Download as pdf or txt
You might also like
- Nefro334REVIEWMagnesiumsupplementationtopreventrecurrenceofrenalstonesOKDocument6 pagesNefro334REVIEWMagnesiumsupplementationtopreventrecurrenceofrenalstonesOKDragoljub DjordjevicNo ratings yet
- Bioavailability of Magnesium SaltsDocument3 pagesBioavailability of Magnesium Saltssantana20130% (1)
- Effects of Inositol HexaphosphateDocument2 pagesEffects of Inositol HexaphosphateManeesha KhalseNo ratings yet
- Veterinary Clinics: Magnesium: A Quick ReferenceDocument4 pagesVeterinary Clinics: Magnesium: A Quick ReferenceDanilo JimenezNo ratings yet
- Bioavailability of Magnesium Salts PDFDocument3 pagesBioavailability of Magnesium Salts PDFsantana2007No ratings yet
- Electrolyte Disorders With Platinum-Based ChemotheDocument14 pagesElectrolyte Disorders With Platinum-Based ChemotheMarisa IzzaNo ratings yet
- A Quick Reference On MagnesiumDocument5 pagesA Quick Reference On Magnesiumrose.msrNo ratings yet
- MagnesiumDocument26 pagesMagnesiumOjan Benard LeoNo ratings yet
- The Role of Magnesium in Clinical PracticeDocument20 pagesThe Role of Magnesium in Clinical PracticeMagdalena Dwiyani HutajuluNo ratings yet
- Jurnal Anemia DefisiensiDocument3 pagesJurnal Anemia DefisiensiAirin Nurul Syahdiva RamliNo ratings yet
- Ijms 16 23076Document18 pagesIjms 16 23076Putri DhayatiNo ratings yet
- ManisumDocument5 pagesManisumvaviga7591No ratings yet
- Nieuw 1Document14 pagesNieuw 1Jasmijn AlmuliNo ratings yet
- Magnesium:: A Mineral With Multiple ApplicationsDocument2 pagesMagnesium:: A Mineral With Multiple Applicationsnadin nNo ratings yet
- Magnesium Salts ComparisonDocument1 pageMagnesium Salts ComparisonSanjay NavaleNo ratings yet
- Bioavailability of Magnesium CompoundsDocument9 pagesBioavailability of Magnesium CompoundsJo KNo ratings yet
- MAA Ossoral DexaDocument33 pagesMAA Ossoral DexaDitaAnggaraKusumaNo ratings yet
- UV, CE, DIffusionDocument49 pagesUV, CE, DIffusionDoaa FarahNo ratings yet
- Dietary Oxalate and Kidney Stone Formation - PMCDocument12 pagesDietary Oxalate and Kidney Stone Formation - PMCRonNo ratings yet
- 1471 4676 1 SMDocument5 pages1471 4676 1 SMAhmad AinurofiqNo ratings yet
- Elevated Urinary Excretion of Aluminium and Iron in Multiple SclerosisDocument8 pagesElevated Urinary Excretion of Aluminium and Iron in Multiple SclerosisIchim MadalinaNo ratings yet
- NONE88Document4 pagesNONE88Sukma EffendyNo ratings yet
- Human Mineral 2Document24 pagesHuman Mineral 2Nitay SorkarNo ratings yet
- Zirconio Caracteristicas FarmacoDocument11 pagesZirconio Caracteristicas FarmacoMARIA LEIVANo ratings yet
- PIIS0272638623010065Document11 pagesPIIS0272638623010065Mohammad YaseenNo ratings yet
- Biological Importance of MagnasiumDocument27 pagesBiological Importance of Magnasiumwarrierabhay100% (1)
- Magnesium Oxide NanoparticlesDocument10 pagesMagnesium Oxide Nanoparticleswaheed akramNo ratings yet
- Nutrients 13 00062Document13 pagesNutrients 13 00062Pedro alexNo ratings yet
- Reddy 2018Document6 pagesReddy 2018Yosoa OktavianusNo ratings yet
- Magnesium: 11.1 Tissue Distribution and Biological Role of MagnesiumDocument13 pagesMagnesium: 11.1 Tissue Distribution and Biological Role of MagnesiumSamuel Rudolf Maranatha JulioNo ratings yet
- Absorption of Magnesium CompoundsDocument8 pagesAbsorption of Magnesium CompoundsJo KNo ratings yet
- Pharmacokinetic Profile of Oral Magnesium HydroxideDocument6 pagesPharmacokinetic Profile of Oral Magnesium HydroxideRegina Marsha XaveriaNo ratings yet
- Calcium Oxalate Nephrolithiasis: An Easy Way To Detect An Imbalance Between Promoting and Inhibiting FactorsDocument7 pagesCalcium Oxalate Nephrolithiasis: An Easy Way To Detect An Imbalance Between Promoting and Inhibiting FactorsJames TerryNo ratings yet
- Bioavailability and Pharmacokinetics of Magnesium AfterDocument13 pagesBioavailability and Pharmacokinetics of Magnesium Afternoviyanti christianaNo ratings yet
- Zinc: 12.1 Role of Zinc in Human Metabolic ProcessesDocument16 pagesZinc: 12.1 Role of Zinc in Human Metabolic ProcessesLuis Lorenzo Rodriguez RojasNo ratings yet
- Calcium Iron AbsorptionDocument2 pagesCalcium Iron AbsorptionwaitNo ratings yet
- Nutrients: Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked To Its DeficiencyDocument44 pagesNutrients: Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked To Its DeficiencylianaidrisNo ratings yet
- Assessmentof MagnesiumStatusDocument6 pagesAssessmentof MagnesiumStatusVasanth KolurNo ratings yet
- Neproku JurnalDocument11 pagesNeproku Jurnalarum damayantiNo ratings yet
- Wide Mag Deficiency PathDocument8 pagesWide Mag Deficiency PathZaid Al OmariNo ratings yet
- Bmes Abstract Roslyn VansickleDocument1 pageBmes Abstract Roslyn Vansickleapi-414830668No ratings yet
- PDF Translator 1582003500196 PDFDocument7 pagesPDF Translator 1582003500196 PDFNurul HabibahNo ratings yet
- GaoSCANNING2021 5530788Document9 pagesGaoSCANNING2021 5530788Lan Đàm Thị PhươngNo ratings yet
- The Nutritional Relationships of MagnesiumDocument5 pagesThe Nutritional Relationships of MagnesiumwynvelNo ratings yet
- Admin, Journal Manager, 5 - YuliaDocument9 pagesAdmin, Journal Manager, 5 - YuliaRizka syftriNo ratings yet
- Castig Lion I 2013Document12 pagesCastig Lion I 2013Reinhart SalimNo ratings yet
- MG Catalase Sejal Et Al TPPSDocument8 pagesMG Catalase Sejal Et Al TPPSAhmad AliNo ratings yet
- (Al-Snafi, 2018) SeledriDocument14 pages(Al-Snafi, 2018) SeledrinanaNo ratings yet
- Radiology, Hospital, Assistance Making: of We Owe Com-OnDocument9 pagesRadiology, Hospital, Assistance Making: of We Owe Com-OnSanja KaranovicNo ratings yet
- Consumo Diario de Calcio y Oxalacetato en Humanos 2Document5 pagesConsumo Diario de Calcio y Oxalacetato en Humanos 2Brain LongwoodNo ratings yet
- Increased Bone Calcium Dissociation in Lead-Exposed Rats: Universa MedicinaDocument8 pagesIncreased Bone Calcium Dissociation in Lead-Exposed Rats: Universa MedicinaIfiq Budiyan NazarNo ratings yet
- Long-Term Management of Organic Acidurias (OA)Document1 pageLong-Term Management of Organic Acidurias (OA)A LNo ratings yet
- Foods 12 01058Document17 pagesFoods 12 01058Pham Chi LanNo ratings yet
- Analytical Assessment Regarding Individuals With Backbone Carved AtrophyctzxqDocument1 pageAnalytical Assessment Regarding Individuals With Backbone Carved Atrophyctzxqguiltystool8No ratings yet
- Therapeutic Uses of Magnesium: Complementary and Alternative MedicineDocument6 pagesTherapeutic Uses of Magnesium: Complementary and Alternative MedicinedanielguerinNo ratings yet
- Can Lemon Juice Be An Alternative To Potassium CitrateDocument5 pagesCan Lemon Juice Be An Alternative To Potassium CitrateerayNo ratings yet
- Functioning of Potassium and Magnesium in PhotosynDocument18 pagesFunctioning of Potassium and Magnesium in PhotosynMuhammad Imam NugrahaNo ratings yet
- Riaz, 2019Document8 pagesRiaz, 2019Di GoNo ratings yet
- Rafia Roll No 12 Comparison of The Histopathological Effects of Selenium Nanoparticles and Cerium Oxide Nanoparticles in CadmiumDocument6 pagesRafia Roll No 12 Comparison of The Histopathological Effects of Selenium Nanoparticles and Cerium Oxide Nanoparticles in CadmiumMehram JuttNo ratings yet
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet
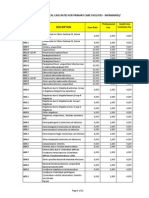
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- Mesothelioma 20.3.19Document33 pagesMesothelioma 20.3.19PradeepNo ratings yet
- Design AI Platform Using Fuzzy Logic Technique To Diagnose Kidney DiseasesDocument9 pagesDesign AI Platform Using Fuzzy Logic Technique To Diagnose Kidney DiseasesTELKOMNIKANo ratings yet
- Herbs For Natural: Health & HealingDocument15 pagesHerbs For Natural: Health & HealingjamatidoNo ratings yet
- Urine Crystals (Crystalluria)Document17 pagesUrine Crystals (Crystalluria)John AsamaohNo ratings yet
- Symtoms of The Kidney StoneDocument4 pagesSymtoms of The Kidney StoneabelNo ratings yet
- 3.MCQ Good PushDocument19 pages3.MCQ Good Pushanderson ndabishakaNo ratings yet
- UGA Reports Cancer Breakthrough: Top 3 Health Concerns: Poor Air, Alcohol, TraumaDocument14 pagesUGA Reports Cancer Breakthrough: Top 3 Health Concerns: Poor Air, Alcohol, TraumaCassandra_Maca_6324No ratings yet
- EC, SIF and PhilHealthDocument13 pagesEC, SIF and PhilHealthMarshan GualbertoNo ratings yet
- Pathophysiology of Nephrolithiasis PDFDocument9 pagesPathophysiology of Nephrolithiasis PDFLayuganlovelyNo ratings yet
- Biologic Crisis:: Prepared By: Recitas, Anna Lou G. BSN-4 Sn-DoscstDocument64 pagesBiologic Crisis:: Prepared By: Recitas, Anna Lou G. BSN-4 Sn-DoscstDonna Solamo TalabocNo ratings yet
- News at NUST: ISAK Donates Measuring Equipment To Sports ScienceDocument8 pagesNews at NUST: ISAK Donates Measuring Equipment To Sports ScienceRatanang Rj NokoNo ratings yet
- Nutri Lab P1p2rbe Exam 2 2Document16 pagesNutri Lab P1p2rbe Exam 2 2SandyNo ratings yet
- NICE GuidelineDocument143 pagesNICE GuidelinewindyayudhiaNo ratings yet
- Posttest. Renal DisordersDocument3 pagesPosttest. Renal Disordersjbagacay100% (3)
- Urologic Diseases American2Document334 pagesUrologic Diseases American2Sii Laddiees CuwekkNo ratings yet
- Nephrolithiasis in A 9 Year OldDocument4 pagesNephrolithiasis in A 9 Year OldJasmin Kae SistosoNo ratings yet
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- Uri Flush 3 Liquid Stones ProblemDocument4 pagesUri Flush 3 Liquid Stones ProblemSourabh KoshtaNo ratings yet
- Genitourinary UltrasoundDocument215 pagesGenitourinary UltrasoundAnselmus Regie100% (4)
- March 2022 RecallsDocument292 pagesMarch 2022 RecallsNguyễn Nhật HoàngNo ratings yet
- Characterization of Renal Stones Using Gsi: Patient HistoryDocument2 pagesCharacterization of Renal Stones Using Gsi: Patient HistoryAlreem AlhajryNo ratings yet
- Effect of Phenolic Compounds From Bergenia Ciliata Leaves On Experimental Kidney StonesDocument4 pagesEffect of Phenolic Compounds From Bergenia Ciliata Leaves On Experimental Kidney StonesSilfia LayliyahNo ratings yet
- Health Teaching PlanDocument3 pagesHealth Teaching PlanJheanAlphonsineT.MeansNo ratings yet
- All BaseDocument281 pagesAll BaseafrahNo ratings yet
- Case Batu Ureter EditDocument22 pagesCase Batu Ureter EditAdinda NatasyaNo ratings yet
- Imaging of Double J Ureteral Stents - What To Look For? PDFDocument46 pagesImaging of Double J Ureteral Stents - What To Look For? PDFJade Kenneth Gonzales LomansocNo ratings yet
- McCance Patho Review QsDocument17 pagesMcCance Patho Review Qsiamdara100% (1)
- Patofisiologi Dan Pencegahan BSKDocument19 pagesPatofisiologi Dan Pencegahan BSKHendry Cleodora RomeoNo ratings yet
- Therapeutic Diet PDFDocument3 pagesTherapeutic Diet PDFJagveer ChauhanNo ratings yet