Download as pdf or txt
You might also like
- ATLSPracticeTest2 With AnswersDocument10 pagesATLSPracticeTest2 With Answersemad mohamed100% (1)
- A New General Catalogue of The Ants of The WorldDocument513 pagesA New General Catalogue of The Ants of The WorldFabiana Soares Cariri Lopes100% (1)
- Michael Friedman, MD, Vytenis Grybauskas, MD, David Chang, MDDocument4 pagesMichael Friedman, MD, Vytenis Grybauskas, MD, David Chang, MDConstantin StanNo ratings yet
- The Anatomy Basis of PIADocument7 pagesThe Anatomy Basis of PIAyeapdshengNo ratings yet
- Ann Burns and Fire Disasters 29 209Document6 pagesAnn Burns and Fire Disasters 29 209fabian hernandez medinaNo ratings yet
- Visweswar Bhattacharya, Rajesh Kumar WattsDocument6 pagesVisweswar Bhattacharya, Rajesh Kumar WattsViswanath_Poli_2693No ratings yet
- Sural BistaDocument6 pagesSural BistaAzmi FarhadiNo ratings yet
- Pec MajorDocument6 pagesPec MajorUsama SaeedNo ratings yet
- Masquelet 1984Document6 pagesMasquelet 1984Hương HuỳnhNo ratings yet
- Superiorly Based Perforator Plus FL Ap For Inguinal Defects: Original ArticleDocument5 pagesSuperiorly Based Perforator Plus FL Ap For Inguinal Defects: Original ArticleamdreyNo ratings yet
- The Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic ReconstrDocument8 pagesThe Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic Reconstrydk sinhNo ratings yet
- Temproal FlapDocument7 pagesTemproal FlapMarko LazicNo ratings yet
- Lateral Thigh and Anterolateral Thigh Free Tissue Transfer: Background, History of The Procedure, IndicationsDocument12 pagesLateral Thigh and Anterolateral Thigh Free Tissue Transfer: Background, History of The Procedure, IndicationsNaenay WannatrakoolNo ratings yet
- Component Separation Technique To Repair Large Midline HerniasDocument10 pagesComponent Separation Technique To Repair Large Midline HerniasOhana S.No ratings yet
- Use of Reverse Lateral Arm Flap For Coverage of Elbow in Burn PatientsDocument3 pagesUse of Reverse Lateral Arm Flap For Coverage of Elbow in Burn PatientsPalwasha MalikNo ratings yet
- Application of Extende D Bi-Pedicle Anterolateral Thigh Free Flaps For Reconstruction of Large Defects - A Case SeriesDocument8 pagesApplication of Extende D Bi-Pedicle Anterolateral Thigh Free Flaps For Reconstruction of Large Defects - A Case Seriescusom34No ratings yet
- Anatomical Basis of The Posterior Brachial Skin Flap: SummaryDocument6 pagesAnatomical Basis of The Posterior Brachial Skin Flap: Summarycusom34No ratings yet
- Cutaneous Perforators and Their Clinical ImplicatiDocument12 pagesCutaneous Perforators and Their Clinical Implicatinidhal.mahdhiNo ratings yet
- First Dorsal Metacarpal Artery Flap For Thumb Reconstruction: A Retrospective Clinical StudyDocument7 pagesFirst Dorsal Metacarpal Artery Flap For Thumb Reconstruction: A Retrospective Clinical StudyAry YounusNo ratings yet
- Jena 2015Document3 pagesJena 2015amdreyNo ratings yet
- Rsa FlapDocument11 pagesRsa Flapdhivya kannanNo ratings yet
- 19 25 1 SMDocument2 pages19 25 1 SMrnvisNo ratings yet
- Burger Et Al 2002 Abdominal Incisions Techniques and Postoperative ComplicationsDocument7 pagesBurger Et Al 2002 Abdominal Incisions Techniques and Postoperative ComplicationsagengbsNo ratings yet
- Injury: Xu Gong, Jian Li Cui, Lai Jin LuDocument4 pagesInjury: Xu Gong, Jian Li Cui, Lai Jin LuPalwasha MalikNo ratings yet
- Indicaciones Colgajo Inguinal MusloDocument10 pagesIndicaciones Colgajo Inguinal MusloMATTHEWS1No ratings yet
- Temporal Bone Resection: Brian Ho, MD, C. Arturo Solares, MD, FACS, Benedict Panizza, MBBS, MBA, FRACSDocument5 pagesTemporal Bone Resection: Brian Ho, MD, C. Arturo Solares, MD, FACS, Benedict Panizza, MBBS, MBA, FRACSAyuAnatrieraNo ratings yet
- Articles Related To Submental FlapDocument8 pagesArticles Related To Submental FlapDipti PatilNo ratings yet
- Biomechanical and Anatomical Consequences of Carpal Tunnel ReleaseDocument9 pagesBiomechanical and Anatomical Consequences of Carpal Tunnel ReleaseSylvia GraceNo ratings yet
- Reconstruction of The Skin Defect of The Knee Using A Reverse Anterolateral Thigh Island FlapDocument4 pagesReconstruction of The Skin Defect of The Knee Using A Reverse Anterolateral Thigh Island FlapAndrea Del VillarNo ratings yet
- Akhtar 2014Document7 pagesAkhtar 2014amdreyNo ratings yet
- 1 s2.0 S2352587814000060 MainDocument5 pages1 s2.0 S2352587814000060 MainjikhNo ratings yet
- 1 s2.0 S0002961004004295 MainDocument6 pages1 s2.0 S0002961004004295 MainResidentes CirugíaNo ratings yet
- 1 - Thoracic Surgery - Not As Difficult As It Seems - FINALDocument15 pages1 - Thoracic Surgery - Not As Difficult As It Seems - FINALKatarina SimicicNo ratings yet
- Chimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Document10 pagesChimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Manny TrujilloNo ratings yet
- Deltopectoral FlapDocument10 pagesDeltopectoral FlapAdit Wendy YRNo ratings yet
- Medial Plantar Flap For Hand ReconstructionDocument7 pagesMedial Plantar Flap For Hand ReconstructionMiguel JohnsonNo ratings yet
- Pia Flap - PhasDocument23 pagesPia Flap - PhasMoiz AliNo ratings yet
- Bases Anatomicas PerforantesDocument12 pagesBases Anatomicas PerforantesAngela GarciaNo ratings yet
- 05 CastelnuovoDocument7 pages05 Castelnuovogabriele1977No ratings yet
- Winter2019 PDFDocument7 pagesWinter2019 PDFAulida Arum MNo ratings yet
- Intracranial Anatomical Triangles A ComprehensiveDocument17 pagesIntracranial Anatomical Triangles A ComprehensiveYusuf BrilliantNo ratings yet
- 2015 AltDocument11 pages2015 Altplay259No ratings yet
- Robertson2008 231106 161521Document8 pagesRobertson2008 231106 161521Cristian SanchezNo ratings yet
- CapituloDocument16 pagesCapitulomaxilohgugmNo ratings yet
- Sabapathy 2014Document15 pagesSabapathy 2014Trina ViskhawatNo ratings yet
- DownloadDocument18 pagesDownloadhasan nazzalNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- The Plastysma Myocutaneous F Lap: Dale A. Baur, DDS, MDDocument6 pagesThe Plastysma Myocutaneous F Lap: Dale A. Baur, DDS, MDlaljadeff12No ratings yet
- Endoscopic Third VentriculostomyDocument4 pagesEndoscopic Third VentriculostomyMohamed Farouk El-FaresyNo ratings yet
- Sural Island Flap - A Good Option For Coverage of The Exposed Heel (Tendo-Achillis)Document6 pagesSural Island Flap - A Good Option For Coverage of The Exposed Heel (Tendo-Achillis)yennysabriniNo ratings yet
- Cucci Linfedema Generalidades AnatomiaDocument8 pagesCucci Linfedema Generalidades AnatomiaFeña Peña GonzalezNo ratings yet
- Archfaci 5 2 197Document5 pagesArchfaci 5 2 197Mugdha FrancisNo ratings yet
- Clinical StudyDocument6 pagesClinical StudyHendra JurbonNo ratings yet
- Double-Pedicle Propeller Flap For Reconstruction of The Foot and Ankle: Anatomical Study and Clinical ApplicationsDocument12 pagesDouble-Pedicle Propeller Flap For Reconstruction of The Foot and Ankle: Anatomical Study and Clinical ApplicationsWulan PurnamiNo ratings yet
- Distally BasedsuperficialDocument7 pagesDistally BasedsuperficialyennysabriniNo ratings yet
- Author 'S Accepted ManuscriptDocument20 pagesAuthor 'S Accepted ManuscriptMashood AhmedNo ratings yet
- Transnasal Prelacrimal Approach To The Inferior Intraconal Space: A Feasibility StudyDocument6 pagesTransnasal Prelacrimal Approach To The Inferior Intraconal Space: A Feasibility Studythanh nguyenNo ratings yet
- Radial Forearm Flap: DR G Avinash Rao Fellow Hand and Microsurgery Skims, SrinagarDocument71 pagesRadial Forearm Flap: DR G Avinash Rao Fellow Hand and Microsurgery Skims, Srinagaravinashrao39No ratings yet
- Scitemed Imj 2017 00036-1Document4 pagesScitemed Imj 2017 00036-1bernicemerryNo ratings yet
- Microsurgical Anatomy Brainstem Safe Entry Zones, Jns 2016Document18 pagesMicrosurgical Anatomy Brainstem Safe Entry Zones, Jns 2016Andrés SeguraNo ratings yet
- Posterior Interosseous Artery Flap For Hand Defects: Original ArticleDocument3 pagesPosterior Interosseous Artery Flap For Hand Defects: Original ArticleKristina DewiNo ratings yet
- Flik Silverpen's Guide ToDocument9 pagesFlik Silverpen's Guide ToSonny3091100% (1)
- Precolumn Fmoc HistamineDocument7 pagesPrecolumn Fmoc HistamineLaura MarcelaNo ratings yet
- Acfrogbpct50utxi Ygf7nagcrvxsznh4jb9pxe5obiap5r9akhldg Tsatlrg6rqvztj 6to3p1cshsnpir568ly7efdd4 Eqryh8b7xshanq4pkq2vkbx-Svf0muql5xenzr4dcjfqxrowi2omDocument58 pagesAcfrogbpct50utxi Ygf7nagcrvxsznh4jb9pxe5obiap5r9akhldg Tsatlrg6rqvztj 6to3p1cshsnpir568ly7efdd4 Eqryh8b7xshanq4pkq2vkbx-Svf0muql5xenzr4dcjfqxrowi2omyebadem228No ratings yet
- MKT 344 EcopreneurshipDocument17 pagesMKT 344 EcopreneurshipMd IrfanNo ratings yet
- BT BrinjalDocument10 pagesBT Brinjallalit krupal67% (3)
- Cementum in Disease - PerioDocument50 pagesCementum in Disease - PerioPoojan ThakoreNo ratings yet
- Guidelines 2.0Document4 pagesGuidelines 2.0Hansel TayongNo ratings yet
- Master Your Research Skills A Practical IEP Approach GuideDocument45 pagesMaster Your Research Skills A Practical IEP Approach GuideSandeep SpNo ratings yet
- All India Institute of Medical Sciences Nagpur Department of Obstetrics and GynecologyDocument19 pagesAll India Institute of Medical Sciences Nagpur Department of Obstetrics and GynecologySugan GavaskarNo ratings yet
- Effect of Phytochemical Constituents of Argemone Mexicana Leaf ExtractDocument6 pagesEffect of Phytochemical Constituents of Argemone Mexicana Leaf ExtractIJRASETPublicationsNo ratings yet
- Science Quarter 1 Module 4 PDFDocument40 pagesScience Quarter 1 Module 4 PDFshang121182% (11)
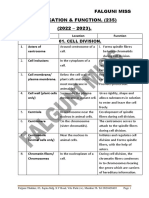
- X Bio Masterkey Location & Function 23 - 24Document28 pagesX Bio Masterkey Location & Function 23 - 24chaitanya100% (3)
- The Champion Text Book On Embalming 1908Document712 pagesThe Champion Text Book On Embalming 1908Ocean100% (3)
- Price Needs Updating, Should We Call The Police?: C M Bleakley, P Glasgow, D C MacauleyDocument2 pagesPrice Needs Updating, Should We Call The Police?: C M Bleakley, P Glasgow, D C MacauleyAna BelchiorNo ratings yet
- Clinical and Basic Immunodermatology 2017Document889 pagesClinical and Basic Immunodermatology 2017Angelo BaezaNo ratings yet
- 04.concept of Plant DiseaseDocument34 pages04.concept of Plant DiseaseLei Ann PunlaNo ratings yet
- AP Catalase Enzyme LabDocument4 pagesAP Catalase Enzyme LabAesthetic LoverNo ratings yet
- 2012 Penstate Nutrition Workshop ProceedingsDocument119 pages2012 Penstate Nutrition Workshop ProceedingsEuler RabeloNo ratings yet
- Instruments Suk2023Document76 pagesInstruments Suk2023chakshu chaudhryNo ratings yet
- CBE658 - Lab Report On Food PreservationDocument23 pagesCBE658 - Lab Report On Food PreservationGua HantuNo ratings yet
- Chapter 19Document61 pagesChapter 19Michelle Dela CruzNo ratings yet
- 96-117+Grima+2023+Article +paper-2Document22 pages96-117+Grima+2023+Article +paper-2Girma TimerNo ratings yet
- 9700 s13 Ms 21Document8 pages9700 s13 Ms 21Muhammad ShahzebNo ratings yet
- Personalized Medicine in BrazilDocument17 pagesPersonalized Medicine in BrazilJuan AraújoNo ratings yet
- Natural ResourcesDocument11 pagesNatural ResourcesBhavesh BhoeeNo ratings yet
- Os 3Document11 pagesOs 3مرتضى محمد فاضل جرجوكNo ratings yet
- Circuit TheoryDocument12 pagesCircuit TheoryHarshalNo ratings yet
- Pollen TestDocument8 pagesPollen TestnugrahaNo ratings yet