Professional Documents
Culture Documents
Safety and Efficacy of Statin Therapy
Safety and Efficacy of Statin Therapy
Uploaded by
Alexa ArceCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Safety and Efficacy of Statin Therapy
Safety and Efficacy of Statin Therapy
Uploaded by
Alexa ArceCopyright:
Available Formats
Reviews
PREVENTION OF CVD
Safety and efficacy of statin therapy
Bhavin B. Adhyaru1* and Terry A. Jacobson1,2*
Abstract | The 2013 ACC/AHA guidelines on blood cholesterol management were a major shift
in the delineation of the main patient groups that could benefit from statin therapy and emphasized
the use of higher-intensity statin therapies. In 2016, an expert consensus panel from the ACC
recommended the use of nonstatin therapies (ezetimibe and PCSK9 inhibitors) in addition to
maximally tolerated statin therapy in individuals whose LDL-cholesterol and non-HDL-cholesterol
levels remained above certain thresholds after statin treatment. Given the substantial benefits
of statin therapies in both primary and secondary prevention of cardiovascular disease, their
long-term safety has become a concern. The potential harmful effects of statin therapy on muscle
and liver have been known for some time, but new concerns have emerged regarding the risk of
new-onset diabetes mellitus, cognitive impairment and haemorrhagic stroke associated with the
use of statins and the risks of achieving very low levels of LDL cholesterol. The increased media
attention on the adverse events associated with statins has unfortunately led to statin therapy
discontinuation, nonadherence to therapy or concerns about initiating statin therapy. In this
Review , we explore the safety of statin therapy in light of the latest evidence and provide clinicians
with reassurance about the safety of statins. Overwhelming evidence suggests that the benefits
of statin therapy far outweigh any real or perceived risks.
Statin-associated muscle
Strong evidence indicates that statins reduce the risk basis of a patient’s baseline risk of ASCVD and the inten-
symptoms of atherosclerotic cardiovascular disease (ASCVD) in sity of statin therapy required for risk reduction1. Statins
(SAMS). Muscle symptoms that primary and secondary prevention1. A meta-analysis were recommended as first-line therapy for ASCVD risk
are the most prevalent adverse from the Cholesterol Treatment Trialists (CTT) sug- reduction on the basis of high-quality data, given the
effect reported with statin
gested that each 1 mmol/l reduction in LDL-cholesterol consistent reductions in ASCVD events observed with
therapy.
(LDL-C) levels in the plasma (approximately 39 mg/dl) the use of statins in primary and secondary preven-
reduces the risk of ASCVD events by 22% after 5 years2,3. tion of ASCVD. Four major statin benefit groups were
However, data from surveys, registries and insurance identified: patients with clinical ASCVD (such as acute
claims suggest that adverse effects of statins are com- coronary syndromes, history of myocardial infarction
mon, which discourages patients from continuing statin (MI), stable or unstable angina, stroke, transient ischae-
therapy at recommended doses4. mic attack (TIA) or peripheral artery disease); patients
In this Review, we briefly discuss the patient popula- without ASCVD or diabetes mellitus with primary eleva-
tions that benefit from statin therapy, as well as the updated tion of LDL-C levels >190 mg/dl (>4.9 mmol/l); patients
recommendations on nonstatin therapy and the use of with diabetes (type 1 or type 2) aged 40–75 years with
LDL-C thresholds to reduce the risk of ASCVD. We dis- LDL-C levels of 70–189 mg/dl (1.8–4.9 mmol/l) and
1
Division of General Internal cuss in detail the evidence base for several adverse effects without clinical ASCVD; and patients without diabe-
Medicine & Geriatrics, of statins, including statin-associated muscle symptoms tes or clinical ASCVD and an estimated 10-year risk of
Department of Medicine,
Emory University School of
(SAMS), and the risks of liver disease, diabetes melli- ASCVD risk ≥7.5%.
Medicine, Atlanta, GA, USA. tus, cognitive impairment and haemorrhagic stroke. According to the 2013 ACC/AHA blood cholesterol
2
Lipid Clinic and Given the high prevalence in clinical practice of mus- management guidelines, the recommended intensity of
Cardiovascular Risk cle symptoms associated with statin therapy, we further statin therapy is based on both the risk of ASCVD and
Reduction Program, explore statin intolerance and examine the risks associated the required percentage reduction in LDL-C levels to
Department of Medicine, with achieving very low LDL-C levels. reduce the risk of ASCVD1. The intensity of statin ther-
Emory University School of
Medicine, Atlanta, GA, USA.
apy is determined by the predicted percentage reduction
Statin efficacy in LDL-C levels: a reduction in LDL-C levels of >50%
*e-mail: badhyar@emory.edu;
tjaco02@emory.edu In 2013, the ACC/AHA guidelines for the management is classified as high-intensity statin therapy (for exam-
https://doi.org/10.1038/ of blood cholesterol levels proposed a paradigm shift in ple, 40–80 mg of atorvastatin and 20–40 mg of rosuva
s41569-018-0098-5 the management and treatment of lipid disorders on the statin daily), whereas reductions of 30–50% or <30% in
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 757
Reviews
In addition, analysis by type of event revealed that
Key points
coronary-related deaths or nonfatal MI were signifi-
• Moderate-intensity and high-intensity statin therapy has demonstrated benefits cantly reduced by 13%, coronary revascularizations by
in reducing the risk of atherosclerotic cardiovascular disease in both primary and 19% and ischaemic stroke by 16% in the more-intensive
secondary prevention. statin group compared with the less-intensive statin
• The most commonly reported adverse effects of statins are statin-associated muscle group. These results are very similar to the proportional
symptoms (SAMS), but whether these symptoms are caused by statin pharmacological risk reduction in major vascular events per 1 mmol/l
effects or by nocebo effects is controversial.
reduction in LDL-C levels seen in the trials on statin ver-
• The clinical tool SAMS-Clinical Index (SAMS-CI) might help clinicians to assess SAMS. sus control (22%), which was also observed in multiple
• Although hepatotoxicity has been a previous concern when using statin therapy, subgroups including secondary and primary prevention
data suggest that statins are safe and that levels of liver enzymes do not need to be cohorts and individuals with diabetes, hypertension, low
checked routinely.
HDL-cholesterol (HDL-C) levels or advanced age. Data
• Other known adverse effects of statins include a small increase in the risk of diabetes from the 26 RCTs showed that patients aged >75 years
mellitus and a possible increase in haemorrhagic stroke in patients who have had a had less benefit in reduction of major vascular events
previous stroke.
(rate ratio (RR) 0.84, 95% CI 0.73−0.97) with statin ther-
• Although concerns have been raised about reaching very low levels of LDL apy than younger patients, although the absolute num-
cholesterol, data from trials on PCSK9 inhibitors suggest that low LDL-cholesterol
ber of patients in this subgroup was small3. However,
levels are safe.
given that the absolute risks of major vascular events are
higher among old individuals, the absolute benefits of
LDL-C levels are classified as moderate-intensity and statin therapy in these patients might be similar to those
low-intensity statin therapy, respectively. The calcula- in younger individuals.
tion of the risk of ASCVD is based on a pooled cohort The findings from the CTT meta-analysis suggest that
equation derived from several patient populations in the further lowering of LDL-C levels in high-risk patients
USA. Considerable controversy surrounded the 2013 provides additional benefits and that the patient’s
ACC/AHA cholesterol guidelines with regard to the lack risk of ASCVD should be assessed to decide whether
of specific LDL-C goals, the use of nonstatin therapy and to initiate statin therapy. Given that the size of the risk
the treatment of special patient populations. To address reduction is directly proportional to the absolute LDL-C
these concerns, in 2016 and 2017, an expert consensus level reduction achieved, large LDL-C level reductions
panel from the ACC updated the recommendations on of 2–3 mmol/l would be expected to yield risk reduc-
the use of nonstatin therapies on the basis of the results tions of 40–50%. Although LDL-C reductions induced
from the IMPROVE-IT5 and FOURIER6 studies and by statin therapy are independent of baseline LDL-C
further defined the importance of achieving LDL-C levels, statins with greater LDL-C-lowering efficacy
thresholds or goals based on specific risk groups7–9. such as the high-intensity statins (atorvastatin 40–80 mg
The major statin benefit groups discussed above are or rosuvastatin 20–40 mg) are often required for LDL
derived from multiple randomized, controlled trials reductions of >50%. Of note, each additional doubling
(RCTs) and meta-analyses of these RCTs. The landmark of the dose of any statin will produce additional reduc-
2010 CTT meta-analyses examined individual-level tions in LDL-C levels of only 6%, which indicates that
patient data from 26 RCTs on statin therapy that the LDL-C-lowering efficacy of statins has limits, par-
included 170,000 individuals at various risk levels of ticularly with moderate-intensity statins (fluvastatin,
major vascular events, including major coronary events lovastatin, pitavastatin, pravastatin and simvastatin)4.
(such as nonfatal MI and coronary heart disease (CHD)- In a subsequent CTT meta-analysis published
related death), stroke and revascularization procedures3. in 2012, the benefits of statin therapy were evaluated in
One part of the meta-analysis included 129,526 patients patients at very low risk of vascular disease15. A pooled
from 21 RCTs that compared statin versus control (pla- analysis of a primary prevention patient cohort with
cebo or usual care) in patients with a mean LDL-C level an ASCVD risk score of 5–10% showed a 31% relative
of 3.7 mmol/l (143 mg/dl) over a median follow-up of risk reduction in major vascular events over 5 years
5 years. The other part of the meta-analysis compared in patients receiving statins compared with patients
data on more-intensive versus less-intensive statin receiving placebo and an 11% relative risk reduction
therapy from five RCTs that included 39,612 patients. in all-cause death. Even patients with an ASCVD risk
The more-intensive statin regimen groups were pre- score <5% had a 38% relative risk reduction in major
scribed a daily dose of 80 mg of either atorvastatin vascular events, but they showed no reductions in all-
(PROVE-IT 10, TNT 11 and IDEAL 12) or simvastatin cause mortality15. Of note, the role of statins in younger
(A to Z13 and SEARCH14). Overall, in the 26 trials, a patients (aged <40 years) and in elderly individuals
Statin intolerance reduction of 1 mmol/l (approximately 39 mg/dl) in (aged >80 years) is unclear given the lack of high-quality
A clinical syndrome
LDL-C levels over 5 years reduced major vascular events data. Some evidence from the CTT study indicates that
characterized by the inability
to tolerate multiple statins with by 22% (95% CI 20–24%, P < 0.0001), CHD death by 20% patients aged <75 years might benefit from statin therapy
either objectionable symptoms and all-cause mortality by 10% (Table 1). In the five trials even if they are in the lowest ASCVD risk group.
or abnormal laboratory of more-intensive versus less-intensive statin therapy, Statin therapy has been studied in particular patient
determinations that are an additional reduction of 0.5 mmol/l in LDL-C levels groups, and the outcomes have varied. For example, many
temporally related to statin
treatment and reversible upon
yielded a 15% further proportional reduction in the high-risk patients with heart failure (HF) were excluded
statin discontinuation but rate of major vascular events, corresponding to a 28% from previous RCTs. Two RCTs, the CORONA16 and
reproducible by rechallenge. risk reduction per 1 mmol/l reduction in LDL-C levels. GISSI-HF 17 studies, were designed to examine the
758 | DECEMBER 2018 | volume 15 www.nature.com/nrcardio
Reviews
Table 1 | Meta-analysis of 26 trials on statin therapy in 170,000 patients3 effect of statins was not significant in patients receiving
haemodialysis (HR 0.95, 95% CI 0.78–1.15). The AURORA
Outcome Number of events (% per year) RR (95% CI)a trial 19, which compared patients with end-stage
High-intensity Moderate-intensity renal disease receiving haemodialysis randomly assigned
statin statin to receive 10 mg rosuvastatin or placebo, showed no sig-
Coronary events nificant benefit of statin therapy on the combined primary
Nonfatal MI 3,485 (1.0) 4,593 (1.3) 0.73 (0.69–0.78) end point of death from cardiovascular causes, non
fatal MI or nonfatal stroke (HR 0.96, 95% CI 0.84–1.11,
CHD death 1,887 (0.5) 2,281 (0.6) 0.80 (0.74-0.87)
P = 0.59). The 4D trial20 to evaluate the effect of ator-
Any major coronary event 5,105 (1.4) 6,512 (1.9) 0.76 (0.73–0.78) vastatin (20 mg daily) versus placebo in 1,255 patients
Revascularization procedures with type 2 diabetes who were receiving haemodialysis
CABG surgery 1,453 (0.4) 1,857 (0.5) 0.75 (0.69–0.82) also showed little evidence of benefit (RR 0.92, 95%
CI 0.77–1.10, P = 0.37). In conclusion, the role of statins
PTCA 1,767 (0.5) 2,283 (0.7) 0.72 (0.65–0.80)
in patients receiving haemodialysis is unclear.
Unspecified 2,133 (0.6) 2,667 (0.8) 0.76 (0.70–0.82)
Any coronary 5,353 (1.5) 6,807 (2.0) 0.75 (0.72-0.78) Statin safety
revascularization Statin-associated muscle symptoms
Stroke Definition. SAMS are the most commonly reported
adverse effects of statins (present in 10–29% of patients
Ischaemic stroke 1,427 (0.4) 1,751 (0.5) 0.79 (0.72–0.87)
taking statin therapy according to observational
Haemorrhagic stroke 257 (0.1) 220 (0.1) 1.12 (0.88–1.43) studies)21,22. This observation is in sharp contrast with
Unknown stroke 618 (0.2) 709 (0.2) 0.88 (0.76–1.01) the results of RCTs, which often report minimal dif-
Any stroke 2,302 (0.6) 2,680 (0.8) 0.84 (0.79–0.89) ferences in the rates of muscle symptoms between
statin-treated and placebo-treated groups 4. These
Vascular events
adverse events are a very common reason for stopping
Any major vascular event 10,973 (3.2) 13,350 (4.0) 0.78 (0.76–0.80) statin therapy despite the well-known cardiovascular
CHD, coronary heart disease; MI, myocardial infarction; PTCA , percutaneous transluminal coronary benefits of the therapy22,23. Varying definitions and terms
angioplasty ; RR , rate ratio. aRR per 1 mmol/l (39 mg/dl) reduction in LDL-cholesterol levels.
are used to define the muscle-related symptoms of stat-
ins and often vary by guidelines24. Of note, SAMS often
effects of statins in patients with HF. The CORONA occur in the absence of an elevation in creatine kinase
study 16 included 5,011 patients (aged ≥60 years) plasma levels, and the symptoms can vary from myalgia
with systolic HF (New York Heart Association (NYHA) to rhabdomyolysis. The term SAMS has become the pre-
class II–IV) of ischaemic origin, with a mean baseline ferred term for muscle symptoms because it does not
LDL-C level of 137 mg/dl and mean ejection fraction necessarily imply causality.
(EF) of 27%, who were randomly assigned to receive Myalgias, cramps and weakness can be categorized
a daily dose of 10 mg rosuvastatin or placebo. No signi as SAMS. Symptoms are usually bilateral and affect large
ficant effects were observed with statin therapy for the muscle groups (thighs, calves, hip flexors or proximal
composite outcome of cardiovascular-related death, non- upper extremities). Symptoms often appear shortly
fatal MI or stroke (HR 0.92, 95% CI 0.83–1.02, P = 0.12). after starting statin therapy or after increasing the dose
The GISSI-HF study17 included a broader range of and generally resolve quickly after cessation of statin
patients in NYHA class II–IV, irrespective of EF or aetio therapy. If the symptoms persist for ≥2 months after
logy (n = 4,600), who were randomly assigned to receive drug cessation, other causes should be explored24.
rosuvastatin (10 mg daily) or placebo. The average age of Health-care providers should realize that although
the patients was 68 years and the study included younger the incidence of SAMS in patients taking statins ranges
Creatine kinase patients than those in the CORONA study16 (mean age from 10% to 29%, the occurrence of myopathy with
An enzyme that is found in
73 years), and 10% of the patients had an EF >40%. The plasma creatine kinase elevation >10 times the upper
skeletal muscle, the heart, and
the brain, and increases in the study revealed no significant difference in the mortality limit of normal (ULN) and rhabdomyolysis is very rare24.
blood due to muscle injury, or rate of hospitalization associated with cardiovascu- In patients taking statins, the incidence of myopathy
inflammation or necrosis of lar events between the rosuvastatin and placebo groups with plasma creatine kinase changes >10 times ULN
skeletal or heart muscle. (HR 1.00, 95% CI 0.898–1.122, P = 0.943). In summary, is estimated to be approximately 1 in 1,000, whereas
Myalgia
these two studies did not show a clear benefit of statin the incidence of rhabdomyolysis is approximately
A condition involving muscle therapy in patients with HF with reduced EF. 1 in 10,000 (ref.24). Myopathy and rhabdomyolysis have
aches, stiffness, soreness, The role of statin therapy in patients receiving haemo been previously reviewed in the SAMS recommenda-
tenderness or cramps. dialysis is also unclear. Three major RCTs, SHARP18, tions of the National Lipid Association (NLA) Safety
AURORA19 and 4D20, have evaluated statins in patients Task Force24, as well as in the recommendations of the
Rhabdomyolysis
A rare, life-threatening with chronic kidney disease. The SHARP trial18, which Canadian25 and European26 Working Groups.
condition, characterized by the included patients with chronic kidney disease (33%
rapid destruction of skeletal of patients were receiving haemodialysis) randomly Evaluation. An initial step in the evaluation of SAMS is
muscle typically with creatine assigned to receive 20 mg simvastatin plus 10 mg ezeti to assess plasma creatine kinase levels to rule out more
kinase levels >10 times the
upper limit of normal and
mibe daily or placebo, showed a 17% risk reduction in substantial muscle involvement, as seen in myopathy or
which often leads to acute the end point of ASCVD events with statin therapy com- rhabdomyolysis. However, most SAMS are not accom-
renal failure. pared with placebo (HR 0.83, 95% CI 0.74–0.94), but the panied by creatine kinase elevations, which makes the
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 759
Reviews
diagnosis more dependent on clinical characteristics, In addition, the SAMS-CI was assessed retrospec-
including symptom location and distribution, temporary tively in a validation study published in 2017 that used
onset upon initiation or rechallenge, and resolution of data from a randomized, double-blind, crossover trial
symptoms upon dechallenge. in patients with SAMS who received simvastatin and
The next step in evaluating SAMS is statin discon- coenzyme Q10 or placebo30,31. Using a slightly revised
tinuation and rechallenge with either a lower dose of SAMS-CI scoring system, a low SAMS-CI score
the same statin or the use of another statin. A washout (<4 instead of <6) had a negative predictive value of
period of several weeks might be helpful before rechal- 91% in identifying patients who were unlikely to have
lenge. Another strategy to consider after failing a third true myalgia 31. Although patients with confirmed
statin at its lowest dose is to consider alternate-day dos- SAMS who were treated with simvastatin had higher
ing of longer-acting statins, such as rosuvastatin or ator- mean scores (6.7) than patients with muscle symptoms
vastatin. A meta-analysis of 13 RCT studies showed that who received placebo (2.2), the index did not differ-
alternate-day dosing can be as efficacious as daily dos- entiate those individuals who had muscle symptoms
ing in lowering LDL-C levels, but its effect on ASCVD when receiving either simvastatin or placebo. These
outcomes remains unclear27. results suggest that the SAMS-CI is a more efficient
In 2014, the NLA proposed a clinical myalgia scor- tool for identifying patients who are unlikely to have
ing system, the Statin Myalgia Clinical Index (SMCI), true SAMS than for identifying patients with true
which might be useful for clinicians in determining the SAMS. This tool might also be helpful for clinicians to
probability that muscle symptoms are statin-related24. motivate patients to adhere to statin therapy even in the
The SMCI was based on several observational stud- presence of muscle symptoms. The SAMS-CI and scor-
ies, including the PRIMO 21 and STOMP 28 studies. ing system need to be further validated prospectively
The PRIMO trial21 included data from questionnaires in other studies30.
completed by 7,924 French patients treated with flu-
vastatin (80 mg daily), atorvastatin (40–80 mg daily), Causes. Several factors can increase the risk of SAMS,
pravastatin (40 mg daily) or simvastatin (40–80 mg including high doses and increased serum concentra-
daily) for ≥3 months. Muscle symptoms were reported tion of statins, the use of statin-interacting drugs that
by 10.5% of the patients. The STOMP study28 included inhibit statin catabolism, hypothyroidism, reduced
420 patients who were randomly assigned to receive muscle mass and increased physical activity 21,31–33.
80 mg atorvastatin or placebo daily for 6 months. In addition, advanced age, female sex, physical frailty
The term myalgia was applied to patients who met all the and alcohol use can increase the risk of SAMS33. Statins
following criteria: new muscle symptoms that were not are metabolized by the cytochrome P450 pathway, which
associated with exercise, symptom duration >2 weeks, transforms lipophilic compounds into hydrophobic
symptom resolution within 2 weeks of statin cessation compounds in the liver for excretion34; the metabolism
and symptom recurrence within 4 weeks of drug rechal- of various statins is detailed in Table 2. Atorvastatin,
lenge. The results of the STOMP trial28 were used to cre- lovastatin and simvastatin are metabolized primarily
ate a clinical profile of patients with true statin-related by cytochrome P450 3A4 (CYP3A4). Medications that
myalgia. For example, patients with true statin-related are also metabolized by CYP3A4, including azole anti-
myalgia were more likely to have bilateral muscle symp- fungals, macrolide or mycin antibiotics, protease inhib-
toms in the calf and thigh muscles than patients in the itors, Ca2+ channel blockers and warfarin, can increase
placebo group, who had more generalized or nonspecific serum concentrations of statins34. Other statins, such
muscle symptoms. Muscle symptoms seemed to occur as fluvastatin, pitavastatin and rosuvastatin, are min
faster among patients with true myalgia after statin imally metabolized by CYP2C9 and have fewer statin–
initiation than in the placebo group (typically 35 days drug interactions. Pravastatin is not metabolized by the
versus 61 days)28. cytochrome P450 system. Gemfibrozil can also interact
In 2017, the NLA SMCI was revised and renamed with statin metabolism and significantly increase the
the Statin-Associated Muscle Symptom Clinical Index risk of SAMS34,35. The statins with the longest half-lives
(SAMS-CI)29 (Box 1). This change was made to better (atorvastatin and rosuvastatin) can reduce LDL-C
reflect the full breadth of SAMS in addition to myal- levels even when taken on a nondaily basis, making
gia and to prepare the instrument for clinical use. these statins particularly attractive for individuals with
In addition, the inter-rater reliability of the SAMS-CI statin intolerance.
was assessed to increase its clinical utility29. The inves- Given that the prevalence of SAMS in observational
tigators conducted constructed in-depth interviews studies is much higher (10–29%) than the prevalence
with the original authors of the index, asked inde- reported in RCTs (1–2%), some investigators have pos-
pendent physicians to develop inter-rater reliability tulated that SAMS could be a result of a nocebo effect.
and sought feedback from external physicians on the The nocebo effect is observed when subjective adverse
clinical use of the SAMS-CI in practice. This quali- events are more likely to be attributed to a treatment
tative study revealed an inter-rater reliability of 0.77 that is believed to cause harm. The investigators of
(95% CI 0.66–0.85), which indicates a fairly high con- the ASCOT-LLA study36,37 examined various adverse
cordance between raters. According to these findings, events of statins in the blinded and unblinded phases
the SAMS-CI might be an improved way to detect of the trial. The first phase of the study was a blinded
SAMS and to optimize treatment for patients with phase that included 10,180 patients randomly assigned
these symptoms29. to receive atorvastatin (10 mg daily) or placebo. After
760 | DECEMBER 2018 | volume 15 www.nature.com/nrcardio
Reviews
the primary end point of combined fatal CHD or non- safety analysis, the design was observational and not an
fatal MI was reached, the study was then extended to an RCT, and individuals with muscle symptoms taking stat-
unblinded phase in which all patients were offered sta- ins during the blinded phase were less likely to agree to
tin therapy. The investigators found that in the blinded take statins in the nonblinded phase38. Finally, the obser-
phase, the annual rate of muscle-related events was sim- vation that the annual rate of muscle symptoms was sig-
ilar in the placebo (2.00%) and statin (2.03%) groups. In nificantly lower in the unblinded phase (1.00–1.26%)
the unblinded phase, the annual rate of muscle-related than in the blinded phase (2.00–2.03%) also casts doubt
symptoms was 1.00% in the group not taking stat- on the possibility of a nocebo effect38.
ins compared with 1.26% in the group receiving statins The GAUSS-3 study39, which used a blinded rechal-
(HR 1.41, 95% CI 1.10–1.79, P = 0.006). These results lenge approach, is the largest study to date to assess the
suggest the possibility of a nocebo effect with respect ability of patients with a history of SAMS to tolerate sta-
to increased muscle-related symptoms in patients who tin therapy. In the initial phase of the study, 491 patients
agreed to take statins. However, the interpretation of the with SAMS received both 20 mg atorvastatin and pla-
results is controversial because the study was a post hoc cebo using a crossover design of 10-week duration per
Box 1 | The statin-associated muscle symptom clinical index29
Overview Instructions
The SAMS-Clinical Index (SAMS-CI) was designed to help • Use for patients who have had muscle symptoms that
clinicians determine the likelihood that a patient’s muscle were new or increased after starting a statin regimen.
symptoms (myalgia or myopathy) were caused by or • A statin regimen includes any statin at any dose or
associated with statin use24. frequency.
• Muscle symptoms might include aches, cramps,
Questionnaire domains heaviness, discomfort, weakness, or stiffness.
The SAMS-CI evaluates muscle symptoms using several • Interpret the score in light of other possible causes of the
domains that encompass the statin regimen, including muscle symptoms including recent physical exertion,
location and pattern of muscle symptoms, timing of changes in exercise patterns, hypothyroidism, drug
muscle symptom onset in relation to starting interaction with statins, concurrent illness, and underlying
the statin regimen, timing of muscle symptom muscle disease.
improvement after withdrawal of the statin, and timing
of muscle symptom recurrence after rechallenge with Interpretation (score: likelihood of SAMS)
a different statin regimen. The score is calculated on • 2–6: unlikely
the basis of the patterns in the different domains • 7–8: possible
(see the figure). • 9–11: probable
If one regimen of statin involved If ≥2 regimens of statin involved
Questions regarding the regimen before
Questions regarding this regimen the most recent regimen
Location and pattern of muscle symptoms Score Location and pattern of muscle symptoms Score
Symmetric, hip flexors or thighs 3 Symmetric, hip flexors or thighs 3
Symmetric, calves 2 Symmetric, calves 2
Symmetric, proximal upper extremity 2 Symmetric, proximal upper extremity 2
Asymmetric, intermittent or not 1 Asymmetric, intermittent or not 1
specific to an area specific to an area
Timing of muscle symptom onset Timing of muscle symptom onset
<4 weeks 3 <4 weeks 3
4–12 weeks 2 4–12 weeks 2
>12 weeks 1 >12 weeks 1
Timing of symptom improvement after Timing of symptom improvement after
statin withdrawal statin withdrawal
<2 weeks 2 <2 weeks 2
2–4 weeks 1 2–4 weeks 1
No improvements after 4 weeks 0 No improvements after 4 weeks 0
Rechallenge with a statin regimen Questions regarding the most recent regimen
Timing of recurrence of similar muscle Timing of recurrence of similar muscle
symptoms after starting second regimen symptoms after starting second regimen
<4 weeks 3 <4 weeks 3
4–12 weeks 1 4–12 weeks 1
>12 weeks or symptoms did not reoccur 0 >12 weeks or symptoms did not reoccur 0
Total: Total:
All four scores above must be All four scores above must be
entered before totalling entered before totalling
Figure adapted from ref.29, Springer Nature Limited.
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 761
Reviews
Table 2 | Pharmacokinetic properties of statins
Statin Bioavailability, % Lipophilicity Protein Metabolism Metabolites t1/2, h Urinary Faecal
binding, % excretion, % excretion, %
Atorvastatin 12 Yes 80–90 CYP3A4; hydroxylation, Active 15–30 2 70
oxidation
Fluvastatin 19–29 Yes >99 CYP2C9 (CYP3A4/2C8) Inactive 0.5–2.3 NR 90
(minor)
Lovastatin 5 Yes >95 CYP3A4 Active 2.9 10 83
Pitavastatin >60 Yes 99 CYP2C9/2C8 (minor); Inactive 12 15 79
glucuronidation
Pravastatin 18 No 55 Non-CYP; sulfation, Inactive 1.3–2.8 20 71
hydroxylation, oxidation
Rosuvastatin 20 No 88 CYP2C9/2C19 (minor); Active 19 10 90
biliary excretion (minor)
Simvastatin 5 Yes 94–98 CYP3A4 Active 2–3 13 58
CYP, cytochrome P450; NR , not reported; t1/2, drug half-life. Adapted with permission from ref.82, Elsevier.
treatment. During rechallenge, 42.6% of the patients The definition of statin intolerance varies between
reported intolerable muscle symptoms with atorvasta- guidelines but generally includes the inability to tolerate
tin but not with placebo, whereas 26.5% of the patients at least two different statins, with one statin assessed at
reported muscle symptoms with placebo but not with its lowest effective dose24–26,42,43.
atorvastatin. Therefore, the majority of patients accurately In 2014, the NLA defined statin intolerance as a clini-
reported statin-related symptoms. However, the modest cal syndrome characterized by the inability to tolerate at
difference in the incidence of muscle symptoms between least two statins, with one statin tested at the lowest start-
the two groups suggests that muscle symptoms are ing daily dose and another statin assessed at any daily
common in many patients and are not always related to dose, that manifests itself by either objectionable symp-
statin use. toms (real or perceived) or abnormal laboratory results
The mechanisms of SAMS are unclear, but several temporally related to statin treatment, reversible upon
hypotheses have been proposed26, including a possi- statin discontinuation and reproducible by statin rechal-
ble alteration in mitochondrial function and cellular lenge43. The assessment was to be made after excluding
energy utilization related to the depletion of coenzyme other known determinants of statin-associated symp-
Q10, which would lead to ATP depletion with aug- toms or laboratory abnormalities, such as hypothyroid-
mentation of oxidative stress by the increased prod ism, known liver or renal disease, concurrent illnesses,
uction of reactive oxygen species. Other potential use of interacting drugs, substantial changes in physical
mechanisms include decreased isoprenoid biosyn- activity or exercise, or underlying muscle disease. The
thesis as a result of decreased mevalonate production hallmark of statin intolerance between the different
and induction of mitochondria-dependent apoptosis. guidelines is generally the patient’s response to both sta-
Individuals could also have a genetic susceptibility to tin dechallenge and rechallenge. Data suggest that statin
SAMS26. Most SAMS resolve after cessation of statin intolerance leads to increased health-care costs and to a
therapy, with the exception of the very rare and idio- higher risk of nonfatal cardiovascular events44. The most
syncratic statin-induced necrotizing autoimmune myopathy common cause of statin intolerance is SAMS.
(SINAM). SAMS might be explained by both a pharma- Muscle complaints during statin treatment are
cological effect of statins and a nocebo effect. Therefore, common, and convincing patients that their muscle
health-care providers should work closely with patients symptoms might be due to causes other than the statin
to continue statin therapy, even at a lower dose or inten- treatment is sometimes difficult. Some patients might
sity or on a nondaily basis. In the hands of expert clini- experience the nocebo effect, and clinicians should not
cal lipidologists, 70–80% of patients deemed to be statin prematurely abandon statin therapy before investigating
intolerant have been able to tolerate a certain dose of other possible causes, including the nocebo effect.
statins on a daily or nondaily basis40. Useful recommen- If patients continue to have statin intolerance, non-
Statin-induced necrotizing dations from health-care providers include switching to statin therapy could be considered, especially in light
autoimmune myopathy a different statin, using a lower or nondaily dose and of the 2016 ACC consensus guidelines8. Studies have
(SINAM). A rare, immune- being able to communicate more effectively about the shown that patients with statin intolerance can tolerate
mediated myopathy
benefits and risks of statin therapy41. ezetimibe45. In addition, data from the IMPROVE-IT
characterized by proximal
muscle weakness, muscle trial5 showed that the combination of ezetimibe and
necrosis with markedly elevated Statin intolerance simvastatin did not increase the incidence of myopathy,
creatine kinase levels, and the Although statins are considered to be one of the most rhabdomyolysis or myalgia with creatine kinase eleva-
presence of autoantibodies to effective strategies to reduce cardiovascular morbidity tions >5 times ULN compared with simvastatin alone5.
hydroxyl-methyl-glutaryl-
coenzyme A reductase, in which
and mortality, many patients are unable to tolerate sta- The GAUSS-3 (ref.39) and ODYSSEY ALTERNATIVE46
muscle symptoms persist tin therapy. Therefore, the management of patients with studies demonstrated that the PCSK9 inhibitors evolo-
despite statin discontinuation. statin intolerance remains a major clinical challenge. cumab and alirocumab, respectively, can be used safely
762 | DECEMBER 2018 | volume 15 www.nature.com/nrcardio
Reviews
in patients with statin intolerance without increases in benefit of statin therapy exceeded the risk of new-onset
adverse muscle-related events39,46,47. diabetes (Table 4).
Additionally, statin therapy did not seem to have a
Risk of diabetes mellitus large effect on measures of glycaemic control, and the
The design of early, large trials on statin therapy did not small weight gain that could be associated with statin
include an assessment of newly diagnosed diabetes as a therapy might not be clinically relevant. The benefits of
clinical end point because this condition was not consid- statins in patients with diabetes were similar to those in
ered clinically relevant. In 2008, the landmark JUPITER other statin-treated subgroups of patients52.
study48 provided evidence that rosuvastatin (20 mg daily) The mechanism of new-onset diabetes associated
significantly increased the relative risk of newly diag- with statin use is not clear, but statins might interfere with
nosed diabetes by 25% compared with placebo. Previous peripheral insulin signalling and pancreatic β-cell func-
studies had not prospectively examined changes in phys tion. With regard to genetic factors, a 2015 study exam-
icians’ diagnosis of diabetes or changes in glycaemic ined single nucleotide polymorphisms in the HMGCR
control, which prompted a meta-analysis of large sta- gene as proxies for 3-hydroxy-3-methylglutaryl-CoA
tin RCTs in 2010 (ref.49) (Table 3). The pooled analysis reductase (HMG-CoA reductase) inhibition by statins53.
showed a 9% increase in the incidence of new-onset The study showed that HMG-CoA inhibition was asso-
diabetes with statin therapy, with little heterogeneity ciated not only with a reduction in plasma LDL-C levels
in incidence. Overall, the increase in absolute risk was but also with a small increase in body weight, waist
very small, with a number needed to harm (NNH) of circumference and plasma insulin and glucose concen-
255 over 4 years49. A subsequent analysis of the JUPITER trations. The data suggested that the increased risk of
study48 suggested that the cardiovascular and mortality diabetes was in part due to HMG-CoA inhibition. Over
benefits exceeded the risk of diabetes even in patients at the past decade, PCSK9 inhibitors have been developed
high risk of developing diabetes50. and have shown significant effects in reducing LDL-C
The SPARCL trial51, which was not included in the levels and the risk of cardiovascular disease. Although
2010 meta-analysis that evaluated new-onset diabetes, the large-scale FOURIER trial54 of cardiovascular out-
showed a 44% relative increase in new-onset diabetes in comes in 27,564 individuals treated with evolocumab
patients with prior stroke or TIA who were treated did not identify an increase in new-onset diabetes after
with atorvastatin (80 mg daily) compared with patients a median duration of 2.2 years, several questions with
treated with placebo, which suggested dose-dependent regard to new-onset diabetes associated with the use of
effects. Five studies, the TNT11, IDEAL12, PROVE-IT this drug class have been raised. A study published in
TIMI10, A to Z13 and SEARCH14 studies, demonstrated 2017 to assess the association between PCSK9 genetic
that more-intensive statin therapy was associated variants and type 2 diabetes showed that, similarly
with a significantly higher risk of new-onset diabe- to the study on HMCGR, every 1 mmol/l reduction
tes (12% increase in pooled risk) than less-intensive in LDL-C levels was associated with a small increase in
statin therapy and with a 16% reduction in the inci- the waist:hip ratio (0.006), body weight (1.02 kg), and
dent risk of cardiovascular disease10–14,52. Again, the fasting blood glucose levels (0.009 mmol/l) and an
Table 3 | Incidence of diabetes mellitus in major trials on statin therapy49
Study (year) Statin therapy Patients Rate of new-onset diabetesa OR (95% CI) Refs
(n)
Statin Placebo or
group control group
ASCOT-LL A (2003) Atorvastatin 10 mg 7 ,773 11.9 10.5 1.14 (0.89–1.46) 37
HPS (2003) Simvastatin 40 mg 14,573 9.2 8.0 1.15 (0.98–1.35) 83
JUPITER (2008) Rosuvastatin 20 mg 17 ,802 16.0 12.8 1.26 (1.04–1.51) 48
WOSCOPS (2001) Pravastatin 40 mg 5,974 5.2 6.5 0.79 (0.58–1.10) 84
LIPID (2003) Pravastatin 40 mg 6,997 6.0 6.6 0.91 (0.71–1.71) 85
CORONA (2007) Rosuvastatin 20 mg 3,534 20.9 18.5 1.14 (0.84–1.55) 16
PROSPER (2002) Pravastatin 40 mg 5,023 20.5 15.8 1.32 (1.03–1.69) 72
MEGA (2006) Pravastatin 10–20 mg 6,086 10.8 10.1 1.07 (0.86–1.35) 86
AFCAPS/TEXCAPS Lovastatin 20–40 mg 6,211 4.5 4.6 0.98 (0.70–1.38) 87
(1998)
4 S (1994) Simvastatin 20–40 mg 4,242 17.3 16.8 1.03 (0.84–1.28) 88
ALLHAT (2002) Pravastatin 40 mg 6,087 16.4 14.4 1.15 (0.95–1.41) 89
GISSI-HF (2008) Rosuvastatin 10 mg 3,378 34.8 32.1 1.10 (0.89–1.35) 17
GISSI-PREV (2000) Pravastatin 20 mg 3,460 27.5 30.6 0.89 (0.67–1.20) 90
Meta-analysisb All statins 91,140 12.23 11.25 1.09 (1.02–1.17) 49
a
Events per 1,000 patient-years. Pooled odds ratio from a meta-analysis of the 13 trials.
b
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 763
Reviews
Table 4 | Diabetes mellitus and cardiovascular disease in trials on intensive versus moderate statin therapy52
Study (year) Intensive and moderate Incident diabetes mellitus Incident CVD Refs
doses
Intensive- Moderate- OR (95% CI) Intensive- Moderate- OR (95% CI)
therapy group therapy group therapy group therapy group
PROVE-IT Atorvastatin 80 mg; 101/1,707 99/1,688 1.01 315/1,707 355/1,688 0.85 10
TIMI (2004) pravastatin 40 mg (5.9%) (5.9%) (0.76–1.34) (18.4%) (21.0%) (0.72–1.01)
A to Z (2004) Simvastatin 40–80 mg; 65/1,768 47/1,736 1.37 212/1,768 234/1,736 0.87 13
placebo or simvastatin 20 mg (3.7%) (2.7%) (0.94–2.01) (12.0%) (13.5%) (0.72–1.07)
TNT (2005) Atorvastatin 80 mg; 418/3,798 358/3,797 1.19 647/3,798 830/3,797 0.73 11
atorvastatin 10 mg (11.0%) (9.4%) (1.02–1.38) (17.0%) (21.9%) (0.65–0.82)
IDEAL (2005) Atorvastatin 80 mg; 240/3,737 209/3,724 1.15 776/3,737 917/3,724 0.80 12
simvastatin 20–40 mg (6.4%) (5.6%) (0.95–1.40) (20.8%) (24.6%) (0.72–0.89)
SEARCH Simvastatin 80 mg; 625/5,398 587/5,399 1.07 1,184/5,398 1,214/5,399 0.97 14
(2010) simvastatin 20 mg (11.6%) (10.9%) (0.95–1.21) (21.9%) (22.5%) (0.88–1.06)
Meta-analysisa Various 1,449/16,408 1,300/16,344 1.12 3,134/16,408 3,550/16,344 0.84 52
(8.8%) (8.0%) (1.04–1.22) (19.1%) (21.7%) (0.75–0.94)
CVD, cardiovascular disease. aPooled odds ratio from a meta-analysis of the five trials.
odds ratio of 1.12 for newly diagnosed diabetes55. Despite or stopped until further evaluation is completed. Data
the study limitations, these data corroborate previous are also available regarding the use of statins in specific
studies indicating that clinicians should screen patients liver diseases, including those below57.
for diabetes when starting statin therapy and concurrently
initiate lifestyle modification strategies. Hepatitis C. Hepatitis C affects 2% of the population in
the USA and leads to chronic liver disease-related mor-
Liver considerations bidity and mortality. The hepatitis C virus (HCV) and
Abnormal liver enzyme tests. Statins were previously lipid metabolism are interrelated, given that viral repli-
thought to have potential hepatotoxicity owing to their cation involves the LDL receptor (LDLR) and enzymes
metabolism in the liver and the interactions with the involved in cholesterol biosynthesis. Statins might inter-
cytochrome P450 pathway. In the past, elevated plasma rupt this process. Several studies have shown that statin
levels in the liver enzymes aspartate transaminase use is linked to improvements in viral response to HCV
(AST) or alanine transaminase (ALT) were a com- treatments, with a minimal effect on liver function tests.
mon reason for statin discontinuation. Hepatologists Certain statins (such as rosuvastatin) should be avoided
use Hy’s law, in which three criteria must be satisfied during hepatitis C treatment with ledipasvir and/or
to suggest drug-induced liver injury: elevation in AST sofosbuvir because of drug–drug interactions58.
or ALT ≥3 times ULN, increase in total bilirubin levels
>2 times ULN, and no other demonstrable cause such NAFLD and NASH. The prevalence of NAFLD and
as cholestasis, viral hepatitis, pre-existing or acute hepato nonalcoholic steatohepatitis (NASH) has increased with
biliary disease, or use of another drug that can cause the the rise in obesity prevalence. Approximately 9–37% of
observed injury56. Rates of fulminant hepatic failure people worldwide have NAFLD, and 3–5% have NASH,
related to statin use are rare; consequently, liver enzymes with higher frequencies in patients with obesity 56.
are not routinely evaluated except for a first-time check Statin use in patients with NAFLD or NASH is asso-
before initiation of statin therapy or periodically if the ciated with a reduction in transaminase plasma levels,
patients are symptomatic. with improvements in steatosis and the liver necro
If a patient has abnormal levels of liver enzymes inflammatory grade but no change in the liver fibrosis
(ALT or AST), the NLA has developed an algorithm grade59,60. Some evidence suggests that patients with
that can be used to guide safe statin use and other clin- NAFLD have a higher 10-year risk of cardiovascular
ical decision-making56. The algorithm is based on the disease than patients without NAFLD61. In the GREACE
degree of ALT or AST elevation: if ALT or AST elevation study62, a post hoc analysis showed that statin therapy is
is above the ULN but ≤ 3 times the ULN, bilirubin levels safe and can improve the plasma levels of liver enzymes
should be evaluated; if ALT or AST levels are normal and and reduce cardiovascular events in patients with mild
creatine kinase level is normal, the patient likely has non- abnormal liver tests attributed to NAFLD.
alcoholic fatty liver disease (NAFLD), and statin therapy
can be reasonably continued; if the elevation in bilirubin Liver transplantation. Many medications used after liver
level is indirect and not new and the creatine kinase level transplantation, such as immunosuppressive therapy,
is normal, the patient could have underlying Gilbert syn- can predispose patients to dyslipidaemia and other con-
drome or NAFLD, and the statin can be continued; a new ditions that can increase the risk of cardiovascular dis-
elevation in bilirubin levels requires further evaluation, ease. One observational study of 598 patients with liver
and the statin should be stopped until further work-up or liver–kidney transplant showed that the prevalence of
is completed; if the elevation in ALT or AST level is hyperlipidaemia increased from 12% before transplanta-
>3 times ULN, a repeated evaluation of ALT or AST levels tion to 22% at 7 years after transplantation63. The high-
should be considered, and statin therapy should be held est risk factors were the use of steroids and sirolimus.
764 | DECEMBER 2018 | volume 15 www.nature.com/nrcardio
Reviews
Statins interact with immunosuppressive agents through impairment71. Two small studies have reported poten-
their CYP3A4-related metabolism; however, statins tial adverse events of statins on cognition. One study
remain the mainstay treatment for hyperlipidaemia. of 209 patients to evaluate the potential psychological
A retrospective study with lipid-lowering agents effects of lovastatin showed that the placebo group had
(statins and fibrates) showed that 90% of the patients greater improvements in cognitive measures than the
reached target lipid levels, with no significant increases statin group at 6 months, but the difference was small
in the plasma levels of liver enzymes. All patients who and of questionable clinical relevance. Another study
developed SAMS were also receiving cyclosporine, a of 308 patients showed a potential detrimental effect of
CYP3A4 inhibitor64. Generally, caution is advisable simvastatin on cognition; however, this study was limited
when using statins that are metabolized via the CYP3A4 by the type of cognitive testing used in the study71.
pathway (atorvastatin, lovastatin and simvastatin) Few large RCTs that prospectively study statins and
in patients receiving immunosuppressants that use the cognition are available. The PROSPER72 and HPS73 stud-
same pathway (for example, cyclosporine, sirolimus ies are the only two large RCTs that have prospectively
and tacrolimus)65. studied cognitive function with the use of well-validated
neuropsychological measurements. The PROSPER
Primary biliary cirrhosis and cholestatic liver disease. study72 involved 5,804 men and women aged 70–82 years
Primary biliary cirrhosis is a rare autoimmune choles- who were at risk of vascular disease. Participants were
tatic liver disease that affects women more than men and randomly assigned to receive either pravastatin (40 mg
notably alters cholesterol metabolism57. Limited data daily) or placebo for 3 years. The patients were assessed
are available on the use of statins in this patient popu over the course of the trial using four validated neuro
lation; however, evidence suggests that statins are safe psychological performance tests for executive function,
and effective for lipid lowering in patients with primary attention, processing speed and immediate and delayed
biliary cirrhosis66. memory. These well-validated cognitive performance
tests showed no effect of pravastatin on cognitive func-
Cognition tion at any point during the trial74. In the HPS study73
Cognition is a very broad term involving four domains: involving 20,536 patients randomly allocated to simvas-
executive function, memory, language and visuospatial tatin (40 mg daily) or placebo for an average of 5 years,
ability. Cognitive dysfunction can be an impairment the effects on memory were systematically assessed
in any of these domains and represents a spectrum of using the modified Telephone Interview for Cognitive
disease67. Mild cognitive impairment (MCI) is a state Status questionnaire. The test was used only once at the
between normal cognition and dementia68. Several end of the study and revealed no difference in the percent-
observational studies and case reports have shown a pos- age of patients classified as cognitively impaired between
sible association between statins and cognitive impair- the simvastatin (23.7%) and placebo (24.2%) groups.
ment67. However, the assessment of statin-induced In addition, assessment of cognition in 5,806 patients
cognitive impairment poses challenges. The mini-mental aged 75–85 years showed no difference in cognitive
status exam (MMSE) is a common test used to assess impairment between the statin and placebo groups73.
cognition but does not evaluate executive function. The In summary, the totality of the evidence, including
Montreal Cognitive Assessment (MOCA) is more com- several meta-analyses of multiple RCTs, does not indi-
prehensive than the MMSE, but the evaluation can take cate an association between statin use and cognitive
more time. Other brief tests, including the Mini-Cog and dysfunction. Given that mild cognitive dysfunction is
Functional Activities scale, have excellent sensitivity common in elderly individuals, the NLA has provided
and specificity for distinguishing MCI and dementia some guidelines to help clinicians assess the risk of cog-
from healthy cognitive ageing69,70. The pathophysio nitive dysfunction during statin use. Generally, a baseline
logy of statin-induced cognitive dysfunction remains cognitive exam does not need to be performed before
unclear. However, some studies in animal models sug- starting statin therapy. Of note, if patients complain of
gest that the reduction of cholesterol synthesis below cognitive symptoms, symptoms should not be dismissed
a critical level in oligodendrocytes, which leads to the if patients are receiving statin therapy. A thorough clinical
inhibition of myelination in the central nervous system, history and physical exam should be performed to look
results in cognitive deficits67. Animal data also suggest for contributors to cognitive impairment, and a MOCA
that brain levels of some statins depend on their lipo- test or other screening test could be used to assess cogni-
philicity (simvastatin > lovastatin > atorvastatin > pravas- tion in the four domains. If a statin is suspected to alter
tatin > rosuvastatin) and whether statins are rapidly cognition, the reasonable option is to stop the drug for
eliminated from the brain67. 1–2 months before considering a rechallenge67.
Observational studies have shown mixed results,
with studies suggesting that statins are associated with Haemorrhagic stroke
either cognitive impairment or improvement in cogni- The 2010 pooled CTT meta-analysis of 26 RCTs involv-
tion67. However, many of these studies are biased owing ing individual patient data showed that statins reduce the
to their observational design and the inclusion of vari- overall risk of stroke by 16% (RR 0.84, 95% CI 0.79–0.89)
ous risk populations, including elderly individuals and and the risk of ischaemic stroke by 21% (RR 0.79, 95%
individuals with pre-existing cognitive dysfunction. CI 0.74–0.85) per 1 mmol/l reduction in LDL-C lev-
A 2015 meta-analysis of 23 RCTs did not indicate els3. However, the increase in the risk of haemorrhagic
that statin therapy was associated with cognitive stroke associated with statin use was not significant
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 765
Reviews
(RR 1.12, 95% CI 0.93–1.35, P = 0.20) (Table 1). The achieved an LDL-C level of <50 mg/dl (1.3 mmol/l)
issue of an increased risk of haemorrhagic stroke asso- (n = 4,000) were compared with patients who achieved
ciated with lower levels of blood cholesterol has been LDL levels >50 mg/dl (1.3 mmol/l) (n = 4,154). The
a concern ever since epidemiological studies suggested a rates of myalgia, muscle weakness, diabetes, neuro
possible correlation. psychiatric conditions, cancer and most other major
The SPARCL trial51 was the first RCT to examine adverse effects were not significantly different among
high-intensity statin (atorvastatin at a daily dose of rosuvastatin-treated participants with or without LDL-C
80 mg) versus placebo in 4,731 patients with a history levels <50 mg/dl. Other RCTs also confirmed that stat-
of stroke or TIA who had LDL-C levels of 100–190 mg/dl. ins did not increase adverse events despite LDL-C level
Although the risk of nonfatal and fatal stroke was reductions well below the existing goal or threshold of
reduced by 16% (RR 0.84, 95% CI 0.71–0.99), a small 70 mg/dl (1.8 mmol/l)3.
increase in the incidence of haemorrhagic stroke (n = 55 A post hoc analysis of the IMPROVE-IT trial77, in
versus n = 33; HR 1.66, 95% CI 1.08–2.55) was observed which 18,144 patients with previous acute coronary
in the statin group compared with the placebo group. syndrome were randomly assigned to either simvastatin
Subsequent analysis revealed that the increased risk of (40 mg daily) or a combination of simvastatin (40 mg
haemorrhagic stroke was higher in individuals with a daily) and ezetimibe (10 mg daily), was performed to
previous haemorrhagic stroke at study entry (HR 5.65, compare individuals with an achieved LDL-C level of
95% CI 2.82–11.30), in men (HR 1.79, 95% CI 1.13–2.84) <30 mg/dl (0.8 mmol/l) versus those with an LDL-C level
and in increasing 10-year age increment groups (HR 1.42, of >30 mg/dl at 1 month. During the 6 years of the trial,
95% CI 1.16–1.74)75. When the results of SPARCL51 and individuals with an LDL-C level <30 mg/dl had a simi-
CORONA16 were added to the 2010 CTT meta-analysis lar safety profile to individuals who had achieved higher
discussed above, the proportional risk of haemorrhagic LDL-C levels. The analysis indicated no differences in
stroke per 1 mmol/l of LDL-C level reduction increased safety end points including serious muscle events, ele-
by 21% (HR 1.21, 95% CI 1.05–1.41, P = 0.01)3. However, vation in plasma aminotransferase levels, gall-bladder
the small additional risk of haemorrhagic stroke is clearly adverse events, neurocognitive events, haemorrhagic
outweighed by the large reductions seen in the risk of stroke or cataracts.
ischaemic stroke and major cardiovascular events. With the advent of several new drugs, including
A meta-analysis of 23 RCTs and 19 observational the PCSK9 inhibitors alirocumab and evolocumab, the
studies including 248,391 patients with a total of 14,784 opportunity now exists to reduce LDL-C to even lower
intracerebral haemorrhages revealed no association levels by adding these drugs to high-intensity statin
between statin therapy and increased risk of intracerebral therapy. These drugs inhibit PCSK9, a protein that binds
stroke76. Analysis of RCTs (RR 1.10, 95% CI 0.86–1.41), to the LDLR and assists in the internalization of the LDLR
cohort studies (RR 0.94, 95% CI 0.81–1.10) or case–control for degradation79. The FOURIER trial6 on evolocumab
studies (RR 0.60, 95% CI 0.41–0.88) also showed no incre was the first trial of a PCSK9 inhibitor in combination
ased risk of intracerebral stroke with statin use. Although with statin therapy to show improved cardiovascular out-
the study was not an analysis of individual patient comes compared with statin therapy alone. In this trial,
data, the meta-analysis also showed no correlation between LDL-C levels were reduced from 92 to 30 mg/dl (2.4 to
the risk of intracerebral stroke and the magnitude of 0.8 mmol/l) with no accompanying safety issues after a
LDL-C level reduction. Data from the IMPROVE-IT median trial duration of 2.2 years. A further safety analy
trial77 on simvastatin and ezetimibe showed a small, sis of the FOURIER trial54 demonstrated no increased
but not significant, increase in haemorrhagic stroke safety effects with LDL-C levels <20 mg/dl (<0.5 mmol/l).
events (59 versus 43; HR 1.38, 95% CI 0.93–2.04) with In addition, a 2017 meta-analysis of pooled RCTs on
statin and ezetimibe use but no association between alirocumab evaluated the safety of achieving LDL-C
haemorrhagic stroke events and low levels of LDL-C levels as low as <25 mg/dl (<0.65 mmol/l) or <15 mg/dl
(<30 mg/dl). Similarly, the FOURIER trial6 showed a (<0.4 mmol/l) and revealed that very low LDL-C levels
nonsignificant increase in haemorrhagic stroke in the were not associated with increased adverse events inclu
statin group compared with the control group (29 versus ding diabetes, neurocognitive or muscle-related events80.
25) but no association between haemorrhagic stroke and However, a small increase in cataracts in the LDL-C
LDL-C levels <0.5 mmol/l (39 mg/dl). In summary, the <25 mg/dl group compared with the propensity-matching
SPARCL trial51 was the only trial to suggest a significant group was observed. More generally, this analysis
increase in haemorrhagic stroke with atorvastatin use, and other short-term and long-term PCSK9 studies add
whereas adjunctive statin therapy with ezetimibe and to the evidence base that achieving low LDL-C levels is
evolocumab leading to very low levels of LDL-C did not. very well-tolerated and is not associated with adverse
Therefore, any small possible additional risk of haemor- events. The ODYSSEY Outcomes trial81 with alirocumab
rhagic stroke is clearly outweighed by the large reductions will add long-term safety information on the use of
seen in overall stroke and major cardiovascular events. PCSK9 inhibitors.
Low LDL-C levels and adverse events Conclusions
In a post hoc analysis of the JUPITER study78, in which The 2013 ACC/AHA guidelines, along with other inter-
patients with an LDL-C level of <130 mg/dl (3.4 mmol/l) national guidelines, establish the primacy of statins in
were randomly assigned to high-intensity statin treat- reducing the risk of ASCVD in both primary and sec-
ment with rosuvastatin (20 mg daily), patients who ondary prevention1. Even with evidence of the benefits of
766 | DECEMBER 2018 | volume 15 www.nature.com/nrcardio
Reviews
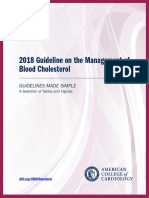
Benefits Adverse effects variety of other hepatobiliary diseases including NASH
Risk of stroke Cognitive dysfunction and hepatitis C.
• ↓ 16% for total stroke • No evidence Other adverse effects of statins such as the increase
• ↓ 21% for ischaemic stroke Risk of haemorrhagic stroke in new-onset diabetes over a 5-year time period are
• Small increase in individuals
with prior stroke very small (HR 1.1 or HR 1.2 with high-intensity statin
therapy). The risks are generally higher in individuals
Risk of major coronary events Liver symptoms/diseases at risk of developing diabetes, such as patients with
• ↓ 27% for nonfatal MI • Clinically insignificant liver
• ↓ 20% for CHD death enzyme elevations
metabolic syndrome or prediabetes. The mechanism
Risk of revascularization • Incidence of liver failure: underlying the increased risk of diabetes is currently
procedures 1/100,000 unknown, and therefore, maintaining lifestyle coun-
• ↓ 25%
Incidence of new-onset
selling during statin therapy, with an emphasis on diet,
diabetes mellitus exercise and weight loss, is prudent.
• Moderate-intensity statin Although statins have been shown to reduce the
therapy: 0.1% per year
• High-intensity statin therapy: risk of overall and ischaemic stroke in most population
0.2% per year groups studied, the SPARCL trial51 is the only study to
demonstrate a significant increase in the risk of haem-
Incidence of muscle
symptoms/diseases orrhagic stroke. The totality of the evidence suggests
• SAMS: 10–29% in observational that statins are safe in most patients with previous
studies and 1–2% in RCTs stroke, with the caveat that the data are not as robust
• Myopathy: 1/1,000
• Rhabdomyolysis: 1/10,000 in patients with a history of intracerebral haemorrhage.
Using thresholds levels of LDL-C for statin therapy
Fig. 1 | Clinical benefits and potential adverse effects of statin therapy. The has been controversial since the publication of the 2013
cardiovascular benefits, including the reduction in the risk of major coronary events and ACC/AHA guidelines on cholesterol management1.The
revascularization and the reduction in the risk of stroke, associated with statin therapy recommendation not to target LDL-C levels to a given
far outweigh the potential risks. Given this clinical benefit, providers should work goal or threshold was based on the absence of RCT
diligently with patients to ensure that patients adhere to therapy in a shared-decision
evidence to do so. However, data from the 2010 CTT
model. CHD, coronary heart disease; MI, myocardial infarction; RCT, randomized
controlled trial; SAMS, statin-associated muscle symptoms.
meta-analysis suggest that reducing LDL-C levels by
1 mmol/l (approximately 39 mg/dl) over 5 years results in
a reduction of 22% in major cardiovascular events, 20%
statin therapy, adverse effects have been cited as a major in CHD death and 10% in all-cause mortality3. The size
reason that limits patients from taking and adhering of the risk reduction in major vascular events is directly
to statin therapy. The most common reported adverse proportional to the absolute LDL-C level reduction
events of statin therapy are muscle-related and are often achieved. The findings suggest even larger risk reduc-
referred to as SAMS. The SAMS-CI is a clinical tool that tions of 40–50% with greater LDL-C level reductions of
might be useful in helping to evaluate muscle symptoms 2–3 mmol/l (77–116 mg/dl). Therefore, the goal of ther-
in patients taking statin therapy. How much of SAMS is apy is to achieve the largest LDL-C reductions without
caused by a true statin pharmacological effect versus a increasing the risk of adverse events. Evidence from
nocebo effect, or by a combination of both, is controver- the IMPROVE-IT5 and FOURIER6 trials suggests that
sial. However, the symptoms are very real for the patient, adjunctive therapy with ezetimibe and PCSK9 inhibi-
regardless of the aetiology, which gives the health-care tors in addition to high-intensity statin therapy results
provider the opportunity to explain to the patient the in a further reduction in cardiovascular risk. This risk
true benefits and harms of statin therapy using shared reduction is seen with levels of LDL-C as low as 30 mg/dl
decision-making (Fig. 1). (0.8 mmol/l) without any apparent harm. Despite con-
Although hepatic toxicity was previously consi cerns that achieving very low LDL-C levels could cause
dered a very concerning adverse effect of statin ther- harm, the results of these trials suggest that achieving
apy given the high frequency of elevated levels of liver very low LDL-C levels is generally safe and yields addi-
enzymes in the plasma, evidence has shown that statins tional cardiovascular benefits. Given how beneficial
are very safe with respect to the liver and can be used and safe statins are in reducing ASCVD events, provid-
safely in a wide variety of liver diseases. Liver enzyme ers should work diligently with patients to ensure that
levels do not need to be checked routinely in patients patients adhere to therapy in a shared-decision model.
receiving statin therapy unless the patient becomes
symptomatic. Statins have been shown to be safe in a Published online 30 October 2018
1. Stone, N. J. et al. 2013 ACC/AHA guideline on the a meta-analysis of data from 170,000 participants 7. Adhyaru, B. B. & Jacobson, T. A. Role of non-
treatment of blood cholesterol to reduce atherosclerotic in 26 randomised trials. Lancet 376, 1670–1681 statins, LDL-C thresholds, and special population
cardiovascular risk in adults: a report of the American (2010). considerations: a look at the updated 2016
College of Cardiology/American Heart Association Task 4. Collins, R. et al. Interpretation of the evidence for ACC Consensus Committee Recommendations.
Force on Practice Guidelines. J. Am. Coll. Cardiol. 63, the efficacy and safety of statin therapy. Lancet 388, Curr. Atheroscler. Rep. 19, 29 (2017).
2889–2934 (2014). 2532–2561 (2016). 8. Writing Committee. et al. 2016 ACC expert consensus
2. Baigent, C. et al. Efficacy and safety of cholesterol- 5. Cannon, C. P. et al. Ezetimibe added to statin therapy decision pathway on the role of non-statin therapies
lowering treatment: prospective meta-analysis of data after acute coronary syndromes. N. Engl. J. Med. 372, for LDL-cholesterol lowering in the management of
from 90,056 participants in 14 randomised trials of 2387–2397 (2015). atherosclerotic cardiovascular disease risk: a report
statins. Lancet 366, 1267–1278 (2005). 6. Sabatine, M. S. et al. Evolocumab and clinical of the American College of Cardiology Task Force
3. Cholesterol Treatment Trialists Collaboration. Efficacy outcomes in patients with cardiovascular disease. on Clinical Expert Consensus documents. J. Am.
and safety of more intensive lowering of LDL cholesterol: N. Engl. J. Med. 376, 1713–1722 (2017). Coll. Cardiol. 68, 92–125 (2016).
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 767
Reviews
9. Lloyd-Jones, D. M. et al. 2017 focused update of the 31. Schech, S. et al. Risk factors for statin-associated from genetic analysis and randomised trials. Lancet
2016 ACC expert consensus decision pathway on the rhabdomyolysis. Pharmacoepidemiol. Drug Saf. 16, 385, 351–361 (2015).
role of non-statin therapies for LDL-cholesterol lowering 352–358 (2007). 54. Giugliano, R. P. et al. Clinical efficacy and safety of
in the management of atherosclerotic cardiovascular 32. Banach, M. et al. Statin intolerance — an attempt at a achieving very low LDL-cholesterol concentrations with
disease risk: a report of the American College of unified definition. Position paper from an International the PCSK9 inhibitor evolocumab: a prespecified
Cardiology Task Force on Expert Consensus Decision Lipid Expert Panel. Expert Opin. Drug Saf. 14, secondary analysis of the FOURIER trial. Lancet 390,
Pathways. J. Am. Coll. Cardiol. 70, 1785–1822 935–955 (2015). 1962–1971 (2017).
(2017). 33. Abd, T. T. & Jacobson, T. A. Statin-induced myopathy: 55. Schmidt, A. F. et al. PCSK9 genetic variants and risk of
10. Cannon, C. P. et al. Intensive versus moderate lipid a review and update. Expert Opin. Drug Saf. 10, type 2 diabetes: a mendelian randomisation study.
lowering with statins after acute coronary syndromes. 373–387 (2011). Lancet Diabetes Endocrinol. 5, 97–105 (2017).
N. Engl. J. Med. 350, 1495–1504 (2004). 34. Guengerich, F. P. Cytochrome P450 and chemical 56. Bays, H., Cohen, D. E., Chalasani, N. & Harrison, S. A.,
11. LaRosa, J. C. et al. Intensive lipid lowering with toxicology. Chem. Res. Toxicol. 21, 70–83 (2008). The National Lipid Association’s Statin Safety Task
atorvastatin in patients with stable coronary disease. 35. Bellosta, S. & Corsini, A. Statin drug interactions and Force. An assessment by the Statin Liver Safety
N. Engl. J. Med. 352, 1425–1435 (2005). related adverse reactions. Expert Opin. Drug Saf. 11, Task Force: 2014 update. J. Clin. Lipidol. 8, S47–S57
12. Pedersen, T. R. et al. High-dose atorvastatin versus 933–946 (2012). (2014).
usual-dose simvastatin for secondary prevention after 36. Gupta, A. et al. Adverse events associated with 57. Herrick, C., Bahrainy, S. & Gill, E. A. Statins and the
myocardial infarction: the IDEAL study: a randomized unblinded, but not with blinded, statin therapy in liver. Cardiol. Clin. 33, 257–265 (2015).
controlled trial. JAMA 294, 2437–2445 (2005). the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid- 58. Henderson, L. M., Patel, S., Giordano, T. P., Green, L.
13. de Lemos, J. A. et al. Early intensive versus a delayed Lowering Arm (ASCOT-LLA): a randomised double- & El-Serag, H. B. Statin therapy and serum
conservative simvastatin strategy in patients with blind placebo-controlled trial and its non-randomised transaminases among a cohort of HCV-infected
acute coronary syndromes: phase Z of the A to Z trial. non-blind extension phase. Lancet 389, 2473–2481 veterans. Dig. Dis. Sci. 55, 190–195 (2010).
JAMA 292, 1307–1316 (2004). (2017). 59. Gomez-Dominguez, E., Gisbert, J. P.,
14. Study of the Effectiveness of Additional Reductions in 37. Sever, P. S. et al. Prevention of coronary and stroke Moreno-Monteagudo, J. A., Garcia-Buey, L.
Cholesterol and Homocysteine (SEARCH) Collaborative events with atorvastatin in hypertensive patients who & Moreno-Otero, R. A pilot study of atorvastatin
Group. Intensive lowering of LDL cholesterol with 80 have average or lower-than-average cholesterol treatment in dyslipemid, non-alcoholic fatty liver
mg versus 20 mg simvastatin daily in 12,064 concentrations, in the Anglo-Scandinavian Cardiac patients. Aliment. Pharmacol. Ther. 23, 1643–1647
survivors of myocardial infarction: a double-blind Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): (2006).
randomised trial. Lancet 376, 1658–1669 (2010). a multicentre randomised controlled trial. Lancet 361, 60. Hyogo, H. et al. Efficacy of atorvastatin for the
15. Cholesterol Treatment Trialists Collaboration. The 1149–1158 (2003). treatment of nonalcoholic steatohepatitis with
effects of lowering LDL cholesterol with statin therapy 38. Adhyaru, B. B. & Jacobson, T. A. Unblinded ASCOT dyslipidemia. Metabolism 57, 1711–1718
in people at low risk of vascular disease: meta-analysis study results do not rule out that muscle symptoms (2008).
of individual data from 27 randomised trials. Lancet are an adverse effect of statins. Evid. Based Med. 22, 61. Motamed, N. et al. Non-alcoholic fatty liver disease
380, 581–590 (2012). 210 (2017). (NAFLD) and 10-year risk of cardiovascular
16. Kjekshus, J. et al. Rosuvastatin in older patients with 39. Nissen, S. E. et al. Efficacy and tolerability of diseases. Clin. Res. Hepatol. Gastroenterol. 41,
systolic heart failure. N. Engl. J. Med. 357, 2248–2261 evolocumab versus ezetimibe in patients with 31–38 (2017).
(2007). muscle-related statin intolerance: the GAUSS-3 62. Athyros, V. G. et al. Safety and efficacy of long-term
17. Tavazzi, L. et al. Effect of rosuvastatin in patients randomized clinical trial. JAMA 315, 1580–1590 statin treatment for cardiovascular events in patients
with chronic heart failure (the GISSI-HF trial): (2016). with coronary heart disease and abnormal liver tests
a randomised, double-blind, placebo-controlled trial. 40. Mampuya, W. M. et al. Treatment strategies in in the Greek Atorvastatin and Coronary Heart Disease
Lancet 372, 1231–1239 (2008). patients with statin intolerance: the Cleveland Clinic Evaluation (GREACE) Study: a post-hoc analysis.
18. Baigent, C. et al. The effects of lowering LDL cholesterol experience. Am. Heart J. 166, 597–603 (2013). Lancet 376, 1916–1922 (2010).
with simvastatin plus ezetimibe in patients with chronic 41. Jacobson, T. A., Khan, A., Maki, K. C., Brinton, E. A. 63. Parekh, J., Corley, D. A. & Feng, S. Diabetes,
kidney disease (Study of Heart and Renal Protection): & Cohen, J. D. Provider recommendations for hypertension and hyperlipidemia: prevalence over
a randomised placebo-controlled trial. Lancet 377, patient-reported muscle symptoms on statin therapy: time and impact on long-term survival after liver
2181–2192 (2011). insights from the understanding statin use in America transplantation. Am. J. Transplant. 12, 2181–2187
19. Fellstrom, B. C. et al. Rosuvastatin and cardiovascular and gaps in patient education survey. J. Clin. Lipidol. (2012).
events in patients undergoing hemodialysis. N. Engl. 12, 78–88 (2018). 64. Martin, J. E. et al. Incidence of adverse events
J. Med. 360, 1395–1407 (2009). 42. Banach, M. et al. Statin intolerance — an attempt at a with HMG-CoA reductase inhibitors in liver
20. Wanner, C. et al. Atorvastatin in patients with type 2 unified definition. Position paper from an International transplant patients. Clin. Transplant. 22, 113–119
diabetes mellitus undergoing hemodialysis. N. Engl. Lipid Expert Panel. Arch. Med. Sci. 11, 1–23 (2015). (2008).
J. Med. 353, 238–248 (2005). 43. Guyton, J. R., Bays, H. E., Grundy, S. M. 65. Wiggins, B. S. et al. Recommendations for
21. Bruckert, E., Hayem, G., Dejager, S., Yau, C. & Jacobson, T. A., The National Lipid Association management of clinically significant drug-drug
& Begaud, B. Mild to moderate muscular symptoms Statin Intolerance Panel. An assessment by the Statin interactions with statins and select agents used in
with high-dosage statin therapy in hyperlipidemic Intolerance Panel: 2014 update. J. Clin. Lipidol. 8, patients with cardiovascular disease: a scientific
patients — the PRIMO study. Cardiovasc. Drugs Ther. S72–S81 (2014). statement from the American Heart Association.
19, 403–414 (2005). 44. Graham, J. H. et al. Clinical and economic consequences Circulation 134, e468–e495 (2016).
22. Cohen, J. D., Brinton, E. A., Ito, M. K. & Jacobson, T. A. of statin intolerance in the United States: results from 66. Cash, W. J. et al. Randomized controlled trial
Understanding statin use in America and gaps in patient an integrated health system. J. Clin. Lipidol. 11, 70–79 assessing the effect of simvastatin in primary biliary
education (USAGE): an internet-based survey of 10,138 (2017). cirrhosis. Liver Int. 33, 1166–1174 (2013).
current and former statin users. J. Clin. Lipidol. 6, 45. Athyros, V. G. et al. Effectiveness of ezetimibe alone or 67. Rojas-Fernandez, C. H. et al. An assessment by
208–215 (2012). in combination with twice a week Atorvastatin (10 mg) the Statin Cognitive Safety Task Force: 2014 update.
23. Colantonio, L. D. et al. Adherence to high-intensity for statin intolerant high-risk patients. Am. J. Cardiol. J. Clin. Lipidol. 8, S5–S16 (2014).
statins following a myocardial infarction hospitalization 101, 483–485 (2008). 68. Petersen, R. C. Clinical practice. Mild cognitive
among medicare beneficiaries. JAMA Cardiol. 2, 46. Moriarty, P. M. et al. Efficacy and safety of impairment. N. Engl. J. Med. 364, 2227–2234
890–895 (2017). alirocumab, a monoclonal antibody to PCSK9, in (2011).
24. Rosenson, R. S. et al. An assessment by the Statin statin-intolerant patients: design and rationale of 69. Nasreddine, Z. S. et al. The Montreal Cognitive
Muscle Safety Task Force: 2014 update. J. Clin. Lipidol. ODYSSEY ALTERNATIVE, a randomized phase 3 trial. Assessment, MoCA: a brief screening tool for
8, S58–71 (2014). J. Clin. Lipidol. 8, 554–561 (2014). mild cognitive impairment. J. Am. Geriatr. Soc. 53,
25. Mancini, G. B. et al. Diagnosis, prevention, 47. Orringer, C. E. et al. Update on the use of PCSK9 695–699 (2005).
and management of statin adverse effects inhibitors in adults: recommendations from an Expert 70. Robert, P. et al. Review of Alzheimer’s disease
and intolerance: Canadian Consensus Working Panel of the National Lipid Association. J. Clin. Lipidol. scales: is there a need for a new multi-domain
Group update. Can. J. Cardiol. 32, S35–S65 11, 880–890 (2017). scale for therapy evaluation in medical practice?
(2016). 48. Ridker, P. M. et al. Rosuvastatin to prevent vascular Alzheimers Res. Ther. 2, 24 (2010).
26. Stroes, E. S. et al. Statin-associated muscle symptoms: events in men and women with elevated C-reactive 71. Ott, B. R. et al. Do statins impair cognition? A
impact on statin therapy-European Atherosclerosis protein. N. Engl. J. Med. 359, 2195–2207 (2008). systematic review and meta-analysis of randomized
Society Consensus Panel Statement on Assessment, 49. Sattar, N. et al. Statins and risk of incident diabetes: controlled trials. J. Gen. Intern. Med. 30, 348–358
Aetiology and Management. Eur. Heart J. 36, a collaborative meta-analysis of randomised statin (2015).
1012–1022 (2015). trials. Lancet 375, 735–742 (2010). 72. Shepherd, J. et al. Pravastatin in elderly individuals
27. Awad, K. et al. Efficacy and Safety of alternate-day 50. Ridker, P. M., Pradhan, A., MacFadyen, J. G., Libby, P. at risk of vascular disease (PROSPER): a randomised
versus daily dosing of statins: a systematic review and & Glynn, R. J. Cardiovascular benefits and diabetes controlled trial. Lancet 360, 1623–1630 (2002).
meta-analysis. Cardiovasc. Drugs Ther. 31, 419–431 risks of statin therapy in primary prevention: 73. Heart Protection Study Collaborative Group. MRC/BHF
(2017). an analysis from the JUPITER trial. Lancet 380, Heart Protection Study of antioxidant vitamin
28. Parker, B. A. et al. Effect of statins on skeletal muscle 565–571 (2012). supplementation in 20,536 high-risk individuals:
function. Circulation 127, 96–103 (2013). 51. Amarenco, P. et al. High-dose atorvastatin after stroke a randomised placebo-controlled trial. Lancet 360,
29. Rosenson, R. S. et al. The statin-associated muscle or transient ischemic attack. N. Engl. J. Med. 355, 23–33 (2002).
symptom clinical index (SAMS-CI): revision for clinical 549–559 (2006). 74. Trompet, S. et al. Pravastatin and cognitive function in
use, content validation, and inter-rater reliability. 52. Preiss, D. et al. Risk of incident diabetes with the elderly. Results of the PROSPER study. J. Neurol.
Cardiovasc. Drugs Ther. 31, 179–186 (2017). intensive-dose compared with moderate-dose statin 257, 85–90 (2010).
30. Taylor, B. A. et al. Application of the statin-associated therapy: a meta-analysis. JAMA 305, 2556–2564 75. Goldstein, L. B. et al. Hemorrhagic stroke in the
muscle symptoms-clinical index to a randomized (2011). stroke prevention by aggressive reduction in
trial on statin myopathy. J. Am. Coll. Cardiol. 70, 53. Swerdlow, D. I. et al. HMG-coenzyme A reductase cholesterol levels study. Neurology 70, 2364–2370
1680–1681 (2017). inhibition, type 2 diabetes, and bodyweight: evidence (2008).
768 | DECEMBER 2018 | volume 15 www.nature.com/nrcardio
Reviews
76. Hackam, D. G. et al. Statins and intracerebral 83. Collins, R. et al. MRC/BHF Heart Protection Study of prevent heart attack trial (ALLHAT-LLT). JAMA 288,
hemorrhage: collaborative systematic review cholesterol-lowering with simvastatin in 5963 people 2998–3007 (2002).
and meta-analysis. Circulation 124, 2233–2242 with diabetes: a randomised placebo-controlled trial. 90. GISSI Prevenzione Investigators (Gruppo Italiano
(2011). Lancet 361, 2005–2016 (2003). per lo Studio della Sopravvivenza nell’Infarto
77. Giugliano, R. P. et al. Long-term safety and efficacy 84. Freeman, D. J. et al. Pravastatin and the development Miocardico). Results of the low-dose (20 mg)
of achieving very low levels of low-density lipoprotein of diabetes mellitus: evidence for a protective treatment pravastatin GISSI Prevenzione trial in 4271 patients
cholesterol: a prespecified analysis of the IMPROVE-IT effect in the West of Scotland Coronary Prevention with recent myocardial infarction: do stopped trials
trial. JAMA Cardiol. 2, 547–555 (2017). Study. Circulation 103, 357–362 (2001). contribute to overall knowledge? Ital. Heart J. 1,
78. Hsia, J., MacFadyen, J. G., Monyak, J. & Ridker, P. M. 85. Keech, A. et al. Secondary prevention of 810–820 (2000).
Cardiovascular event reduction and adverse events cardiovascular events with long-term pravastatin in
among subjects attaining low-density lipoprotein patients with diabetes or impaired fasting glucose: Author contributions
cholesterol <50 mg/dl with rosuvastatin. The JUPITER results from the LIPID trial. Diabetes Care 26, Both authors researched data for the article, contributed to
trial (justification for the use of statins in prevention: 2713–2721 (2003). the discussion of content, and wrote, reviewed and edited the
an intervention trial evaluating rosuvastatin). J. Am. 86. Nakamura, H. et al. Primary prevention of manuscript before submission.
Coll. Cardiol. 57, 1666–1675 (2011). cardiovascular disease with pravastatin in Japan
79. Hess, C. N., Low Wang, C. C. & Hiatt, W. R. PCSK9 (MEGA Study): a prospective randomised controlled Competing interests
inhibitors: mechanisms of action, metabolic effects, trial. Lancet 368, 1155–1163 (2006). T.A.J. is a consultant for Amgen and Regeneron/Sanofi. B.B.A.
and clinical outcomes. Annu. Rev. Med. 69, 133–145 87. Downs, J. R. et al. Primary prevention of acute declares no competing interests.
(2018). coronary events with lovastatin in men and women Publisher's note
80. Robinson, J. G. et al. Safety of very low low-density with average cholesterol levels: results of AFCAPS/ Springer Nature remains neutral with regard to jurisdictional
lipoprotein cholesterol levels with alirocumab: pooled TexCAPS. Air Force/Texas Coronary Atherosclerosis claims in published maps and institutional affiliations.
data from randomized trials. J. Am. Coll. Cardiol. 69, Prevention Study. JAMA 279, 1615–1622 (1998).
471–482 (2017). 88. Scandinavian Simvastatin Survival Study Group. Review criteria
81. Schwartz, G. G. et al. Effect of alirocumab, Randomised trial of cholesterol lowering in 4444 We conducted a literature search using Medline, PubMed and
a monoclonal antibody to PCSK9, on long-term patients with coronary heart disease: the Embase and limited the search to the years 2000–2017.
cardiovascular outcomes following acute coronary Scandinavian Simvastatin Survival Study (4S). Search terms included “statin adverse effects”, “statin safety”,
syndromes: rationale and design of the ODYSSEY Lancet 344, 1383–1389 (1994). “statin side effects” and “statin intolerance”. In addition,
outcomes trial. Am. Heart J. 168, 682–689 89. The ALLHAT Officers and Coordinators for the ALLHAT search terms related to specific target organs and adverse
(2014). Collaborative Research Group. Major outcomes in events were also used, including “statin AND muscle, diabe-
82. Rosenson, R. S. et al. Optimizing cholesterol moderately hypercholesterolemic, hypertensive tes, glucose, cognitive function and stroke”. Publications were
treatment in patients with muscle complaints. patients randomized to pravastatin versus usual care: fully reviewed if the abstract suggested that the study was
J. Am. Coll. Cardiol. 70, 1290–1301 (2017). The antihypertensive and lipid-lowering treatment to relevant and used only human data.
NATuRe RevIewS | CARDIOLOgy volume 15 | DECEMBER 2018 | 769
You might also like
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- 2021 VAERS Vaccine Type As of 4/2/2021Document2,342 pages2021 VAERS Vaccine Type As of 4/2/2021PJ MediaNo ratings yet
- Stable Coronary Artery DiseaseDocument7 pagesStable Coronary Artery DiseaseFreddy PanjaitanNo ratings yet
- Statin Toxicity: ReviewDocument23 pagesStatin Toxicity: ReviewRico AditamaNo ratings yet
- Jurnal 4 WordDocument20 pagesJurnal 4 WordSri MaryatiNo ratings yet
- Statin Therapy, Review of Safety and Potential Side EffectsDocument9 pagesStatin Therapy, Review of Safety and Potential Side EffectsDhita Dwi NandaNo ratings yet
- A Pragmatic View of The New Cholesterol Treatment GuidelinesDocument4 pagesA Pragmatic View of The New Cholesterol Treatment GuidelinesMaria Fernanda CoralNo ratings yet
- Stroke Prevention: Multimedia Library ReferencesDocument17 pagesStroke Prevention: Multimedia Library Referencesmochamad rizaNo ratings yet
- Jaha 116 004909 PDFDocument8 pagesJaha 116 004909 PDFLisbeth MarbunNo ratings yet
- 2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskDocument9 pages2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskGandri Ali Ma'suNo ratings yet
- Case Studies in Hyperlipidemia: Michael Cobble, MD, FNLADocument6 pagesCase Studies in Hyperlipidemia: Michael Cobble, MD, FNLAKhánh ChiNo ratings yet
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 pagesEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaNo ratings yet
- MRC-BHF Heart Protection Study PDFDocument16 pagesMRC-BHF Heart Protection Study PDFArif KurniadiNo ratings yet
- Reviews: Statins in The Primary Prevention of Cardiovascular DiseaseDocument12 pagesReviews: Statins in The Primary Prevention of Cardiovascular DiseaseCrischentian BrinzaNo ratings yet
- Statin Intolerance Some Practical HintsDocument7 pagesStatin Intolerance Some Practical HintsTony Miguel Saba SabaNo ratings yet
- 2022 A Stepwise Approach To Prescribing Novel Lipid-Lowering MedicationsDocument11 pages2022 A Stepwise Approach To Prescribing Novel Lipid-Lowering Medicationslakshminivas PingaliNo ratings yet
- s11883-020-00844-wDocument9 pagess11883-020-00844-wMuhammad FauziNo ratings yet
- Estenosis Carotidea - Manejo 2008Document5 pagesEstenosis Carotidea - Manejo 2008fresaopNo ratings yet
- Baseline Low-Density LipoproteinDocument9 pagesBaseline Low-Density LipoproteinjoNo ratings yet
- Improve ItDocument9 pagesImprove ItPaolo Castelblanco VelandiaNo ratings yet
- Current perspectives on the use of statins in the treatment of dyslipidaemic patientsDocument11 pagesCurrent perspectives on the use of statins in the treatment of dyslipidaemic patientssobairnutNo ratings yet
- DyslipidemiaManagement Continuum 2011Document13 pagesDyslipidemiaManagement Continuum 2011Zuleika DöObsönNo ratings yet
- Overcoming Toxicity and Side-Effects of 2014Document14 pagesOvercoming Toxicity and Side-Effects of 2014Andi MuftyNo ratings yet
- E Cacy and Safety of More Intensive Lowering of LDL Cholesterol: A Meta-Analysis of Data From 170 000 Participants in 26 Randomised TrialsDocument12 pagesE Cacy and Safety of More Intensive Lowering of LDL Cholesterol: A Meta-Analysis of Data From 170 000 Participants in 26 Randomised TrialsStefania CristinaNo ratings yet
- Effect of StatinDocument26 pagesEffect of StatinLaluMuhammadSabarSetiawanNo ratings yet
- Use of Statins and The Incidence of Type 2 Diabetes MellitusDocument6 pagesUse of Statins and The Incidence of Type 2 Diabetes MellitusBenji MincholaNo ratings yet
- 3.cardiovascular Risk Stratification and Appropriate Use of Statins in Patients With Systemic Lupus Erythematosus According To Different StrategiesDocument8 pages3.cardiovascular Risk Stratification and Appropriate Use of Statins in Patients With Systemic Lupus Erythematosus According To Different StrategiesSilvia PeresNo ratings yet
- Jurnal 1 GadarDocument6 pagesJurnal 1 GadarDwi FebriyantiNo ratings yet
- Intensive Statin Therapy - A Sea Change in Cardiovascular PreventionDocument3 pagesIntensive Statin Therapy - A Sea Change in Cardiovascular Preventionsyaiful rinantoNo ratings yet
- Prevenção Secundária AafpDocument9 pagesPrevenção Secundária AafpCamila Gomes Santos MoraesNo ratings yet
- Statin Therapyforthe PreventionaDocument15 pagesStatin Therapyforthe PreventionaMr XNo ratings yet
- MRC/BHF Heart Protection Study of Cholesterol Lowering With Simvastatin in 20 536 High-Risk Individuals: A Randomised Placebocontrolled TrialDocument16 pagesMRC/BHF Heart Protection Study of Cholesterol Lowering With Simvastatin in 20 536 High-Risk Individuals: A Randomised Placebocontrolled Trialblopper123No ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolHussain HameedNo ratings yet
- 2018 Cholesterol Guidelines Made Simple ToolDocument22 pages2018 Cholesterol Guidelines Made Simple ToolLeoberto Batista Pereira SobrinhoNo ratings yet
- Role of Statins in Coronary Artery DiseaseDocument6 pagesRole of Statins in Coronary Artery Diseasemonia agni wiyatamiNo ratings yet
- Thompson Et Al 2016 Statin Associated Side EffectsDocument16 pagesThompson Et Al 2016 Statin Associated Side EffectsdriveamadeaNo ratings yet
- Dr. Herianto, SPS - PPTX - STROKE PREVENTION - FinalDocument48 pagesDr. Herianto, SPS - PPTX - STROKE PREVENTION - FinalKrypton Rakehalu KarnadjajaNo ratings yet
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Document4 pagesAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiNo ratings yet
- AaaaDocument5 pagesAaaaDavy JonesNo ratings yet
- Cardiovascular Disease and Risk Management: American Diabetes AssociationDocument9 pagesCardiovascular Disease and Risk Management: American Diabetes AssociationIngrid DCNo ratings yet
- Ya Qoub Et Al 2023 Upfront Combination of Statin and Ezetimibe For Patients With Acute Coronary Syndrome Time For A NewDocument3 pagesYa Qoub Et Al 2023 Upfront Combination of Statin and Ezetimibe For Patients With Acute Coronary Syndrome Time For A NewPPDS PDL JULI 23No ratings yet
- Statin in CKDDocument10 pagesStatin in CKDKartika RahmawatiNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolSafira HalimatussadiahNo ratings yet
- Review of Medical Treatment of Stable Ischemic Heart DiseaseDocument11 pagesReview of Medical Treatment of Stable Ischemic Heart DiseaseSuci NourmalizaNo ratings yet
- Statins in Renal Disease - AndreaDocument18 pagesStatins in Renal Disease - AndreaNawel BenNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- CTTC Estatinas Lancet 2022Document14 pagesCTTC Estatinas Lancet 2022Silvia Montejo FareloNo ratings yet
- Ragu JC 2Document20 pagesRagu JC 2padma ShriniNo ratings yet
- Lipids JBDocument48 pagesLipids JBMuvenn KannanNo ratings yet
- Module 2 Case Analysis JohnDocument8 pagesModule 2 Case Analysis Johnkimwei clintonNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolMuhammad Ali Ridho ShahabNo ratings yet
- Prescribing Pattern of Statins For Primary Prevention of Cardiovascular Diseases in Patients With Type 2 Diabetes: Insights From EthiopiaDocument8 pagesPrescribing Pattern of Statins For Primary Prevention of Cardiovascular Diseases in Patients With Type 2 Diabetes: Insights From EthiopiaSri MaryatiNo ratings yet
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyDocument37 pagesPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaNo ratings yet
- Dislipidemia Ann Int Med Jun 2023Document17 pagesDislipidemia Ann Int Med Jun 2023pepegiovanny100% (1)
- Low-Density Lipoprotein Cholesterol and Stroke: How Low Should We Go?Document3 pagesLow-Density Lipoprotein Cholesterol and Stroke: How Low Should We Go?pitiwararom rachtipatNo ratings yet
- Review: Jane ArmitageDocument10 pagesReview: Jane ArmitageShafira PutriantiNo ratings yet
- Nej MP 1112023Document2 pagesNej MP 1112023Marcella DharmawanNo ratings yet
- Background: Michael - Blazing@dm - Duke.eduDocument9 pagesBackground: Michael - Blazing@dm - Duke.eduDavy JonesNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- 1260-Article Text-5244-1-10-20221110Document26 pages1260-Article Text-5244-1-10-20221110Salma AfifiNo ratings yet
- NCP-Imbalanced Nutrition Less Than Body RequirementsDocument2 pagesNCP-Imbalanced Nutrition Less Than Body RequirementsJon Eric G. Co84% (37)
- 1a2fb7bf1049ac79371db6838638e95dDocument8 pages1a2fb7bf1049ac79371db6838638e95dLavinia DragalauNo ratings yet
- Drugs@FDA - FDA-Approved DrugsDocument3 pagesDrugs@FDA - FDA-Approved DrugsNguyen binhNo ratings yet
- Xylocaine 10% Pump SprayDocument3 pagesXylocaine 10% Pump SprayprofesorbartolomeoNo ratings yet
- Assessment of Attitudes and Perceptions Toward Neurology and Neurosurgery Specialties Among Zambian Medical StudentsDocument14 pagesAssessment of Attitudes and Perceptions Toward Neurology and Neurosurgery Specialties Among Zambian Medical Studentsakmal shahzadNo ratings yet
- DSS Booklet Feb 08 FinalDocument24 pagesDSS Booklet Feb 08 FinalnagadanfNo ratings yet
- Basic Nurse: EnglishDocument145 pagesBasic Nurse: EnglishVenantius Alberto ValentinoNo ratings yet
- Dementia Awareness Training: Stuart Harper-Reynolds - Named Nurse Adult SafeguardingDocument28 pagesDementia Awareness Training: Stuart Harper-Reynolds - Named Nurse Adult SafeguardingJoanne FojaNo ratings yet
- Generalanaesthesia Drdhriti 111223120647 Phpapp01Document64 pagesGeneralanaesthesia Drdhriti 111223120647 Phpapp01Ridha Surya NugrahaNo ratings yet
- Form B: Non-Invasive InvasiveDocument12 pagesForm B: Non-Invasive InvasiveSrikanth KanagasabapathyNo ratings yet
- Treatment and Prevention. Springer-Verlag Berlin Heidelberg: Sehat: Anatomi Dan Fisiologi. Yogyakarta: UGMDocument2 pagesTreatment and Prevention. Springer-Verlag Berlin Heidelberg: Sehat: Anatomi Dan Fisiologi. Yogyakarta: UGMJontor KotlNo ratings yet
- The Bedside Assessment of VertigoDocument5 pagesThe Bedside Assessment of VertigoManuek GarciaNo ratings yet
- Advances in Facial Rejuvenation Botox, HA Dermal Fillers, & Combination TherapyDocument26 pagesAdvances in Facial Rejuvenation Botox, HA Dermal Fillers, & Combination Therapybluestes100% (1)
- FINAL - Changes - NURS 401 Medication Safety and Calculation Quiz Information - 2Document12 pagesFINAL - Changes - NURS 401 Medication Safety and Calculation Quiz Information - 2guneet cheema0% (1)
- Quadas 2Document10 pagesQuadas 2Lya QillahNo ratings yet
- Pfizer CSRDocument68 pagesPfizer CSRShawkat HaiderNo ratings yet
- Endocrine System: Capillary Glucose MonitoringDocument34 pagesEndocrine System: Capillary Glucose Monitoringjoel david knda mj100% (1)
- Igwe R.M. NdubuisiDocument2 pagesIgwe R.M. NdubuisiMark EmakhuNo ratings yet
- 09 Ra Early Warning ScoringDocument3 pages09 Ra Early Warning ScoringREZNo ratings yet
- OxaliplatinDocument3 pagesOxaliplatinMihaela VișanNo ratings yet
- MEDICINE 2 FOR CN UpdatedDocument67 pagesMEDICINE 2 FOR CN UpdatedkezzaNo ratings yet
- Biomedical Engineering Department Organizational StructureDocument3 pagesBiomedical Engineering Department Organizational StructureFlame St100% (2)
- Mechanical Ventilation in Neurocritical Care SettingDocument14 pagesMechanical Ventilation in Neurocritical Care SettingNissi AllineNo ratings yet
- Merise Hospital 1Document5 pagesMerise Hospital 1Amine HaidarNo ratings yet
- Steps in Outbreak InvestigationDocument34 pagesSteps in Outbreak Investigationsharmaine peroNo ratings yet
- ColedocolitiasisDocument25 pagesColedocolitiasisHabib G. Moutran BarrosoNo ratings yet
- Aortic Valve DiseaseDocument63 pagesAortic Valve DiseaseFaridOrahaNo ratings yet
- Safe Infant Sleep - Special ConsiderationsDocument26 pagesSafe Infant Sleep - Special ConsiderationsChrisel Joy Dela CruzNo ratings yet