Download as pdf or txt
You might also like
- Z-LAND - The Survival Horror RPG - CorebookDocument262 pagesZ-LAND - The Survival Horror RPG - CorebookCaio Cézar Dinelli100% (6)
- Acute Kidney InjuryDocument49 pagesAcute Kidney InjuryfikasywNo ratings yet
- Understanding Chronic Kidney Disease: A guide for the non-specialistFrom EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistRating: 4 out of 5 stars4/5 (3)
- SaaS - Primer (VF) PDFDocument20 pagesSaaS - Primer (VF) PDFfiend114100% (2)
- Acute Kidney Injury: Diagnosis and ManagementDocument8 pagesAcute Kidney Injury: Diagnosis and ManagementfadelNo ratings yet
- Acute Kidney InjuryDocument21 pagesAcute Kidney InjuryyinyangdongNo ratings yet
- Joacp 28 386Document11 pagesJoacp 28 386KrisztinaNo ratings yet
- Renal DisordersDocument164 pagesRenal Disorderspblinder1319No ratings yet
- Perioperative Acute Kidney Injury: DR Mukul Kapoor Director Anesthesia, Max Smart Super Specialty Hospital, Saket, DelhiDocument46 pagesPerioperative Acute Kidney Injury: DR Mukul Kapoor Director Anesthesia, Max Smart Super Specialty Hospital, Saket, DelhiChiragNo ratings yet
- Integrated Therapeutics IiDocument165 pagesIntegrated Therapeutics IiSalahadinNo ratings yet
- Injuria Renală Acută CorectatDocument6 pagesInjuria Renală Acută CorectatCaraiman LarisaNo ratings yet
- Acute Kidney Injury For NAUTHDocument39 pagesAcute Kidney Injury For NAUTHfranklin ifioraNo ratings yet
- Aki 6Document12 pagesAki 6WindaNo ratings yet
- AKI Case Discussion 2.0Document3 pagesAKI Case Discussion 2.0Mary Dominique RomoNo ratings yet
- (AKI) Acute Kidney Injury: Daulat Tampubolon, MD Koja HospitalDocument49 pages(AKI) Acute Kidney Injury: Daulat Tampubolon, MD Koja HospitalnaomiNo ratings yet
- Acute Kidney InjuryDocument44 pagesAcute Kidney InjurySuci MayveraNo ratings yet
- Integrated Therapeutics-Ii For 3 Year STS: Chapter-1Document69 pagesIntegrated Therapeutics-Ii For 3 Year STS: Chapter-1Geleta GalataaNo ratings yet
- Materi 7 - Gagal Ginjal AkutDocument30 pagesMateri 7 - Gagal Ginjal AkutTegar Muhamad RifkiNo ratings yet
- Lra ArtigoDocument12 pagesLra ArtigoLuiza Bezerra SoaresNo ratings yet
- Acute Kidney Injury (AKI) : BackgroundDocument22 pagesAcute Kidney Injury (AKI) : BackgroundDeif TunggalNo ratings yet
- Renal Management in The Critically Ill PatientDocument16 pagesRenal Management in The Critically Ill PatientAbygail RHNo ratings yet
- Pathogenesis and Management Sepsis - Aki: Fajar Yuwanto Rsud Abdul Moeloek Bandar LampungDocument21 pagesPathogenesis and Management Sepsis - Aki: Fajar Yuwanto Rsud Abdul Moeloek Bandar LampungNodi Rahma DiniNo ratings yet
- Acute Kidney InjuryDocument9 pagesAcute Kidney InjuryRobertNo ratings yet
- ACUTE KIDNEY INJURY by Dr. Monday Jacob ZaccheausDocument70 pagesACUTE KIDNEY INJURY by Dr. Monday Jacob ZaccheausDr. Amb. Monday ZaccheausNo ratings yet
- Recent Trends in ESRD: Presented By: DR Sayyed Ahmad Moderator: DR Poonam DalalDocument58 pagesRecent Trends in ESRD: Presented By: DR Sayyed Ahmad Moderator: DR Poonam DalalSayyed Ahmad KhursheedNo ratings yet
- Novel Aspects of Pharmacological Therapies For Acute Renal FailureDocument16 pagesNovel Aspects of Pharmacological Therapies For Acute Renal FailureproluvieslacusNo ratings yet
- AKI - Icu Diagnosis and Management: Dr. Muhamed Al Rohani, MD, FISNDocument39 pagesAKI - Icu Diagnosis and Management: Dr. Muhamed Al Rohani, MD, FISNlisaNo ratings yet
- Emergencydepartment Managementofacute Kidneyinjury, Electrolyte Abnormalities, Andrenal Replacementtherapyinthe CriticallyillDocument13 pagesEmergencydepartment Managementofacute Kidneyinjury, Electrolyte Abnormalities, Andrenal Replacementtherapyinthe Criticallyilldogui0071No ratings yet
- Kidney Injury: AcuteDocument14 pagesKidney Injury: AcutealfredoibcNo ratings yet
- ARFDocument19 pagesARFRinky NishadNo ratings yet
- Kdoki y KdigoDocument24 pagesKdoki y KdigoIsrael Armida SodanargNo ratings yet
- Integrated Therapeutics II: January 2020Document700 pagesIntegrated Therapeutics II: January 2020Seyoum Tumsa100% (2)
- Emergencydepartment Managementofacute Kidneyinjury, Electrolyte Abnormalities, Andrenal Replacementtherapyinthe CriticallyillDocument13 pagesEmergencydepartment Managementofacute Kidneyinjury, Electrolyte Abnormalities, Andrenal Replacementtherapyinthe CriticallyillAlejandro OlivaNo ratings yet
- Nephrology DR ZeinabDocument101 pagesNephrology DR ZeinabZeinab Muhammad100% (1)
- Acute Renal Failure and Cardiac SurgeryDocument9 pagesAcute Renal Failure and Cardiac Surgeryserena7205No ratings yet
- Coursematerial 136Document13 pagesCoursematerial 136Nyj QuiñoNo ratings yet
- Prevention and Management of Acute Kidney Injury (Aki)Document29 pagesPrevention and Management of Acute Kidney Injury (Aki)mdonnyyuniarpratamaNo ratings yet
- Acute Kidney Injury: The Right Clinical Information, Right Where It's NeededDocument53 pagesAcute Kidney Injury: The Right Clinical Information, Right Where It's NeededKushal GurungNo ratings yet
- L11 Renal Failure General Approach 230213 002819Document16 pagesL11 Renal Failure General Approach 230213 002819S sNo ratings yet
- Acute Renal FailureDocument14 pagesAcute Renal FailuredrtpkNo ratings yet
- AKI For Diploma Modified 2024Document33 pagesAKI For Diploma Modified 2024wesam.uv55No ratings yet
- RenalFailure StatPearls NCBIBookshelfDocument8 pagesRenalFailure StatPearls NCBIBookshelfMuhammad Qusyairi KamruldzamanNo ratings yet
- Kidney Emergency: M. Syamsul BakhriDocument30 pagesKidney Emergency: M. Syamsul BakhrierahadeNo ratings yet
- Approach To Acute Kidney InjuryDocument44 pagesApproach To Acute Kidney InjuryKue GosongNo ratings yet
- Final AKI For IM 2014Document45 pagesFinal AKI For IM 2014Andika Yusuf RamadhanNo ratings yet
- Chronic Kidney DiseaseDocument5 pagesChronic Kidney DiseaseXtelle Casipit0% (1)
- Acute Kidney Injury 2Document15 pagesAcute Kidney Injury 2Manish VijayNo ratings yet
- Aetiology: Save Time & Improve Your PDP On Patient - Co.ukDocument9 pagesAetiology: Save Time & Improve Your PDP On Patient - Co.ukBaihaqi SaharunNo ratings yet
- Insuficiencia Renal Aguda: Acute Kidney InjuryDocument10 pagesInsuficiencia Renal Aguda: Acute Kidney InjuryVitor Hugo G CorreiaNo ratings yet
- Gagal Ginjal Akut - Bhs InggrisDocument27 pagesGagal Ginjal Akut - Bhs InggrisAgustinusNo ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- Acute Renal FailureDocument41 pagesAcute Renal FailureShams Ul HaqNo ratings yet
- 2 - Diagnostic AKI in ICU From KDIGO To BlomakerDocument80 pages2 - Diagnostic AKI in ICU From KDIGO To Blomakerhartanto_budi6222No ratings yet
- Acute Renal Failure in The ICU PulmCritDocument27 pagesAcute Renal Failure in The ICU PulmCritchadchimaNo ratings yet
- Renal Failure: Yuni ShahrohDocument28 pagesRenal Failure: Yuni ShahrohaburisyaNo ratings yet
- Acute Kidney InjuryDocument17 pagesAcute Kidney InjuryPrecious C. MamaradloNo ratings yet
- Síndrome Hepatorrenal Cirrosis Eur Gast J 2021Document9 pagesSíndrome Hepatorrenal Cirrosis Eur Gast J 2021Anabel GonzalezNo ratings yet
- Acute Kidney Injury AKIDocument6 pagesAcute Kidney Injury AKIfazeel shah vlogsNo ratings yet
- Lesion Renal Aguda NursingDocument6 pagesLesion Renal Aguda NursingYesica Katerine Novoa GarciaNo ratings yet
- AKI LectureDocument95 pagesAKI LectureDaryl Gay NanoNo ratings yet
- 3308-Article Text-12253-1-10-20231130Document8 pages3308-Article Text-12253-1-10-20231130Hubert AndrewNo ratings yet
- Restoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisFrom EverandRestoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisNo ratings yet
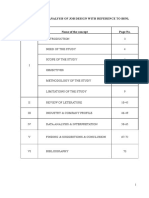
- Job Designing Analysis BSNLDocument75 pagesJob Designing Analysis BSNLpavanNo ratings yet
- The Bobo Doll ExperimentDocument23 pagesThe Bobo Doll ExperimentManiya Dianne ReyesNo ratings yet
- Karachi Public School Cambridge Section Class: IX English Language Midyear Syllabus Session: 2021 - 22Document2 pagesKarachi Public School Cambridge Section Class: IX English Language Midyear Syllabus Session: 2021 - 22Ameer hamzaNo ratings yet
- Term Paper Final 2Document32 pagesTerm Paper Final 2buronjirahmae137No ratings yet
- Worksheet #3 - BalicatDocument2 pagesWorksheet #3 - BalicatZULLIENE RHEZZY BALICATNo ratings yet
- Particle Physics (Physics Factsheet)Document27 pagesParticle Physics (Physics Factsheet)Utsav Dhakal83% (6)
- Public Info - FAKE NEWS - 17!10!04 (Reviewed)Document263 pagesPublic Info - FAKE NEWS - 17!10!04 (Reviewed)Calvin Patrick DomingoNo ratings yet
- PerDev Learning ActivityDocument4 pagesPerDev Learning ActivitydwacindyfjNo ratings yet
- The Field of Engineering ManagementDocument15 pagesThe Field of Engineering ManagementBelle SolaceNo ratings yet
- Access To Childbirth CareDocument67 pagesAccess To Childbirth CareemeNo ratings yet
- Ekman 1992Document33 pagesEkman 1992Zaima Sartaj TaheriNo ratings yet
- Probability and StatisticsDocument17 pagesProbability and StatisticsM. Amin QureshiNo ratings yet
- REINVENTING EDEN. The Fate of Nature in Western Culture. Carolyn Merchant, Second Edition (Updated With A New Foreword and Afterword), 2013Document334 pagesREINVENTING EDEN. The Fate of Nature in Western Culture. Carolyn Merchant, Second Edition (Updated With A New Foreword and Afterword), 2013Francis RijnaNo ratings yet
- PMLS 2 Lesson 1Document4 pagesPMLS 2 Lesson 1Void MelromarcNo ratings yet
- 5 2 ConceptualDocument4 pages5 2 ConceptualArfiNo ratings yet
- @2018 Extreme Gradient BoostingDocument12 pages@2018 Extreme Gradient BoostinghnavastNo ratings yet
- English I C2Document10 pagesEnglish I C2José Sánchez100% (1)
- Pilot Testing, Monitoring and Evaluating The Implementation of The CurriculumDocument34 pagesPilot Testing, Monitoring and Evaluating The Implementation of The CurriculumJoshua Dela Cruz Rogador100% (2)
- Biomarkers of Bone Health and Osteoporosis Risk Symposium On Diet and Bone HealthDocument6 pagesBiomarkers of Bone Health and Osteoporosis Risk Symposium On Diet and Bone HealthDaniel SilvaNo ratings yet
- R. Molski, Polish Antitrust Law in Its Fight Against Cartels - Awaiting A BreakthroughDocument28 pagesR. Molski, Polish Antitrust Law in Its Fight Against Cartels - Awaiting A Breakthroughcsair1No ratings yet
- The Neuroscience Joyful Education Judy Willis MDDocument6 pagesThe Neuroscience Joyful Education Judy Willis MDcecilitusNo ratings yet
- My Sexual Autobiography Vol 1Document218 pagesMy Sexual Autobiography Vol 1megan fisher50% (2)
- Principles of Electrical Engineering (ECE) : Unit 1 DC CircuitsDocument2 pagesPrinciples of Electrical Engineering (ECE) : Unit 1 DC CircuitsPavan KumarNo ratings yet
- Final Reflective Essay - Christina KulasekereDocument7 pagesFinal Reflective Essay - Christina Kulasekereapi-302753885No ratings yet
- Standard Styles in Related Literature, References, or CitationsDocument2 pagesStandard Styles in Related Literature, References, or CitationsGuinevere B.No ratings yet
- Transmission Cycle of InfectionDocument22 pagesTransmission Cycle of InfectionMikeNo ratings yet
- Mark Scheme (Results) : January 2018Document25 pagesMark Scheme (Results) : January 2018Mohamed Nazeer Falah AhamadNo ratings yet
- Masters ThesisDocument61 pagesMasters ThesissampathdtNo ratings yet