Download as pdf or txt
You might also like
- NeralDocument9 pagesNeralmmNo ratings yet
- Syncope Dr. Adrian RIzal PKB 2019Document39 pagesSyncope Dr. Adrian RIzal PKB 2019Fandy Hazzy AlfataNo ratings yet
- 2018 Slides Bradycardia and Cardiac Conduction DelayDocument108 pages2018 Slides Bradycardia and Cardiac Conduction Delayalyn100% (1)
- Management of Malignant Ventricular Arrhytmia - Dr. Achmad LefiDocument32 pagesManagement of Malignant Ventricular Arrhytmia - Dr. Achmad LefiStanley GunawanNo ratings yet
- 1 See Table On Inside Front CoverDocument1 page1 See Table On Inside Front CoverRajendra KunwarNo ratings yet
- BradyarrhythimasDocument61 pagesBradyarrhythimasMhmd A LubadNo ratings yet
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDocument4 pagesLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testNo ratings yet
- Cardiac - Vascular Ultrasonic Scanning SystemsDocument54 pagesCardiac - Vascular Ultrasonic Scanning SystemsGino F. Musso SavageNo ratings yet
- Echo ReportDocument2 pagesEcho ReportweareweNo ratings yet
- ECG - Rhythms - For - ACLS - 201309101532569240 Pages 276, 277Document2 pagesECG - Rhythms - For - ACLS - 201309101532569240 Pages 276, 277Mike GNo ratings yet
- Mechanism and Management ArrhythmiasDocument56 pagesMechanism and Management ArrhythmiasMochamad Rizky HendiperdanaNo ratings yet
- Permanent PacemakerDocument23 pagesPermanent PacemakeradinsNo ratings yet
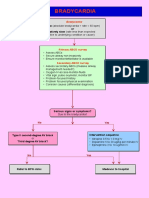
- BradycardiaDocument1 pageBradycardiaVeranika SelviyaNo ratings yet
- Syncope: DR - Hardja Priatna, SPJP, Fiha 26 Februari 2018Document77 pagesSyncope: DR - Hardja Priatna, SPJP, Fiha 26 Februari 2018pkm cibodasariNo ratings yet
- SVT Guideline UpdateDocument20 pagesSVT Guideline UpdateMarianneAiraFalsisPaedNo ratings yet
- Code BlueDocument26 pagesCode BlueJenny CandraNo ratings yet
- Warning: Learners, Please Complete The Learner Survey (Ucalgary - Ca/Codeblue/Surveys) Before Viewing This PowerpointDocument27 pagesWarning: Learners, Please Complete The Learner Survey (Ucalgary - Ca/Codeblue/Surveys) Before Viewing This PowerpointHandrian RahmanNo ratings yet
- Seizure Bam PDFDocument1 pageSeizure Bam PDFJames eullaranNo ratings yet
- Second Degree Av Block Type 1 (Mobitz I or Wenckebach)Document1 pageSecond Degree Av Block Type 1 (Mobitz I or Wenckebach)christine louise bernardoNo ratings yet
- Fellowship Application Deadlines 2022 2023Document2 pagesFellowship Application Deadlines 2022 2023Kutu MiaNo ratings yet
- Acute Coronary Syndrome: History and Clinical Assessment Suggest ACSDocument12 pagesAcute Coronary Syndrome: History and Clinical Assessment Suggest ACSginongNo ratings yet
- NIC Registry Proforma-2010Document7 pagesNIC Registry Proforma-2010Cardiovascular TechnologistsNo ratings yet
- Bradycardia and TachycardiaDocument66 pagesBradycardia and TachycardiaKarissaNo ratings yet
- Cardiology 2023 FinalDocument208 pagesCardiology 2023 FinalBelinda ELISHA100% (1)
- Stress Eco and Eco ReportDocument4 pagesStress Eco and Eco ReportguptarichaandassociatesNo ratings yet
- Borang Pemeriksaan-Mammografi 1Document2 pagesBorang Pemeriksaan-Mammografi 1hsentosaoshNo ratings yet
- Persiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairDocument5 pagesPersiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairYanis Widhiya NingrumNo ratings yet
- K31a - Electrophysiology and Cardiac Arrhytmia EmergencyDocument46 pagesK31a - Electrophysiology and Cardiac Arrhytmia EmergencyXeniel AlastairNo ratings yet
- Spesifikasi Acuson P500Document2 pagesSpesifikasi Acuson P500KurniaBagusNo ratings yet
- 主流几大SPECT-CT 制造商系统参数比较Document6 pages主流几大SPECT-CT 制造商系统参数比较AnguschowNo ratings yet
- Nursing CS Treatment-Of-Atrial-Dysrhythmias 02Document1 pageNursing CS Treatment-Of-Atrial-Dysrhythmias 02frankshro156No ratings yet
- Classification of StrokeDocument7 pagesClassification of StrokeSiti Fairuz NadyaNo ratings yet
- Algoritmo Fiebre de Origen DesconocidoDocument1 pageAlgoritmo Fiebre de Origen Desconocidoluisa gonzálezNo ratings yet
- Needlestick Reporting Monitoring FormDocument5 pagesNeedlestick Reporting Monitoring Formnseducation.mahgNo ratings yet
- Cardiac Arrest Algorithm: Give OxygenDocument2 pagesCardiac Arrest Algorithm: Give OxygenJunius SimarmataNo ratings yet
- VT Ventricular TachyDocument1 pageVT Ventricular Tachymadimadi11No ratings yet
- OHQ NewsLetter - Vol12 - Afib - 1112 - ENDocument5 pagesOHQ NewsLetter - Vol12 - Afib - 1112 - ENherryaptNo ratings yet
- L1 Report TemplateDocument2 pagesL1 Report TemplateRasangi Sumudu Clare SuraweeraNo ratings yet
- Primary Viva Examination: Thursday 31 October 2019Document1 pagePrimary Viva Examination: Thursday 31 October 2019Deliberate self harmNo ratings yet
- Sample Patient Care Report: Name: Date: Sex: M F Time: AddressDocument4 pagesSample Patient Care Report: Name: Date: Sex: M F Time: AddressBCF PRODUCTIONNo ratings yet
- Elektrokardiografi & Kegawatan AritmiaDocument62 pagesElektrokardiografi & Kegawatan AritmiaNindy OktaviyaniNo ratings yet
- NO 11 - NO 11 - Bradycardia and Heart Block (23 August 2011)Document28 pagesNO 11 - NO 11 - Bradycardia and Heart Block (23 August 2011)Ni'matul Muthmainnah SyariefNo ratings yet
- STEMI Algorithm Poster 18x24Document1 pageSTEMI Algorithm Poster 18x24OgizWaraNo ratings yet
- Clinical Guideline: Fibrinolytic Checklist Fibrinolytic ChecklistDocument4 pagesClinical Guideline: Fibrinolytic Checklist Fibrinolytic ChecklistRoi LevinzonNo ratings yet
- NCM 101-GenogramDocument1 pageNCM 101-GenogramCarolyn Moquerio-serniculaNo ratings yet
- DR Fadillah Maricar, SPJP Angina Pectoris Dan Infark MiokardDocument50 pagesDR Fadillah Maricar, SPJP Angina Pectoris Dan Infark MiokardMuhaswadNo ratings yet
- 7 Spesifikasi USG Acuson S1000 USG Obgyn 4D UltraPremium W 3 Probes FINAL PDFDocument95 pages7 Spesifikasi USG Acuson S1000 USG Obgyn 4D UltraPremium W 3 Probes FINAL PDFipungNo ratings yet
- 4 Atrioventricular Block Decision TreeDocument1 page4 Atrioventricular Block Decision TreeAndrea LunaNo ratings yet
- Presentasi Code Blue IGDDocument16 pagesPresentasi Code Blue IGDIgd Pondok TjandraNo ratings yet
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikNo ratings yet
- Audiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowDocument3 pagesAudiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowHarshit AmbeshNo ratings yet
- Adult Cardiac Arrest AlgoritmaDocument1 pageAdult Cardiac Arrest AlgoritmaYouniehacibie Ichisky ChildNo ratings yet
- CP HivDocument2 pagesCP Hivmelania sea kedangNo ratings yet
- Anatomy 2Document2 pagesAnatomy 2Ahmed AdelNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- Arteriovenous Malformation 1001Document19 pagesArteriovenous Malformation 1001housic1No ratings yet
- Spec Compare DP20T and KemenkesDocument4 pagesSpec Compare DP20T and KemenkesRiyandNo ratings yet
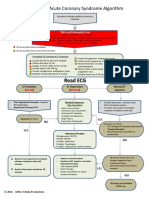
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- Integrated Pest Management For Corn (Zea MaysDocument21 pagesIntegrated Pest Management For Corn (Zea MayscholzNo ratings yet
- United States Patent (10) Patent No.: US 9,024.815 B2Document13 pagesUnited States Patent (10) Patent No.: US 9,024.815 B2Daniela ScobarNo ratings yet
- Study Guide: Kawabata Yasunari "Pomegranate" (Zakuro)Document8 pagesStudy Guide: Kawabata Yasunari "Pomegranate" (Zakuro)Beholdmyswarthyface75% (4)
- The Rotator Cuff (Myofascial Techniques)Document4 pagesThe Rotator Cuff (Myofascial Techniques)Advanced-Trainings.com100% (3)
- Critical Functions & Design Criteria For Geogrids Used in Reinforced Aggregate Raft Foundations For Christchurch Rebuilt - Jan 2013Document4 pagesCritical Functions & Design Criteria For Geogrids Used in Reinforced Aggregate Raft Foundations For Christchurch Rebuilt - Jan 2013Victor WongNo ratings yet
- Implementation of 5S Practices in The Manufacturing Companies: A Case StudyDocument8 pagesImplementation of 5S Practices in The Manufacturing Companies: A Case StudyrscyuzonNo ratings yet
- MR - Mentoring EE Educators Towards PEEEngr. Cirilo Calibjo Nov. 27 2015Document74 pagesMR - Mentoring EE Educators Towards PEEEngr. Cirilo Calibjo Nov. 27 2015ramelNo ratings yet
- Acknowledgement: ReferencesDocument7 pagesAcknowledgement: Referencesdwayne420No ratings yet
- SM 25Document144 pagesSM 25Jan Svein HammerNo ratings yet
- Kenwood B62-2299-20Document2 pagesKenwood B62-2299-20King MaxNo ratings yet
- Expt-1 Lab Manual TE LabDocument6 pagesExpt-1 Lab Manual TE LabFariha Rahman NameerahNo ratings yet
- Nipro Trueresult ManualDocument82 pagesNipro Trueresult Manualfeliperm41No ratings yet
- As Referenced by ASME B20.1 For Use in Conjunction With That StandardDocument26 pagesAs Referenced by ASME B20.1 For Use in Conjunction With That StandardimazaxNo ratings yet
- REX012832GYAP3N0Document28 pagesREX012832GYAP3N0marius.chitigaNo ratings yet
- Phytosome: Presented byDocument14 pagesPhytosome: Presented bySari RamadhaniNo ratings yet
- Categorical PropositionsDocument5 pagesCategorical PropositionsStephanie Reyes GoNo ratings yet
- Alberts-Chapter 11-Membrane TransportDocument44 pagesAlberts-Chapter 11-Membrane TransportMayra SanchezNo ratings yet
- Kitchen SAfety Power Point ComDocument38 pagesKitchen SAfety Power Point CombibubhaskarNo ratings yet
- Guardian Chapter 6Document4 pagesGuardian Chapter 6ME-06-Ahiri SahaNo ratings yet
- A Wanderer in Holland by Lucas, E. V. (Edward Verrall), 1868-1938Document251 pagesA Wanderer in Holland by Lucas, E. V. (Edward Verrall), 1868-1938Gutenberg.orgNo ratings yet
- Power 1 1Document11 pagesPower 1 1stevens001100% (1)
- Batate Batani GashiDocument2 pagesBatate Batani Gashirutik vaidyaNo ratings yet
- EME PPT Unit-5 - ElectiveDocument37 pagesEME PPT Unit-5 - ElectivesudeepkoreaNo ratings yet
- The Oxford Handbook of Time in Music (Oxford Handbooks)Document556 pagesThe Oxford Handbook of Time in Music (Oxford Handbooks)yi luNo ratings yet
- 971 Japanese Company in MalaysiaDocument278 pages971 Japanese Company in MalaysiaWan HazlizamNo ratings yet
- Snell Manuscript (Keelys Secrets)Document5 pagesSnell Manuscript (Keelys Secrets)Gregg Martin100% (2)
- Outline and Critically Evaluate The Classical Conditioning Explanation of Phobias. How Have Such Explanations Influenced The Treatment of These Conditions?Document4 pagesOutline and Critically Evaluate The Classical Conditioning Explanation of Phobias. How Have Such Explanations Influenced The Treatment of These Conditions?AlineMola100% (1)
- Electric and Hybrid Electric VehiclesDocument16 pagesElectric and Hybrid Electric Vehiclessree haritha p100% (1)
- NTC 220 - 50 Manual Rev00Document57 pagesNTC 220 - 50 Manual Rev00Xuân NHNo ratings yet
- NTU-JTC I3C Seminar (02!8!2012) SlidesDocument24 pagesNTU-JTC I3C Seminar (02!8!2012) SlidesChua Chim HueeNo ratings yet