Download as pdf or txt
You might also like
- Management Control System Case "Family Care Specialists Medical Group, Inc"Document3 pagesManagement Control System Case "Family Care Specialists Medical Group, Inc"ainiNo ratings yet
- The Family Medicine Board Review Book 2018 PDFDocument1,113 pagesThe Family Medicine Board Review Book 2018 PDFSalem ELsayed Abdel Aziz100% (12)
- IUSM Regional CampusesDocument9 pagesIUSM Regional CampusesIUSM MSENo ratings yet
- Family Practice Handbook 4edDocument593 pagesFamily Practice Handbook 4eddeb haart100% (1)
- Continuity of Care: Literature Review and ImplicationsDocument10 pagesContinuity of Care: Literature Review and ImplicationsRona RihadahNo ratings yet
- The Athletic MusicianDocument2 pagesThe Athletic MusicianPaul Bravogarcía100% (1)
- Nutrition in The Intensive Care UnitDocument7 pagesNutrition in The Intensive Care UnitElessawey AbdallahNo ratings yet
- Furr Stimming Erin Educating Residents and Students inDocument15 pagesFurr Stimming Erin Educating Residents and Students inAnonymous tG35SYROzENo ratings yet
- 1 - Educación Nutricional en La Escuela de MedicinaDocument2 pages1 - Educación Nutricional en La Escuela de MedicinakbuhringNo ratings yet
- Nutrition in Medical PDFDocument17 pagesNutrition in Medical PDFtantrin novaNo ratings yet
- Issues in Nursing OrganizationsDocument6 pagesIssues in Nursing Organizationssebast107No ratings yet
- archivev3i3MDIwMTMxMDIy PDFDocument9 pagesarchivev3i3MDIwMTMxMDIy PDFLatasha WilderNo ratings yet
- (Journal of Neurosurgery - Spine) Patient Misconceptions Concerning Lumbar Spondylosis Diagnosis and TreatmentDocument7 pages(Journal of Neurosurgery - Spine) Patient Misconceptions Concerning Lumbar Spondylosis Diagnosis and Treatmentefancoolhand09No ratings yet
- Disability Attitudes in Health Care: A New Scale InstrumentDocument12 pagesDisability Attitudes in Health Care: A New Scale InstrumentLeila FortesNo ratings yet
- Why We Need To Know Patients' Education: Invited CommentaryDocument2 pagesWhy We Need To Know Patients' Education: Invited Commentaryabraham rumayaraNo ratings yet
- Mathew 2017Document6 pagesMathew 2017GodlipNo ratings yet
- 1 s2.0 S1836955319300578 MainDocument12 pages1 s2.0 S1836955319300578 MainSairam PhysioNo ratings yet
- Dias 2013Document12 pagesDias 2013Santiago Diaz PinillosNo ratings yet
- Pediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsDocument5 pagesPediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsGio VandaNo ratings yet
- ASPEN - Suplemental Parenteral Nutrition - Review of The Literature and Current Nutriton GuidelinesDocument11 pagesASPEN - Suplemental Parenteral Nutrition - Review of The Literature and Current Nutriton GuidelinesRoberto Cárdenas GarcíaNo ratings yet
- Nursing HealthcareDocument8 pagesNursing HealthcareBrobafettNo ratings yet
- Compliance With Universal Precautions in A Medical Practice With A High Rate of HIV InfectionDocument6 pagesCompliance With Universal Precautions in A Medical Practice With A High Rate of HIV InfectionDirga Rasyidin LNo ratings yet
- Reinvigorating The Clinical Examination For The 21st CenturDocument6 pagesReinvigorating The Clinical Examination For The 21st CenturAnnette GaspardNo ratings yet
- Sci Transl Med 2015 VassyDocument3 pagesSci Transl Med 2015 VassyJesus NavarroNo ratings yet
- The Effect of Emergency Department Crowding On Patient Outcomes: A Literature ReviewDocument4 pagesThe Effect of Emergency Department Crowding On Patient Outcomes: A Literature ReviewRohon EzekielNo ratings yet
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDocument30 pagesJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The Adultsulemi castañonNo ratings yet
- Mechanical Ventilation Training During Graduate Medical Education: Perspectives and Review of The LiteratureDocument13 pagesMechanical Ventilation Training During Graduate Medical Education: Perspectives and Review of The LiteratureAbdullah MohdNo ratings yet
- Rose Joseph 1Document8 pagesRose Joseph 1Misbah Sajid ChaudhryNo ratings yet
- Hypo FPX 4020 Assessment 3Document14 pagesHypo FPX 4020 Assessment 3Sheela malhiNo ratings yet
- Bedside Teaching of Medical StudentsDocument2 pagesBedside Teaching of Medical StudentsRafi Ullah HaleemNo ratings yet
- A Review of The Evidence and Recommendations On Communication Skills and The PatientDocument26 pagesA Review of The Evidence and Recommendations On Communication Skills and The PatientThayna MirandaNo ratings yet
- 2019 Article 305 PDFDocument3 pages2019 Article 305 PDFDipyanalarNo ratings yet
- SSP ArticleDocument6 pagesSSP Articleapi-740259455No ratings yet
- Landscape Analysis of Breastfeeding-Related Physician Education in The United StatesDocument11 pagesLandscape Analysis of Breastfeeding-Related Physician Education in The United StatesGraciela SeveriniNo ratings yet
- Nutrition in Medical Education in Latin America Results of A Cross-Sectional Survey. PrintDocument9 pagesNutrition in Medical Education in Latin America Results of A Cross-Sectional Survey. PrintEDWARD STEVE CAÑIZARES ALVAREZNo ratings yet
- Family-Centred Care in Paediatric and Neonatal Nursing - A Literature ReviewDocument4 pagesFamily-Centred Care in Paediatric and Neonatal Nursing - A Literature Reviewhyzypif0gif3No ratings yet
- The Pediatric Alliance For Cordinated Care Evaluation of A Medical Home ModelDocument12 pagesThe Pediatric Alliance For Cordinated Care Evaluation of A Medical Home ModelSuzana CarvalhoNo ratings yet
- The Effect of Adverse Childhood Experience Training Screenin 2023 EClinicalDocument13 pagesThe Effect of Adverse Childhood Experience Training Screenin 2023 EClinicalronaldquezada038No ratings yet
- Clinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentDocument18 pagesClinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentΜαρία ΧανιωτάκηNo ratings yet
- Student-Run Health Clinic: Novel Arena To Educate Medical Students On Systems-Based PracticeDocument13 pagesStudent-Run Health Clinic: Novel Arena To Educate Medical Students On Systems-Based Practicemilica-miric-7311No ratings yet
- Manuscript Revision 10.15.20Document22 pagesManuscript Revision 10.15.20John SmithNo ratings yet
- En CuestaDocument6 pagesEn CuestaToño VargasNo ratings yet
- An Insight Into Clinical Nursing JudgementDocument7 pagesAn Insight Into Clinical Nursing Judgementapi-546705901No ratings yet
- Cancers 15 00693 With CoverDocument17 pagesCancers 15 00693 With CoverBorja Recuenco CayuelaNo ratings yet
- Educating Nursing Students About Health Literacy - From The Classroom To The Patient BedsideDocument11 pagesEducating Nursing Students About Health Literacy - From The Classroom To The Patient BedsideKusrini Kadar SyamsalamNo ratings yet
- Chapter 5 - Understanding Evidence-Based PracticeDocument29 pagesChapter 5 - Understanding Evidence-Based PracticeIgnacio TroianoNo ratings yet
- Jurnal InggrisDocument10 pagesJurnal InggrisYovi PransiskaNo ratings yet
- Trends in Publications About Cerebral PalsyDocument11 pagesTrends in Publications About Cerebral Palsycvdk8dc8sbNo ratings yet
- The Need To Advance Nutrition EducationDocument14 pagesThe Need To Advance Nutrition EducationAna RMNo ratings yet
- Erosion of Empathy in Medical SchoolDocument1 pageErosion of Empathy in Medical SchoolChristian ObandoNo ratings yet
- Adolescent With CFSDocument6 pagesAdolescent With CFSiri_balNo ratings yet
- Culinary Nutr Course Equips Future Physicians To Educate Patients On A Healthy Diet (Wood NI Et Al, BMC Med Educ 2021)Document11 pagesCulinary Nutr Course Equips Future Physicians To Educate Patients On A Healthy Diet (Wood NI Et Al, BMC Med Educ 2021)Sa'diah Multi KarinaNo ratings yet
- Ijhpm 4 417Document14 pagesIjhpm 4 417JasmitaNo ratings yet
- Sleep Disturbances Among Medical Students: A Global PerspectiveDocument6 pagesSleep Disturbances Among Medical Students: A Global PerspectiveShinichi Conan HaibaraNo ratings yet
- St. Paul University PhilippinesDocument4 pagesSt. Paul University PhilippinesleiNo ratings yet
- The Importance of Health Literacy in Physiotherapy Practice: Andrew M Briggs and Joanne E JordanDocument3 pagesThe Importance of Health Literacy in Physiotherapy Practice: Andrew M Briggs and Joanne E JordanMhmd IrakyNo ratings yet
- 1 s2.0 S0002945923032072 MainDocument8 pages1 s2.0 S0002945923032072 Mainsoam.nadeem23No ratings yet
- Are Knowledge Gaps An Expected Result of The Current Culture of Neurosurgical Resident TrainingDocument3 pagesAre Knowledge Gaps An Expected Result of The Current Culture of Neurosurgical Resident Trainingghcabsb87No ratings yet
- Research Article: Osteoporosis Knowledge of Students in Relevant Healthcare Academic ProgramsDocument4 pagesResearch Article: Osteoporosis Knowledge of Students in Relevant Healthcare Academic ProgramsAnonymous V5l8nmcSxbNo ratings yet
- 1 s2.0 S2213076418300654 MainDocument5 pages1 s2.0 S2213076418300654 MaindaytdeenNo ratings yet
- Platform Abstracts / Journal of Adolescent Health 68 (2021) S20 Es59 S23Document2 pagesPlatform Abstracts / Journal of Adolescent Health 68 (2021) S20 Es59 S23Gina GuisamanoNo ratings yet
- Elearning: A Review of Internet-Based Continuing Medical EducationDocument11 pagesElearning: A Review of Internet-Based Continuing Medical EducationKamran AfzalNo ratings yet
- Igx004 2993Document1 pageIgx004 2993Arifah Budiarti NurfitriNo ratings yet
- Shane Mcwhorter2002Document15 pagesShane Mcwhorter2002Basilharbi HammadNo ratings yet
- PIIS0031395514001801Document2 pagesPIIS0031395514001801DavidBeatonComuladaNo ratings yet
- UE 1 Clavicle FracturesDocument46 pagesUE 1 Clavicle FracturesDavidBeatonComuladaNo ratings yet
- Matching Nail Angle and Native Neck-Shaft AngleDocument4 pagesMatching Nail Angle and Native Neck-Shaft AngleDavidBeatonComuladaNo ratings yet
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 pagesDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaNo ratings yet
- Synergy Hip System-SmallerDocument20 pagesSynergy Hip System-SmallerDavidBeatonComuladaNo ratings yet
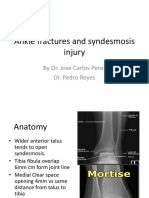
- Ankle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDocument11 pagesAnkle Fractures and Syndesmosis Injury: by Dr. Jose Carlos Perez Dr. Pedro ReyesDavidBeatonComuladaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Vahedi2020 PDFDocument4 pagesVahedi2020 PDFDavidBeatonComuladaNo ratings yet
- Total Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDocument6 pagesTotal Joint Arthroplasty in Patients With Osteopetrosis: A Report of 5 Cases and Review of The LiteratureDavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Osteoarthritis Associated With Osteopetrosis.30Document6 pagesOsteoarthritis Associated With Osteopetrosis.30DavidBeatonComuladaNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Rheumatoid Hand and Wrist Surgery Soft Tissue.99323Document9 pagesRheumatoid Hand and Wrist Surgery Soft Tissue.99323DavidBeatonComuladaNo ratings yet
- Vanhove2014 PDFDocument5 pagesVanhove2014 PDFDavidBeatonComuladaNo ratings yet
- Meltem ÖZBEK YAŞAR CV - Eng1Document4 pagesMeltem ÖZBEK YAŞAR CV - Eng1meltemNo ratings yet
- Community Oriented Primary CareDocument8 pagesCommunity Oriented Primary Carebanigul100% (2)
- Presentation NandaDocument32 pagesPresentation NandaANIS MURNIATINo ratings yet
- New York Health Acquires Three Village Family MedicineDocument2 pagesNew York Health Acquires Three Village Family MedicinePR.comNo ratings yet
- Medical MalpracticeDocument16 pagesMedical MalpracticekruzipNo ratings yet
- Clinic ListDocument2 pagesClinic ListLINDA SAPRIANTINo ratings yet
- Cashless Request Form PDFDocument2 pagesCashless Request Form PDFPrime multispecialiaty HospitalNo ratings yet
- AMA SpecialtyByTOPS 12-9-10Document10 pagesAMA SpecialtyByTOPS 12-9-10bmartindoyle6396No ratings yet
- AKU-NAMA - Winter 2008Document24 pagesAKU-NAMA - Winter 2008Abdul Basit SaeedNo ratings yet
- This Document and The Information Thereon Is The Property of PHINMA Education (Department of Nursing)Document8 pagesThis Document and The Information Thereon Is The Property of PHINMA Education (Department of Nursing)Mark Raymunstine TamposNo ratings yet
- Booklet PDFDocument82 pagesBooklet PDFSaikat BiswasNo ratings yet
- v1 ThomsonDocument59 pagesv1 ThomsonFarshid GheisariNo ratings yet
- Provincail Exam Spec TotalDocument48 pagesProvincail Exam Spec TotalJim ChenNo ratings yet
- Social MedDocument6 pagesSocial MedIntekhabAtaharNo ratings yet
- MI AG Speaker BiographiesDocument5 pagesMI AG Speaker BiographiesJames CampbellNo ratings yet
- Seats DNB 13Document81 pagesSeats DNB 13alansamqlnNo ratings yet
- Harmacotherapy Rinciples RacticeDocument30 pagesHarmacotherapy Rinciples RacticebencleeseNo ratings yet
- Family Medicine Thesis TopicsDocument4 pagesFamily Medicine Thesis Topicspatriciaadamsjackson100% (1)
- Pitch Deck of A Medical Software For ClinicsDocument11 pagesPitch Deck of A Medical Software For ClinicsAl KeyNo ratings yet
- Tadao Okada, MD, MPH, DABFM, FAAFP Brief Bio & CV (2012 - 9)Document3 pagesTadao Okada, MD, MPH, DABFM, FAAFP Brief Bio & CV (2012 - 9)Tadao Okada, MD, MPH, DABFM, FAAFPNo ratings yet
- The Grapevine, November 13, 2013Document32 pagesThe Grapevine, November 13, 2013grapevineNo ratings yet
- Tick Removal: Office ProceduresDocument3 pagesTick Removal: Office ProceduresbararnikhilNo ratings yet
- Marier - ST Onge 510essayDocument7 pagesMarier - ST Onge 510essayGenevieveMarierSt-OngeNo ratings yet
- Mmed Fammed 2014-15Document12 pagesMmed Fammed 2014-15aravindNo ratings yet
- DR Ahmed Abar CVDocument7 pagesDR Ahmed Abar CVAnonymous H1EZvy1yQNo ratings yet