Sakashita M, Sudo T, Murakami Y, Uemura K, et al. Effect of antibiotic heteroge-
neity on the development of infections with antibiotic-resistant gram-negative organisms in a non-inten-
sive care unit surgical ward. World J Surg. 2006; 30: 1269–1276. https://doi.org/10.1007/s00268-005-
0781-7 PMID: 16705389
6. Barlam TF, Cosgrove SE, Abbo LM, MacDougall C, Schuetz AN, Septimus EJ, et al. Implementing an
antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Soci-
ety for Healthcare Epidemiology of America. Clin Infect Dis. 2016; 62: e51–e77. https://doi.org/10.1093/
cid/ciw118 PMID: 27080992
7. Kirk A, Pierce J, Doll M, Lee K, Pakyz A, Kim J et al. The effectiveness of formulary restriction and pre-
authorization at an academic medical center. Am J Infect Control. 2019; 47: 837–839. https://doi.org/
10.1016/j.ajic.2018.12.026 PMID: 30723027
8. Schweitzer VA, van Heijl I, Boersma WG, Rozemeijer W, Verduin K, Grootenboers MJ, et al. Narrow-
spectrum antibiotics for community-acquired pneumonia in Dutch adults (CAP-PACT): a cross-sec-
tional, stepped-wedge, cluster-randomised, non-inferiority, antimicrobial stewardship intervention trial.
Lancet Infect Dis. 2022; 22: 274–283.
9. Mehta JM, Haynes K, Wileyto EP, Gerber JS, Timko DR, Morgan SC, et al. Comparison of prior authori-
zation and prospective audit with feedback for antimicrobial stewardship. Infect Control Hosp Epidemiol.
2014; 35: 1092–1099. https://doi.org/10.1086/677624 PMID: 25111916
10. Honda H, Ohmagari N, Tokuda Y, Mattar C, Warren DK. Antimicrobial stewardship in inpatient settings
in the Asia Pacific region: a systematic review and meta-analysis. Clin Infect Dis. 2017; 64: S119–S126.
https://doi.org/10.1093/cid/cix017 PMID: 28475777
11. Mendez CM, Harrington DW, Christenson P, Spellberg B. Impact of hospital variables on case mix
index as a marker of disease severity. Popul Health Manag. 2014; 17: 28–34. https://doi.org/10.1089/
pop.2013.0002 PMID: 23965045
12. Dellit TH, Owens RC, McGowan JE Jr, Gerding DN, Weinstein RA, Burke JP, et al. Infectious Diseases
Society of America and the Society for Healthcare Epidemiology of America guidelines for developing
an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007; 44: 159–177.
https://doi.org/10.1086/510393 PMID: 17173212
13. van Santen KL, Edwards JR, Webb AK, Pollack LA, O’Leary E, Neuhauser MM, et al. The standardized
antimicrobial administration ratio: a new metric for measuring and comparing antibiotic use. Clin Infect
Dis. 2018; 67: 179–185. https://doi.org/10.1093/cid/ciy075 PMID: 29409000
14. Ruggles BM, Xiong A, Kyle B. Healthcare coverage in the US and Japan: a comparison. Nursing 2019;
49: 56–60. https://doi.org/10.1097/01.NURSE.0000553277.03472.d8 PMID: 30893207
15. Kim B, Ahn SV, Kim DS, Chae J, Jeong SJ, Uh Y, et al. Development of the Korean standardized antimi-
crobial aAdministration ratio as a tool for benchmarking antimicrobial use in each hospital. J Korean
Med Sci. 2022; 37: e191.
16. Plüss-Suard C.; Pannatier A.; Kronenberg A.; Mühlemann K.; Zanetti G. Impact of antibiotic use on car-
bapenem resistance in Pseudomonas aeruginosa: is there a role for antibiotic diversity? Antimicrob.
Agents Chemother. 2013, 57, 1709–1713. https://doi.org/10.1128/AAC.01348-12 PMID: 23357763
17. Brown E. M.; Nathwani D. Antibiotic cycling or rotation: a systematic review of the evidence of efficacy.
J. Antimicrob. Chemother. 2005, 55, 6–9. https://doi.org/10.1093/jac/dkh482 PMID: 15531594
18. Sandiumenge A, Lisboa T, Gomez F, Hernandez P, Canadell L, Rello J. Effect of antibiotic diversity on
ventilator-associated pneumonia caused by ESKAPE Organisms. Chest. 2011; 140: 643–651. https://
doi.org/10.1378/chest.11-0462 PMID: 21659436
19. Bal A. M.; Kumar A.; Gould I. M. Antibiotic heterogeneity: from concept to practice. Ann. N. Y. Acad.
Sci. 2010, 1213, 81–91. https://doi.org/10.1111/j.1749-6632.2010.05867.x PMID: 21175677
20. Ueda T, Takesue Y, Nakajima K, Ichiki K, Ishikawa K, Yamada K, et al. Correlation between Antimicro-
bial Resistance and the Hospital-Wide Diverse Use of Broad-Spectrum Antibiotics by the Antimicrobial
Stewardship Program in Japan. Pharmaceutics. 2023; 15(2):518. https://doi.org/10.3390/
pharmaceutics15020518 PMID: 36839839
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 14 / 15
PLOS ONE Antibiotic stewardship in a community and tertiary hospital
21. World health Organization: Cumulative overview of DDD. WHOCC—DDD alterations accessed 9
March 2023
22. Sandiumenge A, Diaz E, Rodriguez A, Vidaur L, Canadell L, Olona M, et al. Impact of diversity of antibi-
otic use on the development of antimicrobial resistance. Antimicrob Chemother. 2006; 57: 1197–1204.
https://doi.org/10.1093/jac/dkl097 PMID: 16565158
23. Takesue Y, Nakajima K, Ichiki K, Ishihara M, Wada Y, Takahashi Y, et al. Impact of a hospital-wide pro-
gramme of heterogeneous antibiotic use on the development of antibiotic-resistant Gram-negative bac-
teria. J Hosp Infect. 2010; 75: 28–32. https://doi.org/10.1016/j.jhin.2009.11.022 PMID: 20346536
24. European committee on antimicrobial susceptibility testing: The implementation of the new definition of
S, I, and R. EUCAST—Intermediate category—information for all accessed 9 March 2023
25. M100: Performance Standards for Antimicrobial Susceptibility Testing, 30th Edition [cited 13 October
2022]. Available from: (nih.org.pk).
26. Goodman KE, Cosgrove SE, Pineles L, Magder LS, Anderson DJ, Dodds Ashley E, et al. Significant
regional differences in antibiotic use across 576 US hospitals and 11 701 326 adult admissions, 2016–
2017. Clin Infect Dis. 2021; 73: 213–222. https://doi.org/10.1093/cid/ciaa570 PMID: 32421195
27. Raymond DP, Pelletier SJ, Crabtree TD, Gleason TG, Hamm LL, Pruett TL, et al. Impact of a rotating
empiric antibiotic schedule on infectious mortality in an intensive care unit. Crit Care Med. 2001; 29:
1101–1108. https://doi.org/10.1097/00003246-200106000-00001 PMID: 11395583
28. Cobos-Trigueros N, Sole´ M, Castro P, Torres JL, Rinaudo M, De Lazzari E, et al. Evaluation of a mixing
versus a cycling strategy of antibiotic use in critically-ill medical patients: impact on acquisition of resis-
tant microorganisms and clinical outcomes. PLoS One. 2016; 11: e0150274. https://doi.org/10.1371/
journal.pone.0150274 PMID: 26982807
29. Martınez JA, Nicolas JM, Marco F, Horcajada JP, Garcia-Segarra G, Trilla A, et al.: Comparison of anti-
microbial cycling and mixing strategies in two medical intensive care units. Crit Care Med. 2006; 34:
329–336. https://doi.org/10.1097/01.ccm.0000195010.63855.45 PMID: 16424711
30. Shime N, Kosaka T, Fujita N. De-escalation of antimicrobial therapy for bacteraemia due to difficult-to-
treat Gram-negative bacilli. Infection. 2013; 41: 203–210. https://doi.org/10.1007/s15010-012-0388-5
PMID: 23254646
31. Trick WE, Vernon MO, Welbel SF, Demarais P, Hayden MK, Weinstein RA et al. Multicenter interven-
tion program to increase adherence to hand hygiene recommendations and glove use and to reduce
the incidence of antimicrobial resistance. Infect Control Hosp Epidemiol. 2007; 28: 42–49. https://doi.
org/10.1086/510809 PMID: 17230386
32. Gandra S, Trett A, Klein EY, Laxminarayan R. Antimicrobial resistance a bigger problem in tertiary care
hospitals than in small community hospitals in the United States? Clin Infect Dis. 2017; 65:860–863.
33. Pierce J, Stevens MP. COVID-19 and antimicrobial stewardship: lessons learned, best practices, and
future implications. Int J Infect Dis. 2021; 113: 103–108. https://doi.org/10.1016/j.ijid.2021.10.001
PMID: 34624517
PLOS ONE | https://doi.org/10.1371/journal.pone.0284806 April 24, 2023 15 / 15
You might also like
- Mycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andDocument10 pagesMycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andc gNo ratings yet
- Act 1 Manamparan Hosny M.Document8 pagesAct 1 Manamparan Hosny M.Gizelle Mae Pasiol-Macayan100% (2)
- Jac-Antimicrobial ResistanceDocument10 pagesJac-Antimicrobial ResistancenovatuschingoroNo ratings yet
- The Impact of Stewardship Programmes On Antibiotic Consumption PatternsDocument20 pagesThe Impact of Stewardship Programmes On Antibiotic Consumption PatternsRaphael AmponsahNo ratings yet
- NouwenDocument2 pagesNouwenmarkinceNo ratings yet
- Jurnal Mikfar Utari 2-1Document10 pagesJurnal Mikfar Utari 2-1Azri Aprisonia SaritaNo ratings yet
- Ab Round StewardshipDocument7 pagesAb Round StewardshipbpinsaniNo ratings yet
- Evaluation of a clinical pharmacist-led antimicrobial stewardship program in a neurosurgical intensive care unit: a pre-and post-intervention cohort studyDocument10 pagesEvaluation of a clinical pharmacist-led antimicrobial stewardship program in a neurosurgical intensive care unit: a pre-and post-intervention cohort studyf2b9b25kb9No ratings yet
- Antimicrobial StewardshipDocument7 pagesAntimicrobial StewardshipJohn TusselNo ratings yet
- ProkalsitoninDocument11 pagesProkalsitoninFarmasi RSUD Kramat JatiNo ratings yet
- Antibiotics 11 00074Document10 pagesAntibiotics 11 00074fahira amandaNo ratings yet
- Development of A Multiplex Droplet Digital PCR Method For Detection and Monitoring of Mycobacterium Tuberculosis and Drug-Resistant TuberculosisDocument9 pagesDevelopment of A Multiplex Droplet Digital PCR Method For Detection and Monitoring of Mycobacterium Tuberculosis and Drug-Resistant Tuberculosisd4rkgr455No ratings yet
- Interprofessional CollaboratioDocument16 pagesInterprofessional CollaboratioAnggito AbimanyuNo ratings yet
- 6759 25186 1 PBDocument8 pages6759 25186 1 PBPatricio LimaNo ratings yet
- Chaudhari 2013Document4 pagesChaudhari 2013WahyunitadotokaNo ratings yet
- Antibiotic 02Document4 pagesAntibiotic 02Arslan ShahNo ratings yet
- Evaluation of Outpatient Antibiotic Use in Beijing General Hospitals in 2015Document9 pagesEvaluation of Outpatient Antibiotic Use in Beijing General Hospitals in 2015UdtjeVanDerJeykNo ratings yet
- Journal of Infection: SciencedirectDocument8 pagesJournal of Infection: SciencedirectKarina Dwi SwastikaNo ratings yet
- 44 2 159Document19 pages44 2 159Nicole MariaNo ratings yet
- The Time Varying Association Between Previous Anti - 2023 - Clinical MicrobiologDocument4 pagesThe Time Varying Association Between Previous Anti - 2023 - Clinical MicrobiologAnnisa SetyantiNo ratings yet
- ProkalsitoninDocument9 pagesProkalsitoninAndhika HamdanyNo ratings yet
- Point Prevalence Study of Antibiotics Use in Paediatric Wards of A Tertiary Health Facility in Kaduna NigeriaDocument8 pagesPoint Prevalence Study of Antibiotics Use in Paediatric Wards of A Tertiary Health Facility in Kaduna NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clin Infect Dis.-2007-Dellit-159-77Document19 pagesClin Infect Dis.-2007-Dellit-159-77Melo PerezNo ratings yet
- Thu 2012Document5 pagesThu 2012Nadila Hermawan PutriNo ratings yet
- Antibiotics 11 00791 v2Document16 pagesAntibiotics 11 00791 v2Retno WahyuningrumNo ratings yet
- Procalcitonin and AB DecisionsDocument10 pagesProcalcitonin and AB DecisionsDennysson CorreiaNo ratings yet
- SHEA Position Paper: I C H EDocument17 pagesSHEA Position Paper: I C H EIFRS SimoNo ratings yet
- Antibiotics 11 01033 v4Document14 pagesAntibiotics 11 01033 v4Hana AoiNo ratings yet
- 1 s2.0 S2213398421002529 MainDocument5 pages1 s2.0 S2213398421002529 MainZulfkar Latief QadrieNo ratings yet
- Antimicrobial Stewardship: Attempting To Preserve A Strategic ResourceDocument7 pagesAntimicrobial Stewardship: Attempting To Preserve A Strategic Resourcem1k0eNo ratings yet
- HTTP DX Doi Org 10 1017 S0950268811002214Document9 pagesHTTP DX Doi Org 10 1017 S0950268811002214Alvaro SDNNo ratings yet
- Antimicrobial Stewardship in The Intensive Care Unit, 2023Document10 pagesAntimicrobial Stewardship in The Intensive Care Unit, 2023Jonathan Fierro MedinaNo ratings yet
- Jiaa 221Document13 pagesJiaa 221AndradaLavricNo ratings yet
- Importance of Infection Control PracticesDocument5 pagesImportance of Infection Control Practicesapi-3760696No ratings yet
- Knowledge, Attitude and Practice of Antibiotics Resistance: A Questionnaire Study Among Ug and PG Medical StudentsDocument10 pagesKnowledge, Attitude and Practice of Antibiotics Resistance: A Questionnaire Study Among Ug and PG Medical StudentsIJAR JOURNALNo ratings yet
- Title: Improvement in The Appropriate Antimicrobial Usage For Treating PediatricDocument23 pagesTitle: Improvement in The Appropriate Antimicrobial Usage For Treating PediatricSofia Marie GalendezNo ratings yet
- 30-Day Readmission, Antibiotics Costs and Costs of Delay To Adequate Treatment of Enterobacteriaceae UTI, Pneumonia, and SepsisDocument7 pages30-Day Readmission, Antibiotics Costs and Costs of Delay To Adequate Treatment of Enterobacteriaceae UTI, Pneumonia, and SepsisMorris Lintong BarimbingNo ratings yet
- Longitudinal Clinical Evaluation of Antibiotic Use Among Patients With InfectionDocument11 pagesLongitudinal Clinical Evaluation of Antibiotic Use Among Patients With InfectionMITA RESTINIA UINJKTNo ratings yet
- Palliative Care Infections and Antibiotic Cost: A Vicious CircleDocument12 pagesPalliative Care Infections and Antibiotic Cost: A Vicious CircleRahmanu ReztaputraNo ratings yet
- Antibiotics' Use in Thailand: Community Pharmacists' Knowledge, Attitudes and PracticesDocument13 pagesAntibiotics' Use in Thailand: Community Pharmacists' Knowledge, Attitudes and PracticesBudh SiltrakoolNo ratings yet
- SISTEMATIC REVIEW - I Nyoman Triaditya Kresna Putra - 71225050 - 10b.id - enDocument19 pagesSISTEMATIC REVIEW - I Nyoman Triaditya Kresna Putra - 71225050 - 10b.id - enTriaditya KresnaNo ratings yet
- Antibiotico en SepsisDocument13 pagesAntibiotico en Sepsismaomed2014No ratings yet
- Antimicrobial ResistanceDocument11 pagesAntimicrobial Resistanceapi-253312159No ratings yet
- Antibiotic in PicuDocument4 pagesAntibiotic in PicuVickha Dian HapsariNo ratings yet
- Im 2022Document10 pagesIm 2022YogiHadityaNo ratings yet
- Antibiotecoterapia en SepsisDocument13 pagesAntibiotecoterapia en SepsisJuan Pablo Arteaga VargasNo ratings yet
- Effect of Procalcitonin-Guided AntibioticDocument11 pagesEffect of Procalcitonin-Guided AntibioticRaul ContrerasNo ratings yet
- Proposal Powerpoint Rev 2Document24 pagesProposal Powerpoint Rev 2Ma. Luisa BuotNo ratings yet
- 2019 Fauna Ajpcr 12 8Document4 pages2019 Fauna Ajpcr 12 8Fawan HaidirNo ratings yet
- 2019 Fauna Ajpcr 12 8Document4 pages2019 Fauna Ajpcr 12 8Fawan HaidirNo ratings yet
- 2019 Fauna Ajpcr 12 8Document4 pages2019 Fauna Ajpcr 12 8Fawan HaidirNo ratings yet
- Antibiotics 11 00022Document16 pagesAntibiotics 11 00022Putri RamadhaniNo ratings yet
- s13054 023 04626 ZDocument8 pagess13054 023 04626 ZDipendra PoudelNo ratings yet
- Rab 6Document11 pagesRab 6Belia DestamaNo ratings yet
- The Antibiogram Key Considerations For Its DevelopmentDocument6 pagesThe Antibiogram Key Considerations For Its DevelopmentrehanaNo ratings yet
- Principi 2016Document8 pagesPrincipi 2016RaffaharianggaraNo ratings yet
- CC 9062Document9 pagesCC 9062Javed AkhtarNo ratings yet
- Assessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesDocument9 pagesAssessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesAl ANo ratings yet
- Golden Hour CCM Arthur Van Zanten IC1Document3 pagesGolden Hour CCM Arthur Van Zanten IC1Sara NicholsNo ratings yet
- 1 s2.0 S1198743X14621649 MainDocument10 pages1 s2.0 S1198743X14621649 MainMohamed SakrNo ratings yet
- Drug Interactions in Infectious Diseases: Mechanisms and Models of Drug InteractionsFrom EverandDrug Interactions in Infectious Diseases: Mechanisms and Models of Drug InteractionsManjunath P. PaiNo ratings yet
- Articulo 16 PGDocument9 pagesArticulo 16 PGCarol RuizNo ratings yet
- Articulo 12 PGDocument8 pagesArticulo 12 PGCarol RuizNo ratings yet
- Articulo 17 PGDocument10 pagesArticulo 17 PGCarol RuizNo ratings yet
- Articulo 11 PGDocument9 pagesArticulo 11 PGCarol RuizNo ratings yet
- Articulo 10 PGDocument11 pagesArticulo 10 PGCarol RuizNo ratings yet
- WHO TootlkitDocument88 pagesWHO TootlkitVivek BasnetNo ratings yet
- CV - Ashley L LoganDocument6 pagesCV - Ashley L Loganapi-536775958No ratings yet
- 2020 MUSE Conference - Sessions - March 6 2020Document73 pages2020 MUSE Conference - Sessions - March 6 2020Michele LambertNo ratings yet
- Infection Control in Pharmacy ServicesDocument30 pagesInfection Control in Pharmacy ServicesAmeng GosimNo ratings yet
- Antibiotic Usage in Common and Uncommon Infection in Primary Care Setting - Daerah RompinDocument91 pagesAntibiotic Usage in Common and Uncommon Infection in Primary Care Setting - Daerah RompinMonysyha AtriNo ratings yet
- Lecture 12, Introduction To Public Health.Document18 pagesLecture 12, Introduction To Public Health.Katerina BagashviliNo ratings yet
- BookletDocument14 pagesBookletIndra KelanaNo ratings yet
- Jac-Antimicrobial ResistanceDocument7 pagesJac-Antimicrobial ResistanceKarla HernandezNo ratings yet
- Antimicrobial Stewardship in NICU - Mulya Rahma Karyanti-1Document53 pagesAntimicrobial Stewardship in NICU - Mulya Rahma Karyanti-1Enny AndrianiNo ratings yet
- Program at GlanceDocument5 pagesProgram at GlanceAlvarock MunRenoNo ratings yet
- 2023 PREFINALS - Improving PH Thru PharmacyDocument141 pages2023 PREFINALS - Improving PH Thru PharmacyAnthony PamolinoNo ratings yet
- MOH-National Antimicrobial GuidelinesDocument65 pagesMOH-National Antimicrobial GuidelinesHamada Hassan AlloqNo ratings yet
- Woundcon Fall 2021 Syllabus and Exhibitor GuideDocument25 pagesWoundcon Fall 2021 Syllabus and Exhibitor GuidePeter KhanhNo ratings yet
- Introduction:-: Ambulatory Healthcare Organizations IntroducedDocument7 pagesIntroduction:-: Ambulatory Healthcare Organizations Introducedanimesh pandaNo ratings yet
- Form Evaluaso AmsDocument1 pageForm Evaluaso AmsNadial uzmahNo ratings yet
- Global Contributions of Pharmacists During The COVID-19 PandemicDocument13 pagesGlobal Contributions of Pharmacists During The COVID-19 PandemicSILVIA ROSARIO CHALCO MENDOZANo ratings yet
- EAU Guidelines Urological Infections 2016 1 PDFDocument16 pagesEAU Guidelines Urological Infections 2016 1 PDFMaria Jose Zamorano SepulvedaNo ratings yet
- Antibiotic Stewardship in Neonatal SepsisDocument41 pagesAntibiotic Stewardship in Neonatal SepsisyusahanaNo ratings yet
- Webinar 10 12 17 PDFDocument73 pagesWebinar 10 12 17 PDFDanielaGarciaNo ratings yet
- Netcare-SA-ops-Quality-and-Clinical-Gov 2023-04-15 08 - 22 - 54Document10 pagesNetcare-SA-ops-Quality-and-Clinical-Gov 2023-04-15 08 - 22 - 54Shuaib KauchaliNo ratings yet
- RITM ORG CHART - As of May 2017Document6 pagesRITM ORG CHART - As of May 2017Daryl De VeraNo ratings yet
- FICCI India Medical Device ReportDocument80 pagesFICCI India Medical Device ReportGulshan Chhibber100% (1)
- Perceptions and Current Practices of Community Pharmacists Regarding Antimicrobial Stewardship in TasmaniaDocument8 pagesPerceptions and Current Practices of Community Pharmacists Regarding Antimicrobial Stewardship in Tasmaniafarooq shikhNo ratings yet
- Code of Practice 280715 AccDocument98 pagesCode of Practice 280715 AccAdriana MihalachiNo ratings yet
- Ebffiledoc - 31download PDF Practical Clinical Microbiology and Infectious Diseases A Hands On Guide First Edition Gronthoud Ebook Full ChapterDocument53 pagesEbffiledoc - 31download PDF Practical Clinical Microbiology and Infectious Diseases A Hands On Guide First Edition Gronthoud Ebook Full Chaptermary.browne374100% (2)
- Henson 2019Document5 pagesHenson 2019Edimar Joshua FrialaNo ratings yet
- Gilead 7th HIV Summi AgendaDocument8 pagesGilead 7th HIV Summi Agendaayaks uuNo ratings yet
- RASPRODocument36 pagesRASPROVera Yulianti100% (2)
- Oxford - Blood CultureDocument8 pagesOxford - Blood CultureKhoa Vi Sinh BVCRNo ratings yet