Download as pdf or txt
You might also like
- MYMAXICARE REVISED BROCHURE 2023 - FinalDocument16 pagesMYMAXICARE REVISED BROCHURE 2023 - FinalAna Feliciano100% (1)
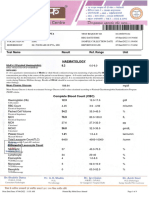
- Haematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountDocument2 pagesHaematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountlijoNo ratings yet
- Lab Report 2157646 20210113110650Document3 pagesLab Report 2157646 20210113110650marlon molinaNo ratings yet
- Gastric Outlet ObstructionDocument9 pagesGastric Outlet ObstructionVivek AhanthemNo ratings yet
- Antiretroviral Therapy Guidelines For HIV-Infected Adults and AdolescentsDocument122 pagesAntiretroviral Therapy Guidelines For HIV-Infected Adults and AdolescentsManoj Kumar MeenaNo ratings yet
- Med Micro AlgorithmsDocument2 pagesMed Micro Algorithmsgregoryvo100% (11)
- Report - 40204702576 - P SAI TEJADocument4 pagesReport - 40204702576 - P SAI TEJASai GopiNo ratings yet
- Test Report: Hemogram Test Name Units Results Bio. Ref. IntervalDocument19 pagesTest Report: Hemogram Test Name Units Results Bio. Ref. Intervalcs2015ok77No ratings yet
- Bloodtest - 20th JuneDocument2 pagesBloodtest - 20th Junenagarjunah1027No ratings yet
- PdfText (38) - 240317 - 201242Document7 pagesPdfText (38) - 240317 - 201242Anurag SharmaNo ratings yet
- LDSPLDocument8 pagesLDSPLSoham DattaNo ratings yet
- 25262lab ReportDocument3 pages25262lab Reportsayand2001No ratings yet
- Mfine Doc 1696249829240Document4 pagesMfine Doc 1696249829240shriniwash5558No ratings yet
- PS325781Document9 pagesPS325781Uchiha ItachiNo ratings yet
- LifeCare Dera PDFDocument9 pagesLifeCare Dera PDFsandeep singh cheemaNo ratings yet
- Haematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountDocument8 pagesHaematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountArun DheekshahNo ratings yet
- .Trashed 1716374771 RHP2308415Document4 pages.Trashed 1716374771 RHP2308415Anita DwivediNo ratings yet
- GOR2208631Document6 pagesGOR2208631SakshiNo ratings yet
- Complete Blood Count: Patient.: Mrs. Sharmila SinghDocument1 pageComplete Blood Count: Patient.: Mrs. Sharmila SinghShivansh SinghNo ratings yet
- PDF TextDocument4 pagesPDF TextABHISHEK SINGHNo ratings yet
- Blood Test ReportDocument13 pagesBlood Test Report7415olymp7415No ratings yet
- Report 1703423614639Document9 pagesReport 1703423614639bsdkmcbc386No ratings yet
- Labreportnew PDFDocument4 pagesLabreportnew PDFMange Ram DhankharNo ratings yet
- CBC Blood Test NewDocument2 pagesCBC Blood Test Newrr10rahulNo ratings yet
- Mrs. V.dhana LakshmiDocument1 pageMrs. V.dhana LakshmiAnonymous lSZ9JVNo ratings yet
- D Seshagiri Rao-08Nov2023-Health CheDocument7 pagesD Seshagiri Rao-08Nov2023-Health CheSUNSHINE DIAGNOSTICSNo ratings yet
- Test Report: Reg - No Age/Sex Name::: Collection:: Received Reg - DateDocument5 pagesTest Report: Reg - No Age/Sex Name::: Collection:: Received Reg - DateNikhila TummaNo ratings yet
- Ms. Chhabi Ghosh: Test Name Result Unit Biological Ref - IntervalDocument7 pagesMs. Chhabi Ghosh: Test Name Result Unit Biological Ref - IntervalAbhishek VivekNo ratings yet
- Lab Report 6322614 20211124074028Document2 pagesLab Report 6322614 20211124074028renisNo ratings yet
- Dipanwita GhoshDocument6 pagesDipanwita Ghoshprotyushkar1No ratings yet
- Isaac Typhoid NegativeDocument5 pagesIsaac Typhoid Negativeganesh khondeNo ratings yet
- Scanner DocumentDocument8 pagesScanner Documenteg1rgNo ratings yet
- Issued To:: 10-Mar-2024 08:19 29 YearsDocument5 pagesIssued To:: 10-Mar-2024 08:19 29 YearsharshitakoutaNo ratings yet
- Lab Report 11867593 20230221104918Document3 pagesLab Report 11867593 20230221104918dineshyadav19900312No ratings yet
- Chetan CBCDocument1 pageChetan CBCLalit Surykant ChavanNo ratings yet
- Bhagwat PuranDocument12 pagesBhagwat PuranAaditya jhaNo ratings yet
- AkashDocument2 pagesAkashVimal NishadNo ratings yet
- Medical ReportsDocument5 pagesMedical Reportsritikapagraj01No ratings yet
- TestsDocument3 pagesTestsaddajrfNo ratings yet
- Final Laboratory ReportDocument5 pagesFinal Laboratory ReportSachinNo ratings yet
- Lab ReportDocument5 pagesLab ReportTAMKEEN MUSTAFANo ratings yet
- 5wmnean5n4mirxrgqi0xa4p5Document3 pages5wmnean5n4mirxrgqi0xa4p5gaamizs0987No ratings yet
- LabreportnewDocument16 pagesLabreportnewmirashaik3No ratings yet
- LabReportNew.aspxDocument6 pagesLabReportNew.aspxharkiratsinghdhanoa3No ratings yet
- Authenticity CheckDocument2 pagesAuthenticity Checkvlande897No ratings yet
- 5047UH0368065047 552937fDocument16 pages5047UH0368065047 552937fpeter smithNo ratings yet
- Test Report: Hematology Parameter Result Biological Reference Interval Complete Blood Count (CBC)Document5 pagesTest Report: Hematology Parameter Result Biological Reference Interval Complete Blood Count (CBC)Jay Deep GhoshNo ratings yet
- DgReportingVF PDFDocument2 pagesDgReportingVF PDFRamani DantuluriNo ratings yet
- DgReportingVF PDFDocument2 pagesDgReportingVF PDFRamani DantuluriNo ratings yet
- DG Reporting VFDocument2 pagesDG Reporting VFRamani DantuluriNo ratings yet
- MAHAAM3Document2 pagesMAHAAM3vlande897No ratings yet
- Comprehensive Body Profile: Method: (SLS)Document26 pagesComprehensive Body Profile: Method: (SLS)peter smithNo ratings yet
- Lab Report 11002949 20221215071852Document2 pagesLab Report 11002949 20221215071852Danish Ahemad SiddiquiNo ratings yet
- Report 1702735488541Document14 pagesReport 1702735488541Srilakshmi MNo ratings yet
- Lab Report 6079908 20211108075900Document4 pagesLab Report 6079908 20211108075900Shahid KvNo ratings yet
- File - Report (1665892839610)Document2 pagesFile - Report (1665892839610)Sameer KauraNo ratings yet
- Medibuddy-ATUL NARANGDocument4 pagesMedibuddy-ATUL NARANGCA Atul NarangNo ratings yet
- LifeCare DeraDocument13 pagesLifeCare Derasandeep singh cheemaNo ratings yet
- Abhishek 00034Document5 pagesAbhishek 00034abhidomadiya2121No ratings yet
- Alka Pandey-Female54 Years-53200Document1 pageAlka Pandey-Female54 Years-53200Shantanu PandeyNo ratings yet
- Test Report: Complete Blood Count (CBC)Document1 pageTest Report: Complete Blood Count (CBC)WSC ALMANo ratings yet
- LabreportnewDocument4 pagesLabreportnewSatvinder SinghNo ratings yet
- Department of Pathology: Mrs. Malyala SujathaDocument6 pagesDepartment of Pathology: Mrs. Malyala Sujathasanath kumarNo ratings yet
- Genetic Counseling: Presented By: Nivedita Kochar M.Sc. Nursing 1 YearDocument17 pagesGenetic Counseling: Presented By: Nivedita Kochar M.Sc. Nursing 1 YearNivedita NivuNo ratings yet
- Utd 22823 Case - Reports DasDocument5 pagesUtd 22823 Case - Reports DasVanny RosalinaNo ratings yet
- Brazilian Guidelines For The Monitoring and Treatment of Pediatric Allergic ConjunctivitisDocument11 pagesBrazilian Guidelines For The Monitoring and Treatment of Pediatric Allergic ConjunctivitisTatiana RecinosNo ratings yet
- 2014 Mrcs Osce RECALLDocument85 pages2014 Mrcs Osce RECALLIdo EgaziNo ratings yet
- Strabismus: Prepared By: Ayesah Janora A. Sarip Msu-Chs BSN IiDocument14 pagesStrabismus: Prepared By: Ayesah Janora A. Sarip Msu-Chs BSN IiTni JolieNo ratings yet
- Gordon'S Functional Health PatternDocument10 pagesGordon'S Functional Health PatternDave SapladNo ratings yet
- Molecular Biology: Test Name Result Reference Value/ Specimen Units Method Prev ResultDocument1 pageMolecular Biology: Test Name Result Reference Value/ Specimen Units Method Prev ResultPrasanna Das RaviNo ratings yet
- Nursing Care Plan Process Analysis Planning and ImplementationDocument2 pagesNursing Care Plan Process Analysis Planning and ImplementationVanessa Prieto100% (2)
- Disclosure: Complex Case: Complications After Cardiac Surgery - Glucose, Sedation and ThrombocytopeniaDocument27 pagesDisclosure: Complex Case: Complications After Cardiac Surgery - Glucose, Sedation and ThrombocytopeniaEnrique SánchezNo ratings yet
- Impaired Gas ExchangeDocument3 pagesImpaired Gas ExchangePaul VincentNo ratings yet
- Isoxilan Generic Name: Isoxsuprine: Drug StudyDocument2 pagesIsoxilan Generic Name: Isoxsuprine: Drug StudyJohn Paolo Tamayo OrioNo ratings yet
- StreptokinaseDocument8 pagesStreptokinaseemman_abzNo ratings yet
- Guide To IAPT Data and Publications PDFDocument90 pagesGuide To IAPT Data and Publications PDFsamNo ratings yet
- Acid Base ImbalanceDocument15 pagesAcid Base ImbalanceIoana SanduNo ratings yet
- Complication of FractureDocument18 pagesComplication of FractureJoni NeohNo ratings yet
- The 15 Health Benefits of Green ChilliesDocument3 pagesThe 15 Health Benefits of Green ChilliesMark Vincent ColamboNo ratings yet
- Cutaneous Larva MigransDocument4 pagesCutaneous Larva MigransanissabilfaqihNo ratings yet
- Topic 1: Molecules, Transport and Health Chapter 1B: Mammalian Transport SystemsDocument4 pagesTopic 1: Molecules, Transport and Health Chapter 1B: Mammalian Transport SystemsMariam El KhatibNo ratings yet
- PATHOPHYS - DermatologyDocument19 pagesPATHOPHYS - Dermatologyaagioaa100% (1)
- Tumor Flash Cards - Osteochondroma and Multiple Hereditary ExostosisDocument23 pagesTumor Flash Cards - Osteochondroma and Multiple Hereditary Exostosislaxge54No ratings yet
- PE - Module 5Document8 pagesPE - Module 5Hanah Grace GomezNo ratings yet
- Physical Agent For Cancer Survvors An Updated Literatured ReviewDocument9 pagesPhysical Agent For Cancer Survvors An Updated Literatured ReviewDeborah SalinasNo ratings yet
- Pregnancy: Signs/Symptoms and Common Health ConcernsDocument5 pagesPregnancy: Signs/Symptoms and Common Health ConcernsTracy50% (2)
- 10 1097@mpg 0000000000002779Document8 pages10 1097@mpg 0000000000002779Felipe Beltrán TorresNo ratings yet
- Case Discussion Day 2 - MatulaDocument1 pageCase Discussion Day 2 - MatulaTRISHA MATULANo ratings yet
- Vector Borne Disease and Infectious Disease FinalDocument35 pagesVector Borne Disease and Infectious Disease Finalerna.dumingNo ratings yet