Download as pdf or txt
You might also like
- Caars Self L Int1Document9 pagesCaars Self L Int1Mona Refaei100% (2)
- Maternal Anatomy WilliamsDocument60 pagesMaternal Anatomy WilliamsZari Novela100% (2)
- Abdomen (Inguinal Hernia) : Anatomy II Block 3 NotesDocument39 pagesAbdomen (Inguinal Hernia) : Anatomy II Block 3 NotesJoseph KimNo ratings yet
- Ma. Elizabeth F. FontanillaDocument48 pagesMa. Elizabeth F. Fontanillatam mei100% (1)
- 15 Top Exercises To Increase HeightDocument1 page15 Top Exercises To Increase Heightnag_akNo ratings yet
- Jane Dunlap - Exploring Inner Space - Personal Experiences Under LSD-25 PDFDocument224 pagesJane Dunlap - Exploring Inner Space - Personal Experiences Under LSD-25 PDFJimy Robayo100% (1)
- Inguinal Canal: DR - Lubna NazliDocument28 pagesInguinal Canal: DR - Lubna NazliAhmed AminNo ratings yet
- Abdominal Wall and HerniaDocument35 pagesAbdominal Wall and HerniaMohammad BanisalmanNo ratings yet
- Anatomy of GIT For PCII Students..Document106 pagesAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNo ratings yet
- Anterior Abdominal Wall& Inguinal Canal 2023Document26 pagesAnterior Abdominal Wall& Inguinal Canal 2023GanapathyGaneshNo ratings yet
- Sahitya Snigdha (Hernia Module)Document159 pagesSahitya Snigdha (Hernia Module)h9pkyd9dg9No ratings yet
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDocument79 pagesSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNo ratings yet
- GIT Cont 071628Document51 pagesGIT Cont 071628Olatomide OlaniranNo ratings yet
- Lo 4Document7 pagesLo 4api-3803109No ratings yet
- The Large IntestineDocument34 pagesThe Large IntestineSastiy MutiadesieNo ratings yet
- Anatomy & Physiology of Anal Canal: Dr. Nadan KandelDocument29 pagesAnatomy & Physiology of Anal Canal: Dr. Nadan Kandelजीवनशैलीव्यवस्थापनकार्यक्रम रवि पाँचथरNo ratings yet
- Dinding Abdomen PSIKDocument79 pagesDinding Abdomen PSIKSondang DamanikNo ratings yet
- Maternal Anatomy ReportDocument52 pagesMaternal Anatomy Reportlovelots1234No ratings yet
- 2 Inguinal Region DiyaDocument31 pages2 Inguinal Region DiyaOmotosho DavidNo ratings yet
- Anatomy of The AbdomenDocument107 pagesAnatomy of The AbdomenmichaelhossianNo ratings yet
- Perineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, SpogDocument16 pagesPerineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, Spogpuskesmas gebangNo ratings yet
- Abdominal WallDocument60 pagesAbdominal WallthinzarNo ratings yet
- Anatomy of The Abdomen: Samara University Biomedical Sciences DepartmentDocument142 pagesAnatomy of The Abdomen: Samara University Biomedical Sciences Departmentfentaw melkieNo ratings yet
- Hernia: RSST Klaten Koas Stase Bedah A13.1Document54 pagesHernia: RSST Klaten Koas Stase Bedah A13.1Bagus WirayudaNo ratings yet
- Inguinal Hernias: Trix M. Asuncion M.D. General SurgeryDocument55 pagesInguinal Hernias: Trix M. Asuncion M.D. General Surgeryjitendra magarNo ratings yet
- PERINEUMDocument24 pagesPERINEUMmhr27112002No ratings yet
- Key PointsDocument34 pagesKey PointsSe YunNo ratings yet
- External & Internal Generative Organs OrgansDocument78 pagesExternal & Internal Generative Organs OrgansdeevoncNo ratings yet
- Hernia: Dr. NachmanyDocument69 pagesHernia: Dr. NachmanyDvir AviramNo ratings yet
- General AnatomyDocument46 pagesGeneral AnatomyIhab IsmailNo ratings yet
- Abdomen Dan PelvisDocument64 pagesAbdomen Dan PelvisRachmad RasidinNo ratings yet
- Anal CanalDocument59 pagesAnal CanalLulu ShukkoorNo ratings yet
- HerniaDocument46 pagesHerniaZubairkhan SuraniNo ratings yet
- Anatomy of The Anterior Abdominal Wall Part II: Lecture - 2Document34 pagesAnatomy of The Anterior Abdominal Wall Part II: Lecture - 2Ahmed OudahNo ratings yet
- 01 Anatomy of Female Genital System DR - OsmaDocument69 pages01 Anatomy of Female Genital System DR - OsmaAyalewNo ratings yet
- Hernia FTDDocument71 pagesHernia FTDEmmanuel Papa AcquahNo ratings yet
- Abdominal WallDocument75 pagesAbdominal WallJojo RyelciusNo ratings yet
- Inguinal Canal: Medial One-Half of The Inguinal Ligament Also Known As Poupart LigamentDocument4 pagesInguinal Canal: Medial One-Half of The Inguinal Ligament Also Known As Poupart LigamentDivya RanasariaNo ratings yet
- Perineal Tear: Presented by - Mayuri Zanwar Guided By-Dr. Sheetal Ma'AmDocument20 pagesPerineal Tear: Presented by - Mayuri Zanwar Guided By-Dr. Sheetal Ma'Ammayuri zanwarNo ratings yet
- Maternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ADocument115 pagesMaternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ANicole Alexandra KhoNo ratings yet
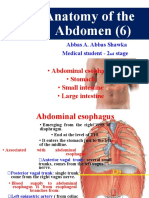
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Perineal TearsDocument49 pagesPerineal TearsvisakhaNo ratings yet
- Abdomen and Abdominal WallDocument40 pagesAbdomen and Abdominal WallAlex ChagalaNo ratings yet
- Digestive SystemDocument64 pagesDigestive SystemAyro Business CenterNo ratings yet
- Physio OB Maternal Anatomy External and Internal Generative Organs PPT 2Document67 pagesPhysio OB Maternal Anatomy External and Internal Generative Organs PPT 2Janine SergioNo ratings yet
- Anatomi PelvisDocument44 pagesAnatomi Pelvisari naNo ratings yet
- 2019 Hernia Kuliah FKDocument50 pages2019 Hernia Kuliah FKKhairani NurhamidahNo ratings yet
- Inguinal Canal and ScrotumDocument55 pagesInguinal Canal and ScrotumAuza Moses IbrahimNo ratings yet
- Hernia: DR - Surender Singh DhankharDocument36 pagesHernia: DR - Surender Singh DhankharBharat BhushanNo ratings yet
- Hernia: Done by D1 GroupDocument47 pagesHernia: Done by D1 Groupanindyadputri100% (1)
- Anatomy Block 3Document16 pagesAnatomy Block 3Eslie NájeraNo ratings yet
- 2 Ureter, Urinary Bladder and Urethra XJGDocument51 pages2 Ureter, Urinary Bladder and Urethra XJGwcbkk4vt9fNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Anatomy of The Abdomen (1) : - IntroductionDocument21 pagesAnatomy of The Abdomen (1) : - IntroductionMunachande KanondoNo ratings yet
- 13 Genital Tract InjuriesDocument100 pages13 Genital Tract InjuriesRana Vandana100% (1)
- GIS1 - K1,2 - Anatomi Dan EmbriologiDocument70 pagesGIS1 - K1,2 - Anatomi Dan EmbriologiNatasya Ryani PurbaNo ratings yet
- Large IntestineDocument29 pagesLarge IntestineOlaifa victorNo ratings yet
- HerniaDocument47 pagesHerniamalathiNo ratings yet
- Inguinal Hernia Ana PhyDocument16 pagesInguinal Hernia Ana PhyJay Marie GonzagaNo ratings yet
- Practices of Anorectal SurgeryFrom EverandPractices of Anorectal SurgeryDong Keun LeeNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- STD & PidDocument61 pagesSTD & Pidsyirah99No ratings yet
- Nurul Insyirah Mohamed Hatta: Current AddressDocument3 pagesNurul Insyirah Mohamed Hatta: Current Addresssyirah99No ratings yet
- Pain in PregnancyDocument60 pagesPain in Pregnancysyirah99No ratings yet
- English Motivational Committee LetterDocument3 pagesEnglish Motivational Committee Lettersyirah99No ratings yet
- KMC 2016 Final Results Published v.3.2 1Document2,452 pagesKMC 2016 Final Results Published v.3.2 1syirah990% (1)
- Impact of ICT On Society:: Lack of Security and Its Effect On Industry, Economy and GovermentDocument10 pagesImpact of ICT On Society:: Lack of Security and Its Effect On Industry, Economy and Govermentsyirah99No ratings yet
- Fetal Vibroacoustic Stimulation Use GuidelinesDocument2 pagesFetal Vibroacoustic Stimulation Use GuidelinesSANANo ratings yet
- StepDocument2 pagesStepAdriana Ysabelle Mercado ArimangNo ratings yet
- ERP Comm Line WII Lematang Add WakatekDocument1 pageERP Comm Line WII Lematang Add WakatekAcunNo ratings yet
- Libro Cuando Mis Preocupaciones Se Hacen Demasiado GrandesDocument46 pagesLibro Cuando Mis Preocupaciones Se Hacen Demasiado GrandesMayra TorresNo ratings yet
- MSDS Khai Báo PDFDocument8 pagesMSDS Khai Báo PDFViệtDũngNo ratings yet
- Unesco Als Ls5 m05 v2.1Document60 pagesUnesco Als Ls5 m05 v2.1als midsayap1100% (3)
- 3 Day Keto Meal PlanDocument22 pages3 Day Keto Meal Planjose96% (27)
- A3.01 Union List of Food Additives Approved For Use in FoodDocument33 pagesA3.01 Union List of Food Additives Approved For Use in FoodBesian OsmaniNo ratings yet
- Major Case Presentation On Acute Pulmonary Embolism WithDocument13 pagesMajor Case Presentation On Acute Pulmonary Embolism WithPratibha NatarajNo ratings yet
- Department of Education: Training, Event and Project Proposal (Tepp) FormDocument2 pagesDepartment of Education: Training, Event and Project Proposal (Tepp) FormGreg Amor OmapasNo ratings yet
- Unit-5 Indoor Air Quality ManagementDocument44 pagesUnit-5 Indoor Air Quality Managementpthangarasu sctengNo ratings yet
- School Safety Assessment Tool (SSAT) 2022 For The Progressive Expansion of The Face-to-Face Learning ModalityDocument6 pagesSchool Safety Assessment Tool (SSAT) 2022 For The Progressive Expansion of The Face-to-Face Learning ModalityDarrel FadrillanNo ratings yet
- PWHS FORM 5 QUEZON KONSULTA HEALTH ASSESSMENT TOOL v5 FOR MISSIONDocument2 pagesPWHS FORM 5 QUEZON KONSULTA HEALTH ASSESSMENT TOOL v5 FOR MISSIONKristin VillasenotNo ratings yet
- Curriculum Vitae Vincent J. Felitti, M.D. Born: Citizenship: Current PositionDocument1 pageCurriculum Vitae Vincent J. Felitti, M.D. Born: Citizenship: Current PositionMWWNo ratings yet
- WHO Good Manufacturing Practices For Medicinal GasesDocument30 pagesWHO Good Manufacturing Practices For Medicinal Gasesdj22500No ratings yet
- Subject: English For Academic and Professional Purposes: Teacher: Ms. Jhonelyn Rose M. Mogueis, LPTDocument20 pagesSubject: English For Academic and Professional Purposes: Teacher: Ms. Jhonelyn Rose M. Mogueis, LPTJhonel Mogueis Dela Cruz100% (3)
- Female Ejaculation and The G-SpotDocument188 pagesFemale Ejaculation and The G-SpotRui Alves0% (1)
- Rebekah Wilson PT ResumeDocument3 pagesRebekah Wilson PT Resumeapi-487211279No ratings yet
- Wife Cheated On Me Part 7Document10 pagesWife Cheated On Me Part 7draculaa9No ratings yet
- Ar TC 2 Healy Medical Home InformationDocument1 pageAr TC 2 Healy Medical Home Informationapi-334098125No ratings yet
- Copia de PBSTUDIO PresentationDocument9 pagesCopia de PBSTUDIO PresentationBué Dominguez PerugaNo ratings yet
- Hersey-Blanchard Situational Leadership TheoryDocument17 pagesHersey-Blanchard Situational Leadership TheoryDahrshini MuraleeNo ratings yet
- Limitations of Qualitative Research ThesisDocument6 pagesLimitations of Qualitative Research Thesisgj9cpzxs100% (2)
- FINAL - Media Statement - MCH Update SMRMCDocument1 pageFINAL - Media Statement - MCH Update SMRMCEdlyn Jade TagulaoNo ratings yet
- Nosocomial Infections For BSN 2021Document48 pagesNosocomial Infections For BSN 2021Muhammad SheerazNo ratings yet
- Full Mouth Rehabilitation of Early Childhood Caries: A Case ReportDocument4 pagesFull Mouth Rehabilitation of Early Childhood Caries: A Case ReportSKRYBE LOLNo ratings yet
- Full Index of Fact Sheets - Final 495838 7Document232 pagesFull Index of Fact Sheets - Final 495838 7garbagepatchNo ratings yet