Download as docx, pdf, or txt
You might also like
- OSTEORADIONECROSISDocument38 pagesOSTEORADIONECROSISAbel AbrahamNo ratings yet
- Trisomy 21Document17 pagesTrisomy 21Paul Michael BaguhinNo ratings yet
- Case Study Julies BakeshopDocument3 pagesCase Study Julies BakeshopKristel Anne AquinoNo ratings yet
- Fundamentals of Nursing PDFDocument18 pagesFundamentals of Nursing PDFJamaica Manuel Iglesias100% (6)
- MPI Painting CodeDocument28 pagesMPI Painting CodeGhayas JawedNo ratings yet
- Trisomy 13, 18Document7 pagesTrisomy 13, 18Maria Donabella OngueNo ratings yet
- 7 Down SyndromeDocument5 pages7 Down SyndromeAdnan RezaNo ratings yet
- Down SyndromeDocument26 pagesDown SyndromeJerralyn GarciaNo ratings yet
- AneuploidyDocument4 pagesAneuploidyTingal, Jaynore C.No ratings yet
- Practicum 1 ReportDocument8 pagesPracticum 1 ReportRazan NasereddineNo ratings yet
- Down Syndrome What Is Down Syndrome?Document4 pagesDown Syndrome What Is Down Syndrome?Vanessa Rose NoelNo ratings yet
- What Is Down Syndrom1Document5 pagesWhat Is Down Syndrom1Mis JassNo ratings yet
- Down Syndrom (Eng)Document11 pagesDown Syndrom (Eng)Echa MagungNo ratings yet
- Down SyndromeDocument19 pagesDown SyndromeRiya LalchandaniNo ratings yet
- SCI-Down SyndromeDocument1 pageSCI-Down SyndromeCharleson Kurt OngNo ratings yet
- Noninvasive Prenatal Testing For Down Syndrome and Other TrisomiesDocument21 pagesNoninvasive Prenatal Testing For Down Syndrome and Other TrisomiesrpbpaNo ratings yet
- Research Paper On Down Syndrome OutlineDocument5 pagesResearch Paper On Down Syndrome Outlinehumin1byjig2100% (1)
- Down Syndrome Overview 1120407 PDFDocument6 pagesDown Syndrome Overview 1120407 PDFHartotok VipnetNo ratings yet
- Trisomy 18 (Edward) and Trisomy 13 (Patau) - Frequently Asked QuestionsDocument3 pagesTrisomy 18 (Edward) and Trisomy 13 (Patau) - Frequently Asked QuestionsNinaNo ratings yet
- What Is Down Syndrome?Document14 pagesWhat Is Down Syndrome?DrEx GUy WadasenNo ratings yet
- Downs SyndromeDocument5 pagesDowns Syndromeapi-243318982No ratings yet
- What Is Down Syndrome What Causes Down SyndromeDocument4 pagesWhat Is Down Syndrome What Causes Down Syndromeapi-243322010No ratings yet
- Birth Defects Ratio: Gene ChromosomeDocument6 pagesBirth Defects Ratio: Gene Chromosomeapi-26413035No ratings yet
- Down SyndromeDocument74 pagesDown Syndromeanumeha sharma100% (2)
- SYNDROMEDocument4 pagesSYNDROMEDavid AbadianoNo ratings yet
- Down SyndromeDocument4 pagesDown SyndromeSudeNo ratings yet
- Sem1 Down SyndromeeeDocument5 pagesSem1 Down SyndromeeeRomina ReidNo ratings yet
- What Is Down SyndromeDocument4 pagesWhat Is Down SyndromeJanica GonzalesNo ratings yet
- Down Screen Proposal For Health Screen at Thyrocare AmitDocument19 pagesDown Screen Proposal For Health Screen at Thyrocare AmitSwatiSuranaNo ratings yet
- Down SyndromeDocument14 pagesDown SyndromeamitharaoNo ratings yet
- Research Paper Topics On Down SyndromeDocument4 pagesResearch Paper Topics On Down Syndrometkpmzasif100% (1)
- Down Syndrome Description Down Syndrome Is A Chromosomal Condition That Is Associated With Intellectual DisabilityDocument2 pagesDown Syndrome Description Down Syndrome Is A Chromosomal Condition That Is Associated With Intellectual Disabilityreyyann369No ratings yet
- Genbio-Meiosis and MitosisDocument6 pagesGenbio-Meiosis and MitosisAlexandra AlbueroNo ratings yet
- GENBIODocument6 pagesGENBIOAlexandra AlbueroNo ratings yet
- Down Syndrome Article 1Document3 pagesDown Syndrome Article 1api-252032417No ratings yet
- DiseasesDocument2 pagesDiseasesMikaela EuniceNo ratings yet
- Trisomy/ Down SyndromeDocument2 pagesTrisomy/ Down SyndromeDanah Grace SanchezNo ratings yet
- Biology Genetics Disorder By: Group A 1. 2. 3. 4. 5Document21 pagesBiology Genetics Disorder By: Group A 1. 2. 3. 4. 5JawadNo ratings yet
- Sindrome de DownDocument27 pagesSindrome de DownKhissi BArzaNo ratings yet
- Downsyndrome 230411172734 b6391831Document32 pagesDownsyndrome 230411172734 b6391831dattamanasmita90No ratings yet
- Brief Description Down Syndrome A. DescriptionDocument4 pagesBrief Description Down Syndrome A. DescriptionJohn Rey AbadNo ratings yet
- Karyotyping Learning OutcomesDocument3 pagesKaryotyping Learning OutcomesALOIZA BELLE LAVI�ANo ratings yet
- Down's, Edward's and Patau's SyndromeDocument6 pagesDown's, Edward's and Patau's SyndromeДанина НиколоваNo ratings yet
- Down Syndrome PresentationDocument43 pagesDown Syndrome Presentationapi-509245925No ratings yet
- DocumentDocument11 pagesDocumentStephanie BolañosNo ratings yet
- Chromosome 18 - 094757Document4 pagesChromosome 18 - 094757Shann Angel MarciaNo ratings yet
- Down Syndrome: Current Status, Challenges and Future PerspectivesDocument5 pagesDown Syndrome: Current Status, Challenges and Future PerspectivesAljusufal Ali Moh. Ali100% (1)
- Patau Syndrome1Document5 pagesPatau Syndrome1api-346355246No ratings yet
- Down SyndromeDocument8 pagesDown SyndromeCozma IonutNo ratings yet
- Down SyndromeDocument5 pagesDown SyndromeBravo BNo ratings yet
- Research Paper Down SyndromeDocument5 pagesResearch Paper Down Syndromeafnkjdhxlewftq100% (1)
- Research Paper 1Document3 pagesResearch Paper 1api-643573791No ratings yet
- Research Paper On Down Syndrome PDFDocument6 pagesResearch Paper On Down Syndrome PDFfzkk43h9100% (1)
- Dawn, Patau and Turner SyndromeDocument10 pagesDawn, Patau and Turner Syndromemdaminulislam71469No ratings yet
- CBL 2 HistoDocument4 pagesCBL 2 Histodrahmed1028No ratings yet
- Down SyndromeDocument3 pagesDown SyndromeMargie Ballesteros Manzano100% (1)
- Pre-Reading Genetics DisordersDocument10 pagesPre-Reading Genetics DisordersMya Phone MohNo ratings yet
- CASEDocument119 pagesCASEGwenn SalazarNo ratings yet
- Down Syndrome: by Mayo Clinic StaffDocument5 pagesDown Syndrome: by Mayo Clinic Staffextramarital_manNo ratings yet
- Bab I Pendahuluan: A. Latar BelakangDocument10 pagesBab I Pendahuluan: A. Latar BelakangOkke KriswidiantoNo ratings yet
- Chromosomal AbnormalitiesDocument29 pagesChromosomal AbnormalitiesdickyNo ratings yet
- Research Paper of Down SyndromeDocument7 pagesResearch Paper of Down Syndromegw13qds8100% (1)
- Clinical Vignette 1Document9 pagesClinical Vignette 1Joanne Alyssa Hernandez LascanoNo ratings yet
- Use of AI in Medicinal Product Lifecycle 1689684121Document17 pagesUse of AI in Medicinal Product Lifecycle 1689684121vivek rakhaNo ratings yet
- G10 1st PERIODICAL TEST MAPEH10 TQDocument5 pagesG10 1st PERIODICAL TEST MAPEH10 TQMaricel LajeraNo ratings yet
- Catálogo de Referencias - Power Conversion SystemsDocument60 pagesCatálogo de Referencias - Power Conversion SystemsBENo ratings yet
- Artificial Intelligence in PharmacyDocument8 pagesArtificial Intelligence in PharmacyMeraNo ratings yet
- Ethics in HRMDocument7 pagesEthics in HRMVinay RamaneNo ratings yet
- The History of The Big Bang TheoryDocument6 pagesThe History of The Big Bang Theorymay ann dimaanoNo ratings yet
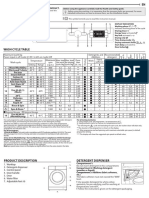
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Lecture 4Document22 pagesLecture 4SUNDAS FATIMANo ratings yet
- (U) Daily Activity Report: Marshall DistrictDocument5 pages(U) Daily Activity Report: Marshall DistrictFauquier NowNo ratings yet
- Model ETR-9200 Automatic Tuning Smarter Logic ControllerDocument26 pagesModel ETR-9200 Automatic Tuning Smarter Logic ControllervhelectronicaNo ratings yet
- Soil Acidity and LimingDocument12 pagesSoil Acidity and LimingEloi Carlos GoveNo ratings yet
- IPC in Family PlanningDocument12 pagesIPC in Family PlanningHari MurtiNo ratings yet
- Chemistry Project 2021-2022Document19 pagesChemistry Project 2021-2022Rudra SathwaraNo ratings yet
- Cylone - Lab Report - FinalizeDocument19 pagesCylone - Lab Report - FinalizeSiti Khairunnur LaderlahNo ratings yet
- John White Videos of Spooky2 InterfaceDocument24 pagesJohn White Videos of Spooky2 InterfaceTimothy M HallNo ratings yet
- Maintain Training Facilities: Submitted By: Aeron M. LumbaDocument10 pagesMaintain Training Facilities: Submitted By: Aeron M. LumbaAeron LumbaNo ratings yet
- 1 Case IDC PDFDocument7 pages1 Case IDC PDFPilar Dueñas Maldonado0% (1)
- Acceptance Criteria of Weld Defects As Per Different CodesDocument17 pagesAcceptance Criteria of Weld Defects As Per Different CodesMidhun K Chandrabose96% (25)
- Developments in The Internal Dosimetry of Radiopharmaceuticals.Document6 pagesDevelopments in The Internal Dosimetry of Radiopharmaceuticals.Edis ĐedovićNo ratings yet
- Economics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Document8 pagesEconomics 9732/01: Pioneer Junior College, Singapore Preliminary Examinations 2014 Higher 2Yvette LimNo ratings yet
- The AwakeningDocument4 pagesThe AwakeningRIMMA DATILESNo ratings yet
- DPP 02 NTSE BY @class - 10 - MaterialsDocument1 pageDPP 02 NTSE BY @class - 10 - MaterialsShashwat MishraNo ratings yet
- Generator Automatic Voltage Regulator Operation ManualDocument6 pagesGenerator Automatic Voltage Regulator Operation ManualMahdi DehghankarNo ratings yet
- Module 7: Health Care Delivery SystemDocument9 pagesModule 7: Health Care Delivery SystemDanz KieNo ratings yet
- Crew Habitability On Mobile Offshore Drilling Units (Modus) : Guide ForDocument87 pagesCrew Habitability On Mobile Offshore Drilling Units (Modus) : Guide ForReza BabriNo ratings yet
- The Winnipeg Foundation 2014 Annual ReportDocument76 pagesThe Winnipeg Foundation 2014 Annual ReportChrisDcaNo ratings yet