Download as pdf or txt
You might also like
- Practice Toeic Reading Test 2021 03 - Tests + AnswerDocument19 pagesPractice Toeic Reading Test 2021 03 - Tests + AnswerAVRILLIA CLEMENTINENo ratings yet
- Social Factors Affecting Educational PlanningDocument9 pagesSocial Factors Affecting Educational PlanningShaayongo Benjamin50% (2)
- DSF Ohada English VersionDocument44 pagesDSF Ohada English VersionNana Abdoulbagui100% (1)
- Invoice: P.T.Evergreen Shipping Agency IndonesiaDocument1 pageInvoice: P.T.Evergreen Shipping Agency IndonesiaDody DermawanNo ratings yet
- InterSchool Activity ScriptDocument7 pagesInterSchool Activity ScriptJessica Loren Leyco87% (15)
- ARTICULO - Daño EPP en La Piel COVID de Los Trabajadores Que Gsestionan La Salud - AcadDocument2 pagesARTICULO - Daño EPP en La Piel COVID de Los Trabajadores Que Gsestionan La Salud - AcadDieter Fernando Sejas LópezNo ratings yet
- 10 1001@jama 2020 9843Document2 pages10 1001@jama 2020 9843Joko Arif KurniawanNo ratings yet
- MaskneDocument5 pagesMaskneyuliNo ratings yet
- 668-Article Text-1030-1-10-20181101Document4 pages668-Article Text-1030-1-10-20181101burhanNo ratings yet
- Association Between Exposure Characteristics and The Risk For COVID-19 Infection Among Health Care Workers With and Without BNT162b2 VaccinationDocument4 pagesAssociation Between Exposure Characteristics and The Risk For COVID-19 Infection Among Health Care Workers With and Without BNT162b2 VaccinationChristian GaraffaNo ratings yet
- High-Dose Spironolactone For Acne in Patients With Polycystic Ovarian Syndrome - A Single-Institution Retrospective StudyDocument2 pagesHigh-Dose Spironolactone For Acne in Patients With Polycystic Ovarian Syndrome - A Single-Institution Retrospective StudyDaniella TruffelloNo ratings yet
- Effect of Seamless Nursing For Complications On Cataract PatientsDocument3 pagesEffect of Seamless Nursing For Complications On Cataract Patientsnila choirun nailiNo ratings yet
- DapusDocument4 pagesDapusZulfiana RahayuNo ratings yet
- CE (Ra1) F (IS) PF1 (HB KM) PN (KM)Document4 pagesCE (Ra1) F (IS) PF1 (HB KM) PN (KM)Mihir ShahNo ratings yet
- Ijo 11 01 043Document5 pagesIjo 11 01 043bellaNo ratings yet
- PIIS0140673620311831Document2 pagesPIIS0140673620311831kayegi8666No ratings yet
- Esicm Lives 2018: Meetingabstracts Open AccessDocument690 pagesEsicm Lives 2018: Meetingabstracts Open AccessjasbvbfitnessNo ratings yet
- 10 30621-Jbachs 863206-1516439Document10 pages10 30621-Jbachs 863206-1516439Joao ColomaNo ratings yet
- Comparison of Efficacy of 1% Silver Sulfadiazine and Acticoat For Treatment of Partial-Thickness Burn WoundsDocument6 pagesComparison of Efficacy of 1% Silver Sulfadiazine and Acticoat For Treatment of Partial-Thickness Burn WoundsHusni maiyantiNo ratings yet
- Covid Mask Use For Proffeesionals by JuanDocument9 pagesCovid Mask Use For Proffeesionals by JuanJuanNo ratings yet
- 10 1016@j Jse 2018 11 025Document2 pages10 1016@j Jse 2018 11 025hari vijayNo ratings yet
- Post Traumatic Endophthalmitis: Incidence and Risk FactorsDocument5 pagesPost Traumatic Endophthalmitis: Incidence and Risk FactorsIgnasius HansNo ratings yet
- SYSTEMATIC REVIEW ArticleDocument33 pagesSYSTEMATIC REVIEW ArticleOui AnyNo ratings yet
- Pi Is 0883944116304877Document6 pagesPi Is 0883944116304877mohamad safiiNo ratings yet
- Jcad 8 4 21Document5 pagesJcad 8 4 21Rosyid PrasetyoNo ratings yet
- Psychological Impact of The Covid19 Pandemic Among Health Care Workers in TunisiaDocument6 pagesPsychological Impact of The Covid19 Pandemic Among Health Care Workers in TunisiaMohamed FerhiNo ratings yet
- Topical Formic Acid Puncture Technique For The Treatment of Common WartsDocument6 pagesTopical Formic Acid Puncture Technique For The Treatment of Common WartsAndrea CalderaNo ratings yet
- Fmed 07 594269Document14 pagesFmed 07 594269valmasci group 6No ratings yet
- TELEDERDocument7 pagesTELEDERSajin AlexanderNo ratings yet
- 05 Palmieri-VadalaDocument7 pages05 Palmieri-VadalaSantosNo ratings yet
- Poster Fesbe Sergio MirtesDocument1 pagePoster Fesbe Sergio MirtesMirtes PereiraNo ratings yet
- Study of Factors Associated With Acute PharyngitisDocument4 pagesStudy of Factors Associated With Acute PharyngitisMarsya Yulinesia LoppiesNo ratings yet
- 1 s2.0 S2093791122000919 MainDocument2 pages1 s2.0 S2093791122000919 MainYULIANTONo ratings yet
- The Impact of COVID-19 On Medical Practice: A Nationwide Survey of Dermatologists and Healthcare Providers in IraqDocument32 pagesThe Impact of COVID-19 On Medical Practice: A Nationwide Survey of Dermatologists and Healthcare Providers in Iraqpopov357No ratings yet
- Comparative Study of Two Topical Therapies in Acne - Benzoyl Peroxide (2.5%) & Retinoic Acid (0.025%)Document4 pagesComparative Study of Two Topical Therapies in Acne - Benzoyl Peroxide (2.5%) & Retinoic Acid (0.025%)manish agrawalNo ratings yet
- Sinusitis Paper - 2015Document23 pagesSinusitis Paper - 2015samah hossnyNo ratings yet
- Science of The Total Environment: Kin-Fai Ho, Lian-Yu Lin, Shao-Ping Weng, Kai-Jen ChuangDocument4 pagesScience of The Total Environment: Kin-Fai Ho, Lian-Yu Lin, Shao-Ping Weng, Kai-Jen ChuangBryan Panchana TorresNo ratings yet
- Jcdsa20120300010 79060760Document5 pagesJcdsa20120300010 79060760iqbalNo ratings yet
- 4883-PDF Galley-29565-1-10-20200730Document7 pages4883-PDF Galley-29565-1-10-20200730Irfan HussainNo ratings yet
- Referencia 5Document10 pagesReferencia 5Ulises MattoNo ratings yet
- Effectiveness of Oral Albendazole As A Treatment For Pediculosis CapitisDocument6 pagesEffectiveness of Oral Albendazole As A Treatment For Pediculosis CapitisAlmuizzu NurjannahNo ratings yet
- Mask Acne During Covid19: Case SeriesDocument3 pagesMask Acne During Covid19: Case SeriesIJAR JOURNALNo ratings yet
- Jamainternal Sickbertbennett 2021 LD 210021 1618355295.10569Document2 pagesJamainternal Sickbertbennett 2021 LD 210021 1618355295.10569Febri engahuNo ratings yet
- Quality of Life, Respiratory Symptoms, and Health Care Utilization 1 Year Following Outpatient Management of COVID 19: A Prospective Cohort StudyDocument4 pagesQuality of Life, Respiratory Symptoms, and Health Care Utilization 1 Year Following Outpatient Management of COVID 19: A Prospective Cohort StudyFranklin GuamanNo ratings yet
- Effectiveness of Kumquat Decoction For The Improvement of Cough Caused by SARS-CoV-2 Omicron Variants, A Multicentre, Prospective Observational StudyDocument8 pagesEffectiveness of Kumquat Decoction For The Improvement of Cough Caused by SARS-CoV-2 Omicron Variants, A Multicentre, Prospective Observational StudyCatherina MoszkowiczNo ratings yet
- Perceptions of The COVID-19 Vaccination Among Health-Care Proffesional in DR M Djamil General Hospital PadangDocument5 pagesPerceptions of The COVID-19 Vaccination Among Health-Care Proffesional in DR M Djamil General Hospital PadangmyhalfsmileNo ratings yet
- A59.2.full PosDocument1 pageA59.2.full PosMaharani Adrianto NNo ratings yet
- AkneDocument4 pagesAkneputri.SpANo ratings yet
- Nigella Sativa Oil Lotion 20% vs. Benzoyl Peroxide Lotion 5% in The Treatment of Mild To Moderate Acne VulgarisDocument6 pagesNigella Sativa Oil Lotion 20% vs. Benzoyl Peroxide Lotion 5% in The Treatment of Mild To Moderate Acne VulgarisDita Rahmaika ANo ratings yet
- Scientific Letter: Archivos de Bronconeumología 58 (2022) 520-522Document3 pagesScientific Letter: Archivos de Bronconeumología 58 (2022) 520-522johannaNo ratings yet
- Canadian Dermatology Today Special Supplement An Overview of Jak Inhibitors Fall 2022Document12 pagesCanadian Dermatology Today Special Supplement An Overview of Jak Inhibitors Fall 2022Ron VNo ratings yet
- Awareness of COVID-19 and Perception of Work Satisfaction Among Healthcare Workers at Patan Hospital, NepalDocument6 pagesAwareness of COVID-19 and Perception of Work Satisfaction Among Healthcare Workers at Patan Hospital, NepalViorentina YofianiNo ratings yet
- 1 s2.0 S1879729615001064 MainDocument4 pages1 s2.0 S1879729615001064 MainMarcelo DiasNo ratings yet
- Treatment Data Using A Topical Povidone-Iodine Antiseptic in Patients With Super Ficial Skin AbscessesDocument6 pagesTreatment Data Using A Topical Povidone-Iodine Antiseptic in Patients With Super Ficial Skin AbscessesADENo ratings yet
- A Clinical Study of Intensity-Modulated Radiotherapy-Induced Dry Eye Disease in Head and Neck MalignanciesDocument6 pagesA Clinical Study of Intensity-Modulated Radiotherapy-Induced Dry Eye Disease in Head and Neck MalignanciesBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Efficacy of Azoles Antifungals in Treatment of Pityriasis VersicolorDocument4 pagesEfficacy of Azoles Antifungals in Treatment of Pityriasis VersicolorAngelika Student1109No ratings yet
- Thamir Al-Khlaiwi, Sultan A. Meo,: Objectives: ResultsDocument5 pagesThamir Al-Khlaiwi, Sultan A. Meo,: Objectives: ResultsDyah Wahyu Oktania SariNo ratings yet
- Evaluation of Cloth Masks and Modified Procedure Masks As Personal Protective Equipment For The PubliDocument18 pagesEvaluation of Cloth Masks and Modified Procedure Masks As Personal Protective Equipment For The Publiharaldd5No ratings yet
- 2020 Wang - Mask Use During COVID-19 A Risk Adjusted StrategyDocument27 pages2020 Wang - Mask Use During COVID-19 A Risk Adjusted StrategyHandy NugrohoNo ratings yet
- Impact of The Covid-19 Pandemic On The Work Activity of Spanish Physical Therapists and Their Response To VaccinationDocument12 pagesImpact of The Covid-19 Pandemic On The Work Activity of Spanish Physical Therapists and Their Response To VaccinationJesus Sanchez MasNo ratings yet
- Hariati 2018 J. Phys. Conf. Ser. 1073 062020Document7 pagesHariati 2018 J. Phys. Conf. Ser. 1073 062020Amira IzzatusyuhadaNo ratings yet
- Effectiveness of Surgical and Cotton MaskstDocument2 pagesEffectiveness of Surgical and Cotton MaskstEduardo FilhoNo ratings yet
- Cancer Oral 1Document4 pagesCancer Oral 1Jessica Paola LagunaNo ratings yet
- Containing Salicylic Acid 0.05%水杨酸功效Document5 pagesContaining Salicylic Acid 0.05%水杨酸功效jiying huangNo ratings yet
- Waste 2Document9 pagesWaste 2Sajin AlexanderNo ratings yet
- Waste 5Document5 pagesWaste 5Sajin AlexanderNo ratings yet
- Ppe 29Document10 pagesPpe 29Sajin AlexanderNo ratings yet
- Ppe 26Document5 pagesPpe 26Sajin AlexanderNo ratings yet
- Ppe 9Document6 pagesPpe 9Sajin AlexanderNo ratings yet
- Ppe 10Document12 pagesPpe 10Sajin AlexanderNo ratings yet
- Ppe 7Document6 pagesPpe 7Sajin AlexanderNo ratings yet
- Ppe 4Document6 pagesPpe 4Sajin AlexanderNo ratings yet
- Change in LegislatureDocument8 pagesChange in LegislatureSajin AlexanderNo ratings yet
- Pediatric DermatosesDocument58 pagesPediatric DermatosesSajin AlexanderNo ratings yet
- Disorders of PigmentationDocument68 pagesDisorders of PigmentationSajin AlexanderNo ratings yet
- Retail Banking ChannelsDocument6 pagesRetail Banking Channelsbeena antuNo ratings yet
- How To Install A Light FixtureDocument5 pagesHow To Install A Light FixtureMarc RiomalosNo ratings yet
- Leccture 4 - Cost of CapitalDocument38 pagesLeccture 4 - Cost of CapitalSeth BrakoNo ratings yet
- Capital Expenditure Control: DR Palash BairagiDocument38 pagesCapital Expenditure Control: DR Palash Bairagisundaram MishraNo ratings yet
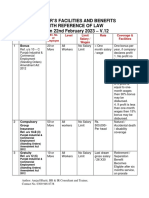
- V 12 - Schedule of Important Labor Laws - 22.02.2023Document6 pagesV 12 - Schedule of Important Labor Laws - 22.02.2023haris hafeezNo ratings yet
- Universal Pump Cart: No. PC200Document1 pageUniversal Pump Cart: No. PC200herbert madariagaNo ratings yet
- Owners ManualDocument24 pagesOwners ManualYouness AlamiNo ratings yet
- Gripping, Prying and TwistingDocument8 pagesGripping, Prying and TwistingLeslie Joy Anastacio VizcarraNo ratings yet
- RCC Teen - Task 5 - BandwidthDocument2 pagesRCC Teen - Task 5 - BandwidthRares AndreiNo ratings yet
- Magpie Lab Student Guide Updated 2014 FinalDocument13 pagesMagpie Lab Student Guide Updated 2014 FinalAmanueNo ratings yet
- Food and Cash Crops Social ScienceDocument19 pagesFood and Cash Crops Social ScienceSUKIRTHI K 19RBAR064No ratings yet
- 2018 Annual Public Debt ReportDocument79 pages2018 Annual Public Debt ReportDr. Ọbádélé KambonNo ratings yet
- HotelDocument2 pagesHotelKHAOULA ELAMRANINo ratings yet
- ZTE UMTS UR15 NodeB Uplink Interference Cancellation Feature GuideDocument34 pagesZTE UMTS UR15 NodeB Uplink Interference Cancellation Feature GuideNiraj Ram ShresthaNo ratings yet
- Driving Stepper Motors Using NXP I C-Bus GPIO Expanders: Rev. 2 - 11 October 2011 Application NoteDocument31 pagesDriving Stepper Motors Using NXP I C-Bus GPIO Expanders: Rev. 2 - 11 October 2011 Application NoteMike ThomsonNo ratings yet
- Chapter 3 Decision TreesDocument12 pagesChapter 3 Decision TreesMark MagumbaNo ratings yet
- ContinueDocument5 pagesContinueuWu uWuNo ratings yet
- Terrell B. Jones: Current PositionsDocument3 pagesTerrell B. Jones: Current PositionsTimiNo ratings yet
- 2014-01-15 US (Szymoniak) V American Doc 241-1 Memo MTD JPMCDocument23 pages2014-01-15 US (Szymoniak) V American Doc 241-1 Memo MTD JPMClarry-612445No ratings yet
- Geocentric MoonDocument7 pagesGeocentric MoonBob McDonaldNo ratings yet
- Sling Aircraft Lsa POHDocument160 pagesSling Aircraft Lsa POHGourav DasNo ratings yet
- Nix ManualDocument108 pagesNix ManualJérôme AntoineNo ratings yet
- Research, Design and Develop A Prototype of Multi-Spindle Drilling HeadDocument6 pagesResearch, Design and Develop A Prototype of Multi-Spindle Drilling HeadtimrompiescommunityNo ratings yet
- Summative Test gr.6 Health MedicineDocument2 pagesSummative Test gr.6 Health MedicineJINKY RAMIREZNo ratings yet
- Antivirus ListDocument3 pagesAntivirus ListAlekhyaNo ratings yet