Download as pdf or txt
You might also like
- Clinical Anatomy Maxillary ArteryDocument7 pagesClinical Anatomy Maxillary ArteryNivedha AvoodaiappanNo ratings yet
- Assessment of The Peripheral Vascular SystemDocument17 pagesAssessment of The Peripheral Vascular SystemgrailbadNo ratings yet
- 16 Stroke SyndromesDocument32 pages16 Stroke SyndromesRos Potter100% (2)
- Descriptive Analysis of Sphenovomerine Suture and Its Importance in NeurosurgeryDocument4 pagesDescriptive Analysis of Sphenovomerine Suture and Its Importance in Neurosurgery相壮壮No ratings yet
- Aaid Joi D 20 00307 - R3Document32 pagesAaid Joi D 20 00307 - R3christian makaryNo ratings yet
- Branching of Mandibular Canal On Cone BeamDocument5 pagesBranching of Mandibular Canal On Cone BeamKarina CarlinNo ratings yet
- Artigo Canal RetomolarDocument6 pagesArtigo Canal Retomolarhalaldesvio.0nNo ratings yet
- Radiographic Measurements of Normal Elbows: Clinical Relevance To Olecranon FracturesDocument4 pagesRadiographic Measurements of Normal Elbows: Clinical Relevance To Olecranon Fracturesjmhinos4833No ratings yet
- Foramen Huschke PatologicoDocument7 pagesForamen Huschke PatologicoLM AdrianneNo ratings yet
- Bare Olecranon PDFDocument6 pagesBare Olecranon PDFGhassen BouaouajaNo ratings yet
- Chitsazi 2017 AAADocument6 pagesChitsazi 2017 AAAJavi ChavezNo ratings yet
- Trochlear Morphology in Healthy People ImplicatioDocument7 pagesTrochlear Morphology in Healthy People ImplicatioNacho TorreroNo ratings yet
- Bilateral Double Parotid Ducts A Case Report (#316531) - 371025Document3 pagesBilateral Double Parotid Ducts A Case Report (#316531) - 371025Evaristo GomesNo ratings yet
- The Mandibular Landmarks A FacialDocument6 pagesThe Mandibular Landmarks A Facialletty3gapeNo ratings yet
- Comparison of Overjet Among 3 Arch Types in Normal OcclusionDocument8 pagesComparison of Overjet Among 3 Arch Types in Normal OcclusionAlexandra308No ratings yet
- Archives of Oral Biology: ArticleinfoDocument6 pagesArchives of Oral Biology: Articleinfoمحمد عبدالرحمنNo ratings yet
- An Assessment of The Relationship Between The Maxillary Sinus Floor and The Maxillary Posterior Teeth Root Tips Using Dental Cone-Beam Computerized TomographyDocument6 pagesAn Assessment of The Relationship Between The Maxillary Sinus Floor and The Maxillary Posterior Teeth Root Tips Using Dental Cone-Beam Computerized TomographyLuciana EspinosaNo ratings yet
- Anatomy-Based Image Processing Analysis of The Running Pattern of The Perioral Artery For Minimally Invasive Surgery - Lee, 2014Document5 pagesAnatomy-Based Image Processing Analysis of The Running Pattern of The Perioral Artery For Minimally Invasive Surgery - Lee, 2014Rafael Autran Cavalcante AraújoNo ratings yet
- Ciftci Et Al 2023Document10 pagesCiftci Et Al 2023henriquetaranNo ratings yet
- Which Orthodontic Archwire Sequence? A Randomized Clinical TrialDocument6 pagesWhich Orthodontic Archwire Sequence? A Randomized Clinical TrialBurcuNo ratings yet
- CamperDocument64 pagesCampersilvia pérezNo ratings yet
- S 0039 1697866Document6 pagesS 0039 1697866alejandraNo ratings yet
- Atlas c1Document5 pagesAtlas c1davorribicicNo ratings yet
- Comparison of The Pharyngeal Airways of PatientsDocument10 pagesComparison of The Pharyngeal Airways of PatientsfriscaNo ratings yet
- Anatomy of The Middle Temporal Vein: Implications For Skull-Base and Craniofacial Reconstruction Using Free FlapsDocument10 pagesAnatomy of The Middle Temporal Vein: Implications For Skull-Base and Craniofacial Reconstruction Using Free FlapsPhạm Nhật HoàngNo ratings yet
- Mitral Valve Annular Downsizing Forces: Implications For Annuloplasty Device DevelopmentDocument8 pagesMitral Valve Annular Downsizing Forces: Implications For Annuloplasty Device Developmentdiana25No ratings yet
- Incisive Canal and Its Propinquity To Maxillary Central Incisors in Various Sagittal Growth Patterns: A CBCT StudyDocument11 pagesIncisive Canal and Its Propinquity To Maxillary Central Incisors in Various Sagittal Growth Patterns: A CBCT StudyIJAR JOURNALNo ratings yet
- 19 Khanapurkar EtalDocument5 pages19 Khanapurkar EtaleditorijmrhsNo ratings yet
- Analysis of Correlation Between Height of Residual Ridge and Bone Density of Residual Ridge Crest at Edentulous Mandible Using Computed TomographyDocument8 pagesAnalysis of Correlation Between Height of Residual Ridge and Bone Density of Residual Ridge Crest at Edentulous Mandible Using Computed TomographydentureNo ratings yet
- Anatomical Variationsofthe Foramen MagnumDocument11 pagesAnatomical Variationsofthe Foramen MagnumChavdarNo ratings yet
- A Three-Dimensional Comparison of Condylar Position Changes Between Centric Relation and Centric Occlusion Using The Mandibular Position Indicator. Utt 1995Document11 pagesA Three-Dimensional Comparison of Condylar Position Changes Between Centric Relation and Centric Occlusion Using The Mandibular Position Indicator. Utt 1995Fernando Ruiz BorsiniNo ratings yet
- Indian Journal of Otolaryngology and Head & Neck SurgeryDocument14 pagesIndian Journal of Otolaryngology and Head & Neck SurgeryDrKunal KaradeNo ratings yet
- Probe Tine Diameter and Probing DepthDocument5 pagesProbe Tine Diameter and Probing DepthEdgar PantojaNo ratings yet
- Centelles Et Al 2016Document8 pagesCentelles Et Al 2016henriquetaranNo ratings yet
- ContentServer AspDocument6 pagesContentServer AspSebastian RamosNo ratings yet
- 1 s2.0 S1808869421000860 MainDocument10 pages1 s2.0 S1808869421000860 MainMuhammad IqbalNo ratings yet
- Abat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyDocument10 pagesAbat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyJavier MartinNo ratings yet
- 1 s2.0 S1010518216000652 Main PDFDocument9 pages1 s2.0 S1010518216000652 Main PDFRoberto AmayaNo ratings yet
- 3D Transthoracic Echocardiography Provides Accurate Cross-Sectional Area of The RV Outflow Tract - 1Document3 pages3D Transthoracic Echocardiography Provides Accurate Cross-Sectional Area of The RV Outflow Tract - 1Thumper KatesNo ratings yet
- 12 - RyszDocument5 pages12 - RyszElvita Srie WahyuniNo ratings yet
- Akkaya 2018Document7 pagesAkkaya 2018Carolina ValenzuelaNo ratings yet
- Radiologi Aneurisma AortaDocument11 pagesRadiologi Aneurisma AortanurminsyahNo ratings yet
- Podesser 2004Document7 pagesPodesser 2004Tien Li AnNo ratings yet
- Bernardi Et Al. - 2016 - Cone Beam Computed Tomography Investigation of TheDocument6 pagesBernardi Et Al. - 2016 - Cone Beam Computed Tomography Investigation of TheCarlos Torres VillarNo ratings yet
- Maxillary Width and Hard Palate Thickness in Men and Women With Different Vertical and Sagittal Skeletal PatternsDocument10 pagesMaxillary Width and Hard Palate Thickness in Men and Women With Different Vertical and Sagittal Skeletal PatternsLily CANo ratings yet
- Garrett 2008Document11 pagesGarrett 2008Swadhinata HNo ratings yet
- Morphometric Analysis of The Foramen Magnum: An Anatomic StudyDocument4 pagesMorphometric Analysis of The Foramen Magnum: An Anatomic Studyspin_echoNo ratings yet
- 3-Dimensional Analysis and Literature Review of The Root Canal Morphology and Physiological Foramen Geometry of 125 Mandibular Incisors by Means of Micro-Computed Tomography in A German PopulationDocument8 pages3-Dimensional Analysis and Literature Review of The Root Canal Morphology and Physiological Foramen Geometry of 125 Mandibular Incisors by Means of Micro-Computed Tomography in A German PopulationalondraNo ratings yet
- CT of The Paranasal Sinuses Normal Anatomyvariants and PathologyDocument10 pagesCT of The Paranasal Sinuses Normal Anatomyvariants and PathologyAndi FirdaNo ratings yet
- Angio IRMDocument8 pagesAngio IRMAndreea MunteanuNo ratings yet
- Mandibular Posterior Anatomic Limit For MolarDocument8 pagesMandibular Posterior Anatomic Limit For MolarRommy MelgarejoNo ratings yet
- BJR 20140542Document8 pagesBJR 20140542Sava Marius ConstantinNo ratings yet
- Evaluation of Morphology and Anatomical Measurement of Nasopalatine Canal Using Cone Beam Computed TomographyDocument8 pagesEvaluation of Morphology and Anatomical Measurement of Nasopalatine Canal Using Cone Beam Computed TomographyAndre UgaldeNo ratings yet
- CT of Antrochoanal PolypDocument5 pagesCT of Antrochoanal PolypDimas PriyantonoNo ratings yet
- Evillavicencioc,+art6 CompressedDocument6 pagesEvillavicencioc,+art6 CompressedElizabeth CaballeroNo ratings yet
- Al-Kayat and BramliDocument13 pagesAl-Kayat and BramliAshish Dadhania100% (1)
- Anatomic Study of Pterygomaxillary Junctions in KoreansDocument8 pagesAnatomic Study of Pterygomaxillary Junctions in KoreansDONGXU LIUNo ratings yet
- Value of Acoustic Rhinometry For Measuring Nasal Valve AreaDocument8 pagesValue of Acoustic Rhinometry For Measuring Nasal Valve AreaKishorePrabakaranKumarNo ratings yet
- Demarcation of Arteriopulmonary Segments A Novel ADocument11 pagesDemarcation of Arteriopulmonary Segments A Novel ASergio San Juan DertkigilNo ratings yet
- Wall TrackingDocument14 pagesWall TrackinghoplalaNo ratings yet
- Atlas of CT Angiography: Normal and Pathologic FindingsFrom EverandAtlas of CT Angiography: Normal and Pathologic FindingsNo ratings yet
- Jin Gang Walking GongDocument2 pagesJin Gang Walking GongKaraim KaraimNo ratings yet
- Awesome ReviewDocument11 pagesAwesome Reviewapi-512337782No ratings yet
- Emervel Portfolio BookletDocument8 pagesEmervel Portfolio Bookletvini_tbNo ratings yet
- One Lung VentilationDocument38 pagesOne Lung VentilationVarun Reddy V100% (1)
- "CPSP Questions": Question No. 01Document39 pages"CPSP Questions": Question No. 01Moin AshrafNo ratings yet
- Lumbar Plexus (Grays Anatomy)Document12 pagesLumbar Plexus (Grays Anatomy)Joemar ReveloNo ratings yet
- Table of Upper Limb JointsDocument3 pagesTable of Upper Limb JointsVijay Pradeep100% (3)
- Pathway For Shoulder PainDocument1 pagePathway For Shoulder Painrizk86No ratings yet
- Body Parts Vocabulary Esl Multiple Choice Test For KidsDocument2 pagesBody Parts Vocabulary Esl Multiple Choice Test For KidsАлинаNo ratings yet
- Anatomy and Physiology of The Human LungDocument13 pagesAnatomy and Physiology of The Human LungRosal ClarinoNo ratings yet
- 12 Cranial NervesDocument2 pages12 Cranial NervesJessica KruppNo ratings yet
- Conduction System of The HeartDocument9 pagesConduction System of The Hearthirap50% (2)
- Dim Mak Vital Points From Rick ClarkDocument7 pagesDim Mak Vital Points From Rick Clarknakadakaken100% (1)
- The Respiratory System: Supplement To Text, Chapter 9Document77 pagesThe Respiratory System: Supplement To Text, Chapter 9Christina GonezNo ratings yet
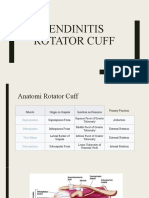
- Tendinitis Rotator CuffDocument17 pagesTendinitis Rotator CuffDewii OhyverNo ratings yet
- FMS II Lab Manual Week 1Document20 pagesFMS II Lab Manual Week 1Dapot SianiparNo ratings yet
- Embryology04 CardiovascularSystemDocument48 pagesEmbryology04 CardiovascularSystemAlexandre NascimentoNo ratings yet
- LESSON 4 Basic Steps PDFDocument28 pagesLESSON 4 Basic Steps PDFLovlegin DiongNo ratings yet
- Changes in The Body: What Is Puberty?Document4 pagesChanges in The Body: What Is Puberty?Mitch MarananNo ratings yet
- SCIENCE Role of Hormone in Female and Male Reproductive SystemDocument8 pagesSCIENCE Role of Hormone in Female and Male Reproductive SystemJasmineNo ratings yet
- The Manufacture of Boots and Shoes 1000747941Document321 pagesThe Manufacture of Boots and Shoes 1000747941adiseif100% (3)
- HA Breast & AxillaDocument27 pagesHA Breast & AxillaDarran Earl GowingNo ratings yet
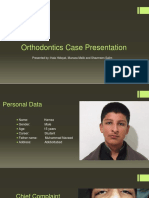
- Ortho Case ReportDocument6 pagesOrtho Case ReportAlex Adille OgaoNo ratings yet
- Language of AnatomyDocument31 pagesLanguage of AnatomyAlexa UyNo ratings yet
- Ent MBBS NotesDocument23 pagesEnt MBBS NotesDr.Riashat azimNo ratings yet
- Labour Law Notes - CompensationDocument6 pagesLabour Law Notes - CompensationayishaNo ratings yet
- Thyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadDocument87 pagesThyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadSherman BellNo ratings yet
- Ortho CaseDocument26 pagesOrtho CaseYusra ShaukatNo ratings yet