Download as pdf or txt
You might also like
- CD Manual 09Document99 pagesCD Manual 09Matthew Ho100% (2)
- Covid CT Chest Scan Score & SeverityDocument7 pagesCovid CT Chest Scan Score & SeverityMohan DesaiNo ratings yet
- Original Research PaperDocument5 pagesOriginal Research PapersrijitNo ratings yet
- CT Manifestations of Coronavirus Disease 2019 A RDocument5 pagesCT Manifestations of Coronavirus Disease 2019 A ReugeniaNo ratings yet
- The Value of HRCT Chest in Diagnosis of COVID 19 and Its Correlation With RT-PCRDocument5 pagesThe Value of HRCT Chest in Diagnosis of COVID 19 and Its Correlation With RT-PCREditor IJETBSNo ratings yet
- The Pulmonary Sequalae in Discharged Patients With COVID-19: A Short-Term Observational StudyDocument7 pagesThe Pulmonary Sequalae in Discharged Patients With COVID-19: A Short-Term Observational StudyCloud NeilalungNo ratings yet
- Radiologi 3Document5 pagesRadiologi 3Sarah watiNo ratings yet
- Diagnostik Dasar Radiologis COVID-19Document42 pagesDiagnostik Dasar Radiologis COVID-19tenty isniNo ratings yet
- Evaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19Document7 pagesEvaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19IJAR JOURNALNo ratings yet
- Asymptomatic COVID-19 Patients at A COVID Designated Asymptomatic COVID-19 Patients at A COVID Designated Hospital in Nepal Hospital in NepalDocument7 pagesAsymptomatic COVID-19 Patients at A COVID Designated Asymptomatic COVID-19 Patients at A COVID Designated Hospital in Nepal Hospital in NepalJudelle Enriquez-GazaNo ratings yet
- Performance of Radiologists in Differentiating COVID-19 From Non-COVID-19 Viral Pneumonia at Chest CTDocument9 pagesPerformance of Radiologists in Differentiating COVID-19 From Non-COVID-19 Viral Pneumonia at Chest CTrishaNo ratings yet
- Tabatabaei2020 Article ALow-doseChestCTProtocolForTheDocument9 pagesTabatabaei2020 Article ALow-doseChestCTProtocolForTheyuda ibnuNo ratings yet
- Chest CT For Detecting COVID-19 A Systematic RevieDocument14 pagesChest CT For Detecting COVID-19 A Systematic RevieWiseup StudioNo ratings yet
- Chest CT Vs RT-PCR in Covid-19Document9 pagesChest CT Vs RT-PCR in Covid-19Srini AwallaNo ratings yet
- 1 s2.0 S2405630822000696 MainDocument7 pages1 s2.0 S2405630822000696 MainfumadelabuenaNo ratings yet
- CT Scan Vs PCR2Document6 pagesCT Scan Vs PCR2risanataliasiburianNo ratings yet
- Chest CT CovidDocument6 pagesChest CT CovidShinta FrennandaNo ratings yet
- Articulo DiagnósticoDocument9 pagesArticulo DiagnósticoevelynNo ratings yet
- Piis0167814019331123 230304 134522Document7 pagesPiis0167814019331123 230304 134522Samuel Kelvin RuslimNo ratings yet
- Chen2020 Article ADiagnosticModelForCoronavirusDocument10 pagesChen2020 Article ADiagnosticModelForCoronavirusPier Cedron LescanoNo ratings yet
- Medicine: Chest CT of COVID-19 in Patients With A Negative First RT-PCR TestDocument8 pagesMedicine: Chest CT of COVID-19 in Patients With A Negative First RT-PCR TestFernando CarrilloNo ratings yet
- XmdffaDocument5 pagesXmdffaIndira LarasatiNo ratings yet
- Pediatric Covid XrayDocument6 pagesPediatric Covid XrayShinta FrennandaNo ratings yet
- Radiological Evaluation and Correlation of CT Chest With Progress of Disease in Covid 19 PatientsDocument14 pagesRadiological Evaluation and Correlation of CT Chest With Progress of Disease in Covid 19 PatientsIJAR JOURNALNo ratings yet
- Radiol 2020200642Document9 pagesRadiol 2020200642sanya eusebia lupaca lupacaNo ratings yet
- Is HRCT Reliable in Determining Disease Activity in Pulmonary Tuberculosis?"Document0 pagesIs HRCT Reliable in Determining Disease Activity in Pulmonary Tuberculosis?"Seftiana SaftariNo ratings yet
- Chest CT in COVID-19 Pneumonia: What Are The Findings in Mid-Term Follow-Up?Document9 pagesChest CT in COVID-19 Pneumonia: What Are The Findings in Mid-Term Follow-Up?rishaNo ratings yet
- BJR 20200219Document9 pagesBJR 20200219WilsonR.CorzoNiñoNo ratings yet
- Evaluation of Covid-19 Pneumonia by Conventional Radiographyat Agmc & GBP HospitalDocument8 pagesEvaluation of Covid-19 Pneumonia by Conventional Radiographyat Agmc & GBP HospitalIJAR JOURNALNo ratings yet
- The British Rhinology Society National COVID-19 Study Resuming Elective SurgeryDocument13 pagesThe British Rhinology Society National COVID-19 Study Resuming Elective Surgeryahmed_ateegNo ratings yet
- Clinical Microbiology and Infection: Research NoteDocument4 pagesClinical Microbiology and Infection: Research NoteNoorNo ratings yet
- Faen ZhangDocument6 pagesFaen ZhangAlejandro TurnerNo ratings yet
- LC PDFDocument10 pagesLC PDFJorge Andres Balza GranadosNo ratings yet
- Radiological Features of AIDS-related Pneumocystis Jiroveci InfectionDocument3 pagesRadiological Features of AIDS-related Pneumocystis Jiroveci InfectionJavi MontañoNo ratings yet
- Prognostic Role of HPV Integration Status and Molecular Profile in Advanced Anal Carcinoma: An Ancillary Study To The epitopes-HPV02 TrialDocument13 pagesPrognostic Role of HPV Integration Status and Molecular Profile in Advanced Anal Carcinoma: An Ancillary Study To The epitopes-HPV02 TrialStefano KimNo ratings yet
- Jurnal BEDocument6 pagesJurnal BEM Ali AdrianNo ratings yet
- Jurnal 20Document5 pagesJurnal 20Ahmad Fari Arief LopaNo ratings yet
- COVID 19 RadiologyDocument29 pagesCOVID 19 RadiologyДоржготов АриунболдNo ratings yet
- Abstracts of The 4th Congress of ECCO The European Crohn's and Colitis Organisation S33Document2 pagesAbstracts of The 4th Congress of ECCO The European Crohn's and Colitis Organisation S33Сергей СадовниковNo ratings yet
- Tuberculous Pleural Effusion in ChildrenDocument5 pagesTuberculous Pleural Effusion in ChildrenAnnisa SasaNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- Vaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyDocument7 pagesVaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyFlor ZalazarNo ratings yet
- Journal ReadingDocument7 pagesJournal ReadingTheresa JulietNo ratings yet
- Indiscriminate Use of CT Chest Imaging During TheDocument2 pagesIndiscriminate Use of CT Chest Imaging During TheRaudha Dani RahmalisaNo ratings yet
- Utility of Chest Radiograph Severity Scoring in Emergency Department For Predicting Outcomes in COVID-19 - A Study of 1275 PatientsDocument7 pagesUtility of Chest Radiograph Severity Scoring in Emergency Department For Predicting Outcomes in COVID-19 - A Study of 1275 PatientsimaragisellaNo ratings yet
- CO-RADS: A Categorical CT Assessment Scheme For Patients Suspected of Having COVID-19-Definition and EvaluationDocument8 pagesCO-RADS: A Categorical CT Assessment Scheme For Patients Suspected of Having COVID-19-Definition and EvaluationrishaNo ratings yet
- Juridng Obs InggrisDocument6 pagesJuridng Obs InggristiaranindyNo ratings yet
- A Profile of Cervical Cancer Cases in A Government Medical College HospitalDocument6 pagesA Profile of Cervical Cancer Cases in A Government Medical College HospitalIOSRjournalNo ratings yet
- Early Recurrence of Carcinoma Gall Bladder After R0 Resection of Stage T1B-T3Document6 pagesEarly Recurrence of Carcinoma Gall Bladder After R0 Resection of Stage T1B-T3IJAR JOURNALNo ratings yet
- Clinico-Radiological Co-Relation of Carcinoma Larynx and Hypopharynx: A Prospective StudyDocument7 pagesClinico-Radiological Co-Relation of Carcinoma Larynx and Hypopharynx: A Prospective StudyDede MarizalNo ratings yet
- The Appropriate Use of Testing For COVID-19Document4 pagesThe Appropriate Use of Testing For COVID-19newazNo ratings yet
- Jurnal Prognosis Radiologi 1Document9 pagesJurnal Prognosis Radiologi 1Henry WijayaNo ratings yet
- Role of Chest X-Ray in Predicting Outcome of Acute Severe PneumoniaDocument6 pagesRole of Chest X-Ray in Predicting Outcome of Acute Severe PneumoniaNurul AprilianiNo ratings yet
- Radiol 2020201754Document10 pagesRadiol 2020201754Rila RivandaNo ratings yet
- International Journal of Infectious Diseases: SciencedirectDocument7 pagesInternational Journal of Infectious Diseases: SciencedirectKinja NinjaNo ratings yet
- A Study of Correlation Between Chest HRCT Score With CT Values of RT-PCR Testing For Covid-19 InfectionDocument4 pagesA Study of Correlation Between Chest HRCT Score With CT Values of RT-PCR Testing For Covid-19 InfectionIJAR JOURNALNo ratings yet
- Boursiani 2017Document5 pagesBoursiani 2017Carlos Urkieta MonetaNo ratings yet
- Imaging Profile of The COVID-19 Infection: Radiologic Findings and Literature ReviewDocument9 pagesImaging Profile of The COVID-19 Infection: Radiologic Findings and Literature ReviewHielmy Auliya HasyimNo ratings yet
- TID 9999 E13413Document5 pagesTID 9999 E13413saraabolghasemi1No ratings yet
- Radiology - Letter Warning of CT False Negative Rate in COVID-YangDocument3 pagesRadiology - Letter Warning of CT False Negative Rate in COVID-YangRemigius RiyanNo ratings yet
- Imaging of the Liver and Intra-hepatic Biliary Tract: Volume 2: Tumoral PathologiesFrom EverandImaging of the Liver and Intra-hepatic Biliary Tract: Volume 2: Tumoral PathologiesNo ratings yet
- Position Paper ZABATEDocument20 pagesPosition Paper ZABATEAtty. Emmanuel SandichoNo ratings yet
- Bilal Ahmad Khan CVDocument2 pagesBilal Ahmad Khan CVfr.faisal8265No ratings yet
- A Study of Work Life Balance of Female Employee With Refrence To HDFC Bank at MoradabadDocument72 pagesA Study of Work Life Balance of Female Employee With Refrence To HDFC Bank at MoradabadbuddysmbdNo ratings yet
- 3) Z. 10.1016@j.jcrc.2020.06.005 (Alexis Tabah)Document18 pages3) Z. 10.1016@j.jcrc.2020.06.005 (Alexis Tabah)Mastifa HanasitaNo ratings yet
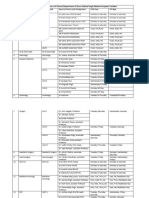
- OPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalDocument4 pagesOPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalBohar singh Brar BrarNo ratings yet
- Anatomi Dan Fisiologi PerkemihanDocument89 pagesAnatomi Dan Fisiologi Perkemihannia djNo ratings yet
- GIT InfectionDocument43 pagesGIT InfectionRaja RuzannaNo ratings yet
- MCQ in OphthalmologyDocument108 pagesMCQ in OphthalmologySushi HtetNo ratings yet
- Synthesis of The Work of Enderlein, Etc PDFDocument3 pagesSynthesis of The Work of Enderlein, Etc PDFpaulxe100% (1)
- Project ReportDocument27 pagesProject Reportniladri mondalNo ratings yet
- Department of Labor: Bct-Fy01Document101 pagesDepartment of Labor: Bct-Fy01USA_DepartmentOfLabor100% (1)
- B. VinothDocument5 pagesB. VinothBilal HassanNo ratings yet
- Written Report Abnormal PsychologyDocument23 pagesWritten Report Abnormal PsychologyCy Esquibel LingaNo ratings yet
- Oral IronDocument72 pagesOral IronKishore ChandkiNo ratings yet
- Qdoc - Tips - Prometric Practice Exam For Nurses Test 1Document6 pagesQdoc - Tips - Prometric Practice Exam For Nurses Test 1Ponnudev100% (1)
- Soal Inggris - 2Document6 pagesSoal Inggris - 2vivitrisami05No ratings yet
- Substance AbuseDocument54 pagesSubstance AbuseCharles CastilloNo ratings yet
- June 2008Document17 pagesJune 2008proxy1589No ratings yet
- Bod+cod Statistici MARSDocument16 pagesBod+cod Statistici MARSandreiNo ratings yet
- Closed PTW AuditDocument1 pageClosed PTW Auditf.BNo ratings yet
- 5 1 Why Your Body Needs NutrientsDocument3 pages5 1 Why Your Body Needs Nutrientsapi-261782961No ratings yet
- Celebrating Worthing College 2012 SpeadsDocument9 pagesCelebrating Worthing College 2012 SpeadsWorthing College-SportNo ratings yet
- Purine Rich FoodDocument3 pagesPurine Rich Foodttstanescu4506No ratings yet
- Thorax and Lungs Physical Assessment Includes InspectionDocument9 pagesThorax and Lungs Physical Assessment Includes InspectionwiwinNo ratings yet
- Readings On Human Development of NepalDocument310 pagesReadings On Human Development of NepalBirkha B PunNo ratings yet
- Rose Doe v. The City of New York, Et. Al.Document57 pagesRose Doe v. The City of New York, Et. Al.Daily Caller News FoundationNo ratings yet
- New Lipid PowerpointDocument113 pagesNew Lipid PowerpointMadane Jamila Amerol SaminNo ratings yet
- Shiva LatestDocument3 pagesShiva LatestToby JordanNo ratings yet
- Medical Condition Report Free PDF TemplateDocument2 pagesMedical Condition Report Free PDF Templateapi-340236228No ratings yet