Download as pdf or txt
You might also like
- Drug Study (Epinephrine, Lidocaine, Diazepam)Document6 pagesDrug Study (Epinephrine, Lidocaine, Diazepam)Abigaile Operiano100% (2)
- ToxicologyDocument8 pagesToxicologysarguss14100% (3)
- How To Lose Weight and Keep It OffDocument2 pagesHow To Lose Weight and Keep It OffLUMINITA GIUCANo ratings yet
- Reviewer 6Document6 pagesReviewer 6asdfdjfeonaNo ratings yet
- Psychotropic DrugsDocument29 pagesPsychotropic DrugsBahaa ShaabanNo ratings yet
- Drug Testing I. Definition of TermsDocument7 pagesDrug Testing I. Definition of TermsMichael Salazar OcampoNo ratings yet
- Major Symptoms: Nursing ResponsibilitiesDocument5 pagesMajor Symptoms: Nursing ResponsibilitiesAraw GabiNo ratings yet
- Pharmacology Neuromuscular DisordersDocument4 pagesPharmacology Neuromuscular Disorders8dxf5bqv6gNo ratings yet
- PsychopharmacologyDocument8 pagesPsychopharmacologyzashileighNo ratings yet
- Anti ParkinsonsDocument4 pagesAnti ParkinsonsMichaela BernadasNo ratings yet
- Pharma Lecture Midterm ReviewerDocument28 pagesPharma Lecture Midterm ReviewerKristel RolloNo ratings yet
- Drug StudyDocument7 pagesDrug StudyVenus April LimonNo ratings yet
- NPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesDocument83 pagesNPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Other CNS Drugs MonasDocument172 pagesOther CNS Drugs MonasMichael MohammedNo ratings yet
- Pharma Nca1 Notes MidtermDocument8 pagesPharma Nca1 Notes MidtermAICEL A. ABILNo ratings yet
- Opioid AnalgesicsDocument27 pagesOpioid AnalgesicsScribdTranslationsNo ratings yet
- Pcol 1 Prefinals Part 1 PDFDocument9 pagesPcol 1 Prefinals Part 1 PDFJillian Mae DacerNo ratings yet
- Perphenazine Drug StudyDocument4 pagesPerphenazine Drug Studyshadow gonzalezNo ratings yet
- Pharma Lab. Activity 2Document55 pagesPharma Lab. Activity 2Majestic RavenNo ratings yet
- By Duy Thai, 1997: Diffuse Out of Nerve Terminal and Act On COMPT in External TissuesDocument5 pagesBy Duy Thai, 1997: Diffuse Out of Nerve Terminal and Act On COMPT in External Tissuesravi2likeNo ratings yet
- Anti ParkinsonsDocument4 pagesAnti ParkinsonsMichaela BernadasNo ratings yet
- Drug Study, Olanzapine, Kalium Durule, AripiprazoleDocument7 pagesDrug Study, Olanzapine, Kalium Durule, Aripiprazoleroshannevergara0777No ratings yet
- Autonomic Nervous System PharmacologyDocument97 pagesAutonomic Nervous System PharmacologyKarun Kumar Shingari100% (1)
- Psychotropic Substance Hallucinogens and Dissociatives - CompressedDocument39 pagesPsychotropic Substance Hallucinogens and Dissociatives - CompressedshuyuichewNo ratings yet
- Presented byDocument71 pagesPresented byRun HajNo ratings yet
- Amine Hypothesis of Affective DisorderDocument36 pagesAmine Hypothesis of Affective DisorderRupinder GillNo ratings yet
- Opioids - An IntroductionDocument48 pagesOpioids - An IntroductionPranathi PrasadNo ratings yet
- DeliriumDocument16 pagesDeliriumMission JupiterNo ratings yet
- FlupentixolDocument3 pagesFlupentixolshiplusNo ratings yet
- Neurotransmission and Its ClassificationDocument40 pagesNeurotransmission and Its ClassificationDr_GSNo ratings yet
- Non Cat Echo La MinesDocument4 pagesNon Cat Echo La MinesM Yusuf Ali RNo ratings yet
- Autonomic Drugs 3Document34 pagesAutonomic Drugs 3ismailaiaibrahimNo ratings yet
- NCM 106 Drugs Acting On ANS - Synchronous Session Ver 2Document7 pagesNCM 106 Drugs Acting On ANS - Synchronous Session Ver 2Crecia Bullecer2No ratings yet
- Pharmacological Treatment: Antipsychotics: Mechanism of ActionDocument7 pagesPharmacological Treatment: Antipsychotics: Mechanism of Actionvarsha thakurNo ratings yet
- Pengantar Toksikologi Dan ToxindromeDocument29 pagesPengantar Toksikologi Dan ToxindromeCalvin Tanuwijaya Stick BolaNo ratings yet
- By: Professor Emiliano Z. Sison JRDocument40 pagesBy: Professor Emiliano Z. Sison JRT Z BenNo ratings yet
- 404T Opioid Analgesics and AntagonistDocument14 pages404T Opioid Analgesics and AntagonistRaja RajaNo ratings yet
- Neurotransmitter: S P SutamaDocument22 pagesNeurotransmitter: S P Sutamaanon_134497206No ratings yet
- Autonomic Nervous SystemDocument54 pagesAutonomic Nervous SystemEzio SartoraNo ratings yet
- Parkinsons DiseaseDocument3 pagesParkinsons Diseasem3d1kNo ratings yet
- Drug Study CCMHDocument35 pagesDrug Study CCMHJose Mari F. EsguerraNo ratings yet
- Cns AgentsDocument10 pagesCns Agentsroldanmarygrace023No ratings yet
- CardiotropicsDocument4 pagesCardiotropicsbeans taralaNo ratings yet
- NCM 106 Week 5 and 6 ReviewerDocument15 pagesNCM 106 Week 5 and 6 ReviewerCrecia Bullecer2No ratings yet
- PharmaDocument3 pagesPharmaVinceNo ratings yet
- Pharmacology 040 - Anti Psychotic DrugsDocument6 pagesPharmacology 040 - Anti Psychotic DrugsKaye NeeNo ratings yet
- Toxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiDocument59 pagesToxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiTan Geok EngNo ratings yet
- Agitated PatientDocument2 pagesAgitated PatientCassandra GeldenhuysNo ratings yet
- 404T CNS StimulantsDocument19 pages404T CNS StimulantsRaja RajaNo ratings yet
- CC3 Finals Toxicology of The Drugs of Abuse-1Document4 pagesCC3 Finals Toxicology of The Drugs of Abuse-1Gabriel QuillNo ratings yet
- Adrenoceptor - Activating Other Sympathomimetic Drugs PDFDocument43 pagesAdrenoceptor - Activating Other Sympathomimetic Drugs PDFRupal RaghuwanshiNo ratings yet
- Agricultural PoisonDocument25 pagesAgricultural Poisons.shreevarshiniNo ratings yet
- 2022 Anesth s1t8 Intravenous Anesthesia and OpioidsDocument10 pages2022 Anesth s1t8 Intravenous Anesthesia and OpioidsmedicoNo ratings yet
- Pharmacology of AntidepressantsDocument28 pagesPharmacology of Antidepressantsحيدر كريم سعيد حمزهNo ratings yet
- Sympathomimetics and SympatholyticsDocument3 pagesSympathomimetics and Sympatholyticsbunso padillaNo ratings yet
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- ACTIVITY 14. 1. Drugs Affecting The CNS Mechanism of Action Indications Adverse Effects Important Nursing ConsiderationsDocument19 pagesACTIVITY 14. 1. Drugs Affecting The CNS Mechanism of Action Indications Adverse Effects Important Nursing ConsiderationsPatricia Dianne RuizNo ratings yet
- Clinical ToxicologyDocument8 pagesClinical Toxicologysarguss14100% (1)
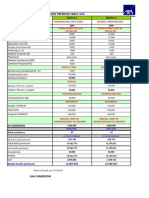
- COTATION AFCOTT CAM SARL - Fr.enDocument1 pageCOTATION AFCOTT CAM SARL - Fr.enMichel erickson talom waboNo ratings yet
- CHHEM SirikaDocument23 pagesCHHEM SirikaSirika ChhemNo ratings yet
- USFDA Regulatory Toxicology OverviewDocument100 pagesUSFDA Regulatory Toxicology OverviewHarsh KoshtiNo ratings yet
- A Case Study of Cognitive Behavior Therapy of Obsessive Compulsive Disorder Content File PDFDocument18 pagesA Case Study of Cognitive Behavior Therapy of Obsessive Compulsive Disorder Content File PDFAleksandra CvetkovicNo ratings yet
- Kasus Farmakokinetika Klinik AntibiotikaDocument2 pagesKasus Farmakokinetika Klinik AntibiotikaMr-Eng DeathbatthefallensevenfoldismNo ratings yet
- Neuropathic Pain AssignmentDocument3 pagesNeuropathic Pain Assignmentbattal eduNo ratings yet
- Oral Health 1-3&5Document38 pagesOral Health 1-3&5Umar FarouqNo ratings yet
- Procedure in Assessing The Body Temperature Using A Mercury ThermometerDocument10 pagesProcedure in Assessing The Body Temperature Using A Mercury Thermometercrrfrnc50% (4)
- Acute Leukemia - Knowledge at AMBOSSDocument1 pageAcute Leukemia - Knowledge at AMBOSSRenad AlharbiNo ratings yet
- Celiac Disease: Signs and SymptomsDocument7 pagesCeliac Disease: Signs and SymptomsPrincess Dianne Difuntorum MabezaNo ratings yet
- YMMNO ProposalDocument2 pagesYMMNO ProposalYamon Min Nyunt OoNo ratings yet
- Developmental Dysplasia of The Hip - Clinical Features and Diagnosis - UpToDateDocument13 pagesDevelopmental Dysplasia of The Hip - Clinical Features and Diagnosis - UpToDateFernandoVianaNo ratings yet
- B4 HAND DefinitionDocument13 pagesB4 HAND DefinitionFajar Rudy QimindraNo ratings yet
- Management of Sore ThroatDocument11 pagesManagement of Sore ThroatSheera EiyraaNo ratings yet
- Arthritis Rheumatology - 2021 - Chung - 2021 American College of Rheumatology Vasculitis Foundation Guideline For TheDocument10 pagesArthritis Rheumatology - 2021 - Chung - 2021 American College of Rheumatology Vasculitis Foundation Guideline For TheDiana RamirezNo ratings yet
- Abruptio Placentae 2Document23 pagesAbruptio Placentae 2api-370504650% (2)
- Fisiologi BerkemihDocument34 pagesFisiologi BerkemihTunik SugiantoNo ratings yet
- Microbial and Virulent View To Causative Agent of Foot and Mouth Disease in Unvaccinated Dairy Cows in Diyala Governorate, IraqDocument4 pagesMicrobial and Virulent View To Causative Agent of Foot and Mouth Disease in Unvaccinated Dairy Cows in Diyala Governorate, IraqCentral Asian StudiesNo ratings yet
- IPMAT Response SheetDocument50 pagesIPMAT Response SheetJaydev JaswaniNo ratings yet
- Andreas Ludwig Kalcker - How To Detect and Treat A Parasitic InfectionDocument16 pagesAndreas Ludwig Kalcker - How To Detect and Treat A Parasitic InfectionOtpor Stoko100% (7)
- Nursing Care PlanDocument4 pagesNursing Care PlanKath RubioNo ratings yet
- Post-Partum Depression Effect On Child Health and DevelopmentDocument6 pagesPost-Partum Depression Effect On Child Health and DevelopmentEndang JunaelaNo ratings yet
- Factors Affecting Postoperative Recovery in Fort Portal Regional Referral Hospital, UgandaDocument6 pagesFactors Affecting Postoperative Recovery in Fort Portal Regional Referral Hospital, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Visual Anosognosia (Anton-Babinski Syndrome) : Report of Two Cases Associated With Ischemic Cerebrovascular DiseaseDocument5 pagesVisual Anosognosia (Anton-Babinski Syndrome) : Report of Two Cases Associated With Ischemic Cerebrovascular DiseaseHanna EnitaNo ratings yet
- Saroj Devi - DR Shahbaz Mohd Khan Online Opinion 3Document1 pageSaroj Devi - DR Shahbaz Mohd Khan Online Opinion 3Krishna JainNo ratings yet
- Causes of Mental IllnessDocument4 pagesCauses of Mental IllnessRima Pigar Goza MeleloaNo ratings yet
- Case Presentation ENTDocument39 pagesCase Presentation ENTtarshaNo ratings yet
- Ezpap - Effects of EzPAP Post Operatively in Coronary Artery Bypass Graft PatientsDocument1 pageEzpap - Effects of EzPAP Post Operatively in Coronary Artery Bypass Graft Patientsjesushenandez_ftrNo ratings yet
- Final - Specifications of Stereotactic FrameDocument2 pagesFinal - Specifications of Stereotactic FrameadeshdrNo ratings yet