Download as docx, pdf, or txt
You might also like
- Epperson - The Unseen Hand - An Introduction To The Conspiratorial View of History (1994)Document476 pagesEpperson - The Unseen Hand - An Introduction To The Conspiratorial View of History (1994)oihf99% (71)
- Graphy Template 06Document17 pagesGraphy Template 06adnan shoukatNo ratings yet
- Espoir Academy Admission Application Editable 3.0Document3 pagesEspoir Academy Admission Application Editable 3.0regan.chetty07No ratings yet
- PERSONAL DATA FORM - Personal DetailsDocument3 pagesPERSONAL DATA FORM - Personal DetailsMORSHEDNo ratings yet
- Youth Fellowship Registration Form: NameDocument1 pageYouth Fellowship Registration Form: NameSteven MitchellNo ratings yet
- JTL-FM-HR-005 Personal Details JTL ScaffoldingDocument2 pagesJTL-FM-HR-005 Personal Details JTL ScaffoldingpeterNo ratings yet
- Company Employee Form PDFDocument2 pagesCompany Employee Form PDFblindskateNo ratings yet
- 7 A 0 ADocument2 pages7 A 0 Antswakimathibela13No ratings yet
- Appointment Letter: Name: Sex: Father's Name: Marital Status: AddressDocument5 pagesAppointment Letter: Name: Sex: Father's Name: Marital Status: AddressNadeemNo ratings yet
- Application For Admission To SchoolDocument5 pagesApplication For Admission To SchooltohoorulainNo ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- Benjs Medicenter Patient InformationDocument1 pageBenjs Medicenter Patient InformationcharNo ratings yet
- Face SheetDocument1 pageFace Sheetdbowe9724No ratings yet
- Updated Application For Rental AccommodationDocument4 pagesUpdated Application For Rental AccommodationAnaNo ratings yet
- Job Application FormDocument2 pagesJob Application FormMitchel BibarNo ratings yet
- London Children's Academy Enrolment Forms 2023Document11 pagesLondon Children's Academy Enrolment Forms 2023Gideon AnumbaNo ratings yet
- Biodata BlankDocument1 pageBiodata BlankjonardschoolcollegeNo ratings yet
- JLS Will Questionnaire Version 4.0Document10 pagesJLS Will Questionnaire Version 4.0Benn KingyNo ratings yet
- Employment Application Form-DASSDocument2 pagesEmployment Application Form-DASSnavin212No ratings yet
- Updated Application Form - HangryDocument20 pagesUpdated Application Form - HangryTaupan JainudinNo ratings yet
- TSCC Registration Forms 2023Document4 pagesTSCC Registration Forms 2023api-251804492No ratings yet
- DE HAP ApplicationDocument1 pageDE HAP Applicationeddy.ortiz8321No ratings yet
- Candidate Job Application FormDocument2 pagesCandidate Job Application FormPrince AyaanNo ratings yet
- Bio Datacopyrighted 140725050745 Phpapp01Document2 pagesBio Datacopyrighted 140725050745 Phpapp01LC LeeNo ratings yet
- Application Form Plataran IndonesiaDocument6 pagesApplication Form Plataran Indonesiasatriaalex52No ratings yet
- Homeownership ApplicationDocument11 pagesHomeownership ApplicationMattie LynnNo ratings yet
- MCI - Job Application FormDocument2 pagesMCI - Job Application FormAbd DullNo ratings yet
- ApplicationDocument1 pageApplicationMichael AngeloNo ratings yet
- Auto-Riser Car Loan & Insurance Services: Clients InformationDocument1 pageAuto-Riser Car Loan & Insurance Services: Clients InformationMichael AngeloNo ratings yet
- Patient Registration Form 1 2018 Adult UpdatedDocument4 pagesPatient Registration Form 1 2018 Adult UpdatedEskinderNo ratings yet
- Access Florida Application Details 681754164 PDFDocument7 pagesAccess Florida Application Details 681754164 PDFDonellChristopherTorres0% (1)
- Visa Application FormDocument3 pagesVisa Application Formgirish kumarNo ratings yet
- Boyfriend Application Form: Applicant InformationDocument3 pagesBoyfriend Application Form: Applicant InformationgnoadicarNo ratings yet
- Rental ApplicationDocument2 pagesRental ApplicationRobert BatesNo ratings yet
- Questionnaire - PersonalDocument2 pagesQuestionnaire - PersonalLarah BuhaweNo ratings yet
- MCI - Job Application Form 2020Document3 pagesMCI - Job Application Form 2020dave davidNo ratings yet
- GORE Infoform PPVupdatedDocument2 pagesGORE Infoform PPVupdatedKimmy DeeNo ratings yet
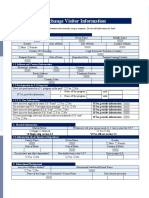
- Exchange Visitor InformationDocument3 pagesExchange Visitor InformationPrathamesh ParabNo ratings yet
- Correspondent RequirementsDocument10 pagesCorrespondent RequirementsNica HannahNo ratings yet
- UGC Bulletin 185Document18 pagesUGC Bulletin 185Rafin সাজ্জাদNo ratings yet
- To Fill-Up Id-Atm FormDocument7 pagesTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNo ratings yet
- Character References: PhotoDocument1 pageCharacter References: PhotolabelelNo ratings yet
- Internship Program Application Form: Instructions To ApplicantsDocument2 pagesInternship Program Application Form: Instructions To ApplicantsSania MirzaNo ratings yet
- TGI Employment Application FormDocument2 pagesTGI Employment Application FormReago FedelinNo ratings yet
- TGI Employment Application FormDocument2 pagesTGI Employment Application FormReago FedelinNo ratings yet
- Non-Adsb Student Registration FormDocument2 pagesNon-Adsb Student Registration FormAmeerah PoliquinNo ratings yet
- Application For Employment HPLDocument1 pageApplication For Employment HPLsamisaeed300No ratings yet
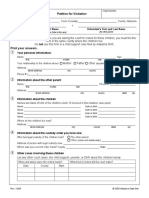
- Petition For Visitation Form PS 06Document2 pagesPetition For Visitation Form PS 06Abhishek YadavNo ratings yet
- Geirutquestionnaire 2021Document7 pagesGeirutquestionnaire 2021Menakali2003No ratings yet
- Partner 1 Partner 2: Apture of ATA ORMDocument1 pagePartner 1 Partner 2: Apture of ATA ORMjasmine.donohoeNo ratings yet
- Application Form 12-UpgradingDocument3 pagesApplication Form 12-UpgradingMakara IpiNo ratings yet
- k-8 Enrollment Application 2024-25Document3 pagesk-8 Enrollment Application 2024-25api-741164195No ratings yet
- Badge TrackerDocument20 pagesBadge TrackerAlisa BleskeNo ratings yet
- Marin Country Day School: Application For AdmissionDocument4 pagesMarin Country Day School: Application For AdmissionTammy NamNo ratings yet
- Personal Information: Last Name First Name Middle NameDocument2 pagesPersonal Information: Last Name First Name Middle NameEdith Mendoza Sabanto100% (1)
- Psa Request FormDocument3 pagesPsa Request FormLiza CruzNo ratings yet
- Blank History FormDocument9 pagesBlank History FormlatashaNo ratings yet
- BiodataDocument1 pageBiodataBARANGAY 2 POBLACIONNo ratings yet
- Ug Cuet BSW Internal UrDocument2 pagesUg Cuet BSW Internal UrSunnyNo ratings yet
- Modern Art in Fascist ItalyDocument6 pagesModern Art in Fascist ItalyKevin OumaNo ratings yet
- Marques 1994Document34 pagesMarques 1994ceren.tataylakNo ratings yet
- DACA Cover Letter TemplateDocument2 pagesDACA Cover Letter TemplateElrandomhero100% (1)
- Final Final Magazine 1Document2 pagesFinal Final Magazine 1api-602574076No ratings yet
- De-Trumping U.S. Foreign Policy Can Biden Bring America Back (Stanley R. Sloan)Document108 pagesDe-Trumping U.S. Foreign Policy Can Biden Bring America Back (Stanley R. Sloan)Pablo Fernando Suárez RubioNo ratings yet
- Our Task: To Make Rizal Obsolete: Prof. Renato ConstantinoDocument5 pagesOur Task: To Make Rizal Obsolete: Prof. Renato ConstantinoJon Joseph LlanoNo ratings yet
- History of AlbayDocument2 pagesHistory of AlbayELSA ARBRENo ratings yet
- McManus, M. (2020) - A Review of Jessica Whyte's The Morals of The Market - Human Rights and The Rise of Neoliberalism PDFDocument3 pagesMcManus, M. (2020) - A Review of Jessica Whyte's The Morals of The Market - Human Rights and The Rise of Neoliberalism PDFminastirNo ratings yet
- Reseacher Sample FalgunimahajanDocument6 pagesReseacher Sample FalgunimahajanFalguni MahajanNo ratings yet
- M. G. RamachandranDocument8 pagesM. G. Ramachandranayushonline2No ratings yet
- Colombo Plan: Dr. Maheswari JaikumarDocument20 pagesColombo Plan: Dr. Maheswari Jaikumarraymond punoNo ratings yet
- Crafting Courts in New Democracies (Ingram)Document20 pagesCrafting Courts in New Democracies (Ingram)Arthur BanzattoNo ratings yet
- What Really Happened - ConfucianismDocument3 pagesWhat Really Happened - ConfucianismzwslpoNo ratings yet
- Addis Ababa University College of Social Science Center For African and Oriental Studies Ethiopia Foreign Policy Toward Horn of AfricaDocument79 pagesAddis Ababa University College of Social Science Center For African and Oriental Studies Ethiopia Foreign Policy Toward Horn of AfricaedenNo ratings yet
- Summative Assessment - VillegasDocument3 pagesSummative Assessment - VillegasMichael VillegasNo ratings yet
- Gen004 Module5Document5 pagesGen004 Module5John Lopez CruzNo ratings yet
- Art Festival Score SheetDocument2 pagesArt Festival Score SheetMarlyvic SuavilloNo ratings yet
- Lallan Top - Latest News, Opinion & Viral Stories From India in HindiDocument36 pagesLallan Top - Latest News, Opinion & Viral Stories From India in HindiannnoyynnmussNo ratings yet
- 1AM Country NationalityDocument1 page1AM Country NationalityEmir KhanNo ratings yet
- P5 Evs 2 L14 WorksheetDocument3 pagesP5 Evs 2 L14 WorksheetAadya khattarNo ratings yet
- 2nd Form Study GuideDocument3 pages2nd Form Study GuideVirgilio CusNo ratings yet
- Two Roads To ModernisationDocument2 pagesTwo Roads To ModernisationSonia SabuNo ratings yet
- Fulltext01 PDFDocument352 pagesFulltext01 PDFCtRlZ 17No ratings yet
- EssayDocument4 pagesEssayNo ExcuseNo ratings yet
- New Era University: College of AccountancyDocument2 pagesNew Era University: College of AccountancyMakiko A. MotokiNo ratings yet
- Copyreading Symbols. Write A Slug Line and Printer's DirectionDocument2 pagesCopyreading Symbols. Write A Slug Line and Printer's DirectionPauline Karen Macaisa-ConcepcionNo ratings yet
- The People of India - A Series of Photographic Illustrations, With Descriptive Letterpress, of The Races and Tribes of Hindustan 1868Document304 pagesThe People of India - A Series of Photographic Illustrations, With Descriptive Letterpress, of The Races and Tribes of Hindustan 1868madihartahirNo ratings yet
- Branch Branch Name Province Cluster Region District Branch Contact# Branch AddressDocument3 pagesBranch Branch Name Province Cluster Region District Branch Contact# Branch Addressadnansharif1336No ratings yet