Download as pdf or txt
You might also like
- Clinical Reasoing Cycle Textbook Answers Tracy-Levett JonesDocument41 pagesClinical Reasoing Cycle Textbook Answers Tracy-Levett JonesCaleb Fellowes81% (27)
- RPAH Elimination Diet Handbook With Food Shopping Guide PDFDocument33 pagesRPAH Elimination Diet Handbook With Food Shopping Guide PDFmalamatiyya33% (6)
- DeVry HIT 111 All Discussions - LatestDocument11 pagesDeVry HIT 111 All Discussions - Latestshonwilllen0% (1)
- Pure Bodybuilding - PPLDocument128 pagesPure Bodybuilding - PPLsw0nlessNo ratings yet
- Metabolic Disease Case Study Learning ActivityDocument8 pagesMetabolic Disease Case Study Learning ActivityKhali Sciola0% (1)
- Cms Psych 3.odtDocument19 pagesCms Psych 3.odtwalt65No ratings yet
- Case Write Up - Harmeet - Multinodular GoitreDocument29 pagesCase Write Up - Harmeet - Multinodular GoitreShalini Soorya71% (7)
- Case Report DengueDocument16 pagesCase Report DengueAimanazrul ZainudinNo ratings yet
- INTUSSUSCEPTIONDocument43 pagesINTUSSUSCEPTIONValarmathi100% (3)
- All CasesDocument32 pagesAll CasesMona NasrNo ratings yet
- Medicine OSCEDocument21 pagesMedicine OSCEAakash KsNo ratings yet
- GPSN StemsDocument7 pagesGPSN StemsRohit SharmaNo ratings yet
- Chronic Heart FailureDocument3 pagesChronic Heart FailurearavindNo ratings yet
- Mentalt Health 6-116Document16 pagesMentalt Health 6-116Osama NasrNo ratings yet
- Patient InformationDocument7 pagesPatient Informationفاطمہ خالدNo ratings yet
- Nursing Management of A Patient With: HyperthyroidismDocument31 pagesNursing Management of A Patient With: Hyperthyroidismember parkNo ratings yet
- D2-Milla - Telemed Written Report 4Document5 pagesD2-Milla - Telemed Written Report 4Gabriel MillaNo ratings yet
- 3 HPLCDocument9 pages3 HPLClorrainebarandonNo ratings yet
- 11mastering Medical Long CaseDocument42 pages11mastering Medical Long CaseAthirahRaraNo ratings yet
- Case No. 6 Lost The PlotDocument7 pagesCase No. 6 Lost The PlotNermeen AlrajhiNo ratings yet
- Medsurg Careplan 1Document6 pagesMedsurg Careplan 1Melanie DuttonNo ratings yet
- Family Medicine - General Practice MEQ 2006Document6 pagesFamily Medicine - General Practice MEQ 2006jermie22100% (1)
- Rle - Module Sample Course Code Course Title Level Offering Clinical Area of Assignment Date of Exposure No. of HoursDocument9 pagesRle - Module Sample Course Code Course Title Level Offering Clinical Area of Assignment Date of Exposure No. of HoursBrose Wayne CapizNo ratings yet
- Alcohol Withdrawal Case ConferenceDocument6 pagesAlcohol Withdrawal Case ConferenceGhazal KangoNo ratings yet
- Soup Notes Templateweek 91Document7 pagesSoup Notes Templateweek 91emmah mwendeNo ratings yet
- Clinical CasesDocument2 pagesClinical CasesAshish R. JadhavNo ratings yet
- Case For Small Group Discussion For StudentsDocument4 pagesCase For Small Group Discussion For StudentsMuhmd shiyas.HNo ratings yet
- Course Code Course Title Level Offering Clinical Area of Assignment Date of Exposure No. of HoursDocument9 pagesCourse Code Course Title Level Offering Clinical Area of Assignment Date of Exposure No. of HoursIsaiah RabangNo ratings yet
- ADDison LovaanDocument4 pagesADDison Lovaaneraj rahmanNo ratings yet
- Assignment 3Document5 pagesAssignment 3api-577583685No ratings yet
- Geriatrics For StudentsDocument88 pagesGeriatrics For StudentsRv DeanNo ratings yet
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 pagesMedical Case 1: Language Centre of Malahayati University at 2010putri1114No ratings yet
- Acute Neurology Clinical Vignettes 1Document8 pagesAcute Neurology Clinical Vignettes 1coolblue89No ratings yet
- Blake, Baroni, Rotenberg, Zhang Part 4Document7 pagesBlake, Baroni, Rotenberg, Zhang Part 4Tanner Jameson BlakeNo ratings yet
- Amc Psychiatric 2005 To 2009Document28 pagesAmc Psychiatric 2005 To 2009Sindu Sai100% (1)
- Cagayan State University - College of Medicine and Surgery Clinical Neurology Oral Revalida, May 4, 2016Document4 pagesCagayan State University - College of Medicine and Surgery Clinical Neurology Oral Revalida, May 4, 2016Michelle Vera GabunNo ratings yet
- Mental Health Case StudyDocument14 pagesMental Health Case Studyapi-663879558No ratings yet
- MH Case StudyDocument17 pagesMH Case StudyS. JacobsNo ratings yet
- Case Presentation NewDocument13 pagesCase Presentation Newsherief maroufNo ratings yet
- Shelf IM Patient NotesDocument6 pagesShelf IM Patient NotesRuth SanmooganNo ratings yet
- Aggression and Homicidal Thoughts in A Patient With Primary Hyperparathyroidism A Case ReportDocument3 pagesAggression and Homicidal Thoughts in A Patient With Primary Hyperparathyroidism A Case ReportKimberly SemenzaNo ratings yet
- Telemed Written Report 4Document5 pagesTelemed Written Report 4Gabriel MillaNo ratings yet
- Groups ABCD - Family Medicine End Block QuestionsDocument10 pagesGroups ABCD - Family Medicine End Block QuestionsHisham ChomanyNo ratings yet
- Rta and Substance Use (Autosaved) - 1Document34 pagesRta and Substance Use (Autosaved) - 1Akampurira IanNo ratings yet
- Is She Depressed???.": What Is Your Differential Diagnosis What Other Information Would You Like To Know About Mrs. X ?Document5 pagesIs She Depressed???.": What Is Your Differential Diagnosis What Other Information Would You Like To Know About Mrs. X ?Doha EbedNo ratings yet
- MH Case StudyDocument11 pagesMH Case Studyapi-455565203No ratings yet
- Case Pres.Document22 pagesCase Pres.Cherie MayNo ratings yet
- NBME Sample QuestionsDocument144 pagesNBME Sample QuestionsYear Tentacle100% (3)
- Case StudyDocument3 pagesCase StudyAmila RahmahNo ratings yet
- Soap 5 - Geriatric 65Document13 pagesSoap 5 - Geriatric 65api-482726932No ratings yet
- Case 40 2015 A 40-Year-Old Homeless Woman With Headache Hypertension and PsychosisDocument8 pagesCase 40 2015 A 40-Year-Old Homeless Woman With Headache Hypertension and Psychosisapi-344719326No ratings yet
- Practice Case: Vestibular DysfunctionDocument4 pagesPractice Case: Vestibular DysfunctionMarvin Luis MontillaNo ratings yet
- Case Study On AlcoholismDocument2 pagesCase Study On Alcoholismdenebrench23No ratings yet
- Running Head: CASE STUDY 1Document17 pagesRunning Head: CASE STUDY 1api-507206712No ratings yet
- Matt DeHart: Eastern Maine Medical Center Emergency Department ReportDocument5 pagesMatt DeHart: Eastern Maine Medical Center Emergency Department ReportNational Post100% (1)
- Depression Case StudyDocument9 pagesDepression Case StudySara Lynn LeSage86% (7)
- Communication CasesDocument146 pagesCommunication CasesMohammadAbdurRahmanNo ratings yet
- Abuajela Sreh - St5 Gastroenterology - Sheffield Teaching Hospitals 1 4 / 0 1 / 2 0 2 2Document48 pagesAbuajela Sreh - St5 Gastroenterology - Sheffield Teaching Hospitals 1 4 / 0 1 / 2 0 2 2sryh2012No ratings yet
- Casos Clínicos UDocument12 pagesCasos Clínicos USARA DANIELA RIOS RIVEROSNo ratings yet
- SURVIVE THE HOSPITAL, BE YOUR OWN ADVOCATE, DON'T GET NEGLECTEDFrom EverandSURVIVE THE HOSPITAL, BE YOUR OWN ADVOCATE, DON'T GET NEGLECTEDNo ratings yet
- Best Clinical Guide for Your Family and Your Doctor: The Helper in Critical Health SituationsFrom EverandBest Clinical Guide for Your Family and Your Doctor: The Helper in Critical Health SituationsNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Facial Pigmentation Impacts Quality of Life Regardless of Clinical SeverityDocument7 pagesFacial Pigmentation Impacts Quality of Life Regardless of Clinical SeverityMeta SakinaNo ratings yet
- Submaximal Fitness Tests in Team SportsDocument22 pagesSubmaximal Fitness Tests in Team SportsRoberto Portillo GarcíaNo ratings yet
- Dettol FinalDocument20 pagesDettol Finalsili core50% (2)
- EE 123-Problem-1Document4 pagesEE 123-Problem-1Email TugasNo ratings yet
- A.Examine A Healthcare Organization That Has Significance To You,...Document7 pagesA.Examine A Healthcare Organization That Has Significance To You,...DrogNo ratings yet
- Civic Welfare Training Service-1: Certified To ISO 9001:2015 CERT. No.: 50500643QM15Document7 pagesCivic Welfare Training Service-1: Certified To ISO 9001:2015 CERT. No.: 50500643QM15ciedelle arandaNo ratings yet
- HEO Hydraulic Excavator NC II CBCDocument62 pagesHEO Hydraulic Excavator NC II CBCRoi Jason Carillo DetorresNo ratings yet
- DLP - Grade 8 - Diseases That Result From Nutrient Deficiency and Ingestion of Harmful Substances. EditedDocument9 pagesDLP - Grade 8 - Diseases That Result From Nutrient Deficiency and Ingestion of Harmful Substances. Editedmars100% (3)
- Design, User Experience, and Usability: Marcelo M. Soares Elizabeth Rosenzweig Aaron MarcusDocument500 pagesDesign, User Experience, and Usability: Marcelo M. Soares Elizabeth Rosenzweig Aaron MarcusJosé Carlos Gamero LeónNo ratings yet
- ToR Consultant - Information Technology, NHSRCDocument5 pagesToR Consultant - Information Technology, NHSRCHanumant NNo ratings yet
- 383WKS 1 Forest Harvesting Trees Around Power LinesDocument80 pages383WKS 1 Forest Harvesting Trees Around Power LinesKevin DucusinNo ratings yet
- Final WHH NEWSLETTER ISSUE 1 - KINAKONI - ImposedDocument6 pagesFinal WHH NEWSLETTER ISSUE 1 - KINAKONI - ImposedinklabdigitalprintersNo ratings yet
- Reading Log - Social Emotional LearningDocument5 pagesReading Log - Social Emotional Learningapi-497970481No ratings yet
- Health & Wellness (October 2021)Document20 pagesHealth & Wellness (October 2021)Watertown Daily Times100% (1)
- Meera NowDocument181 pagesMeera NowelpidaNo ratings yet
- Literature Review The Perception of The Impact of Teachers Teaching Styles On Students Learning SDocument12 pagesLiterature Review The Perception of The Impact of Teachers Teaching Styles On Students Learning SIshika PrasadNo ratings yet
- Riska Amelia, A. Mushawwir Taiyeb, Irma Suryani IdrisDocument11 pagesRiska Amelia, A. Mushawwir Taiyeb, Irma Suryani IdrisÈkä Sêtýä PrätämäNo ratings yet
- Cancer - 2005 - Van Gogh - The Efficacy of Voice Therapy in Patients After Treatment For Early Glottic CarcinomaDocument11 pagesCancer - 2005 - Van Gogh - The Efficacy of Voice Therapy in Patients After Treatment For Early Glottic CarcinomaNathalia Dos ReisNo ratings yet
- Physical Education and Health 11: Learning Activity Sheet (Week 5-6) Personal Safety Background InformationDocument4 pagesPhysical Education and Health 11: Learning Activity Sheet (Week 5-6) Personal Safety Background InformationRheena-Ann Dupale PadillaNo ratings yet
- Central Council For: in HomoeopathyDocument18 pagesCentral Council For: in Homoeopathy9891233665No ratings yet
- Corporate Social Responsibility of TOP 10 Corporations in The PhilippinesDocument8 pagesCorporate Social Responsibility of TOP 10 Corporations in The PhilippinesEmJay Nonoi0% (1)
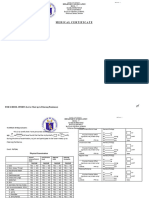
- Medical Certificate MC Form 1 All Sports EventsDocument2 pagesMedical Certificate MC Form 1 All Sports EventsKriston CabilesNo ratings yet
- How Can Weak Student Can Be Improve D?Document31 pagesHow Can Weak Student Can Be Improve D?Muhammad Ali100% (1)
- Preliminary Residents' Society Budget - Oaken ResidencesDocument2 pagesPreliminary Residents' Society Budget - Oaken Residencestangbinbin2007No ratings yet
- Acute Renal Failure Case StudyDocument19 pagesAcute Renal Failure Case StudyHomework PingNo ratings yet
- Ot 1Document29 pagesOt 1CTV CalgaryNo ratings yet
- How Much Responsibility Can We Give Twelve-Year-Olds - An AnalysisDocument6 pagesHow Much Responsibility Can We Give Twelve-Year-Olds - An AnalysisAaron DoguilesNo ratings yet