Download as pdf or txt
You might also like
- Self-Reporting Booklet - Am I An ADHDerDocument73 pagesSelf-Reporting Booklet - Am I An ADHDerOmayra Sánchez González100% (2)
- Sports PhysicalDocument6 pagesSports Physicalapi-671085061No ratings yet
- Poultry Disease MCQs - Veterinary Online QuizzesDocument4 pagesPoultry Disease MCQs - Veterinary Online Quizzesbasit abdulNo ratings yet
- 2022 ART Revised Kenyan GuidelinesDocument39 pages2022 ART Revised Kenyan GuidelinesJOHN KAMAUNo ratings yet
- Reported Pathological ChildhoodDocument7 pagesReported Pathological ChildhoodMartha Lucía Triviño LuengasNo ratings yet
- Associations Between Four Types of Childhood Neglect and Personality Disorder Symptoms During Adolescence and Early Adulthood: Findings of A Community-Based Longitudinal StudyDocument17 pagesAssociations Between Four Types of Childhood Neglect and Personality Disorder Symptoms During Adolescence and Early Adulthood: Findings of A Community-Based Longitudinal StudyUmer FarooqNo ratings yet
- Factors Affecting The Diagnosis and Prediction of PTSD PDFDocument8 pagesFactors Affecting The Diagnosis and Prediction of PTSD PDFAGRANo ratings yet
- (PERSONALIDADE) Childhood Maltreatment Increases Risk For Personality Disorders During Early Adulthood (JAMA 1999)Document7 pages(PERSONALIDADE) Childhood Maltreatment Increases Risk For Personality Disorders During Early Adulthood (JAMA 1999)dilsohNo ratings yet
- Construct Validity of TPAADocument11 pagesConstruct Validity of TPAAponchossNo ratings yet
- Lister, 2015Document7 pagesLister, 2015Bianca HlepcoNo ratings yet
- RESUMEN ANALÍTICO ESPECIALIZADO (RAE) PsicopatologíaDocument7 pagesRESUMEN ANALÍTICO ESPECIALIZADO (RAE) PsicopatologíaCamila GuevaraNo ratings yet
- BulliedDocument13 pagesBulliedBarry BurijonNo ratings yet
- Fruzzetti 2005 OptionalDocument24 pagesFruzzetti 2005 OptionalMacovei Anca0% (1)
- Dating Violence Perpetration and Victimization Among U.S. Adolescents: Prevalence, Patterns, and Associations With Health Complaints and Substance UseDocument8 pagesDating Violence Perpetration and Victimization Among U.S. Adolescents: Prevalence, Patterns, and Associations With Health Complaints and Substance UseAlba EneaNo ratings yet
- Lee, Z,2003 Validez APSDDocument16 pagesLee, Z,2003 Validez APSDSonia FernandezNo ratings yet
- Early Risk and Protective Factors and Young Adult Outcomes in A Longitudinal Sample ofDocument22 pagesEarly Risk and Protective Factors and Young Adult Outcomes in A Longitudinal Sample ofNhon NhonNo ratings yet
- Fonseca-Pedrero, Et Al., 2011Document15 pagesFonseca-Pedrero, Et Al., 2011Diana StrambeiNo ratings yet
- Adolescent Personality Disorders Associated With Violence and Criminal Behavior During Adolescence and Early AdulthoodDocument7 pagesAdolescent Personality Disorders Associated With Violence and Criminal Behavior During Adolescence and Early AdulthoodIoana Duminicel100% (1)
- Child Maltreatment and Mental Health Problems in Adulthood Birth Cohort StudyDocument6 pagesChild Maltreatment and Mental Health Problems in Adulthood Birth Cohort Studyfotosiphone 8No ratings yet
- Psychopathics Traits in Adolescent OffendersDocument25 pagesPsychopathics Traits in Adolescent OffendersТеодора ДелићNo ratings yet
- Violencia en La Pareja1 PDFDocument13 pagesViolencia en La Pareja1 PDFNata ParraNo ratings yet
- Childhood Adversity and TLPDocument15 pagesChildhood Adversity and TLPPaula Ardila100% (1)
- Gri Zenko 1994Document11 pagesGri Zenko 1994Alex BoncuNo ratings yet
- Annotated Bibliography On Childhood Risk Factors To Criminal BehaviorDocument8 pagesAnnotated Bibliography On Childhood Risk Factors To Criminal Behaviorapi-667528548No ratings yet
- Edwards Et Al, 2021Document18 pagesEdwards Et Al, 2021fq8h6d87t4No ratings yet
- NIH Public Access: Author ManuscriptDocument35 pagesNIH Public Access: Author Manuscriptalfath akbarNo ratings yet
- (2013) - ExnerDocument10 pages(2013) - Exnerbeatriz.l.oliveira.2300No ratings yet
- Personality Disorders in AdolescenceDocument2 pagesPersonality Disorders in AdolescenceMale BajoNo ratings yet
- Associations Between Childhood Trauma, Bullying and Psychotic Symptoms Among A School-Based Adolescent SampleDocument6 pagesAssociations Between Childhood Trauma, Bullying and Psychotic Symptoms Among A School-Based Adolescent SampleChRist LumingkewasNo ratings yet
- The Childhood Trauma Questionnaire in ADocument15 pagesThe Childhood Trauma Questionnaire in ATuấn KhangNo ratings yet
- T K9 Ogxr LGUDocument7 pagesT K9 Ogxr LGUs.ullah janNo ratings yet
- Early Childhood Predictors of Boys' Antisocial and Violent Behavior in Early AdulthoodDocument15 pagesEarly Childhood Predictors of Boys' Antisocial and Violent Behavior in Early AdulthoodVictoria ZorzopulosNo ratings yet
- Childhood Adversity and Associated Psychosocial Function inDocument19 pagesChildhood Adversity and Associated Psychosocial Function inAraceli del PilarNo ratings yet
- Child and Adolescent Maltreatment Patterns and Risk of Eating Disorder Behaviors Developing in Young AdulthoodDocument9 pagesChild and Adolescent Maltreatment Patterns and Risk of Eating Disorder Behaviors Developing in Young AdulthoodVivian BandeiraNo ratings yet
- Child Abuse & Neglect: SciencedirectDocument19 pagesChild Abuse & Neglect: Sciencedirectana raquelNo ratings yet
- Childhood Adversity and Personality Disorders Results From A Nationallyrepresentative Population-Based Study - Afifi 2016 PDFDocument9 pagesChildhood Adversity and Personality Disorders Results From A Nationallyrepresentative Population-Based Study - Afifi 2016 PDFRodrigo Romo MuñozNo ratings yet
- A Risk Calculator For Bipolar Spectrum DisorderDocument2 pagesA Risk Calculator For Bipolar Spectrum DisorderDavidNo ratings yet
- NIH Public Access: Reciprocal-Effects of Parenting and Borderline Personality Disorder Symptoms in Adolescent GirlsDocument35 pagesNIH Public Access: Reciprocal-Effects of Parenting and Borderline Personality Disorder Symptoms in Adolescent Girlsalfath akbarNo ratings yet
- Child Personality Facets and Overreactive Parenting As PredictorsDocument15 pagesChild Personality Facets and Overreactive Parenting As Predictorsmary grace bialenNo ratings yet
- 1 s2.0 S0165178123000124 MainDocument11 pages1 s2.0 S0165178123000124 MainDwi HandayaniNo ratings yet
- 1 Sem 2 ModerationDocument18 pages1 Sem 2 ModerationalbertoNo ratings yet
- Vonderlin, 2018Document10 pagesVonderlin, 2018Zeynep ÖzmeydanNo ratings yet
- Jamapediatrics Moreno 2023 Ed 220035 1673637425.56866Document2 pagesJamapediatrics Moreno 2023 Ed 220035 1673637425.56866Lili CarrizalesNo ratings yet
- Callous-Unemotional Traits and Their Implication For Understanding and Treating Aggressive and Violent YouthsDocument20 pagesCallous-Unemotional Traits and Their Implication For Understanding and Treating Aggressive and Violent YouthsMaría Teresa Carrasco OjedaNo ratings yet
- Running Head: MENTAL DISORDERS 1Document12 pagesRunning Head: MENTAL DISORDERS 1api-532509198No ratings yet
- The Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To ChildDocument12 pagesThe Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To Child方科惠No ratings yet
- Talking About Sexuality With YouthDocument9 pagesTalking About Sexuality With YouthMariana AzevedoNo ratings yet
- Peer Selection and Socialization Effects On Adolescent Intercourse Without A Condom and Attitudes About The Costs of SexDocument14 pagesPeer Selection and Socialization Effects On Adolescent Intercourse Without A Condom and Attitudes About The Costs of SexTwradioNo ratings yet
- Kugler 2018Document8 pagesKugler 2018Andra IvanNo ratings yet
- Reactive Attachment Disorder Following Early Maltreatment: Systematic Evidence Beyond The InstitutionDocument11 pagesReactive Attachment Disorder Following Early Maltreatment: Systematic Evidence Beyond The Institution874328No ratings yet
- Prevalence of Mental Disorders - Children and AdolescentsDocument17 pagesPrevalence of Mental Disorders - Children and Adolescentsisabellabatista.psiNo ratings yet
- Children of Mothers With BPDDocument16 pagesChildren of Mothers With BPDapi-252946468100% (1)
- Nihms-July 22 - Early Timing and Determinants of The Sexual Orientation DisparityDocument22 pagesNihms-July 22 - Early Timing and Determinants of The Sexual Orientation DisparityArdaNo ratings yet
- Nihms 923786Document12 pagesNihms 923786FARHAT HAJERNo ratings yet
- 1-S2.0-S1053810016300629-Main Intimate Partner ViolenceDocument10 pages1-S2.0-S1053810016300629-Main Intimate Partner ViolenceVissente TapiaNo ratings yet
- The Role of Childhood Traumatization in The Development of Borderline Personality Disorder in HungaryDocument14 pagesThe Role of Childhood Traumatization in The Development of Borderline Personality Disorder in HungaryrahafNo ratings yet
- Predictive Factors For Juvenile Delinquency: The Role of Family Structure, Parental Monitoring and Delinquent PeersDocument9 pagesPredictive Factors For Juvenile Delinquency: The Role of Family Structure, Parental Monitoring and Delinquent PeersYogi setiawanNo ratings yet
- Rates of Nonsuicidal Self-Injury in YouthDocument9 pagesRates of Nonsuicidal Self-Injury in YouthWilson Javier Dominguez PerezNo ratings yet
- Gender Identity Disorder in Children and AdolescentsDocument27 pagesGender Identity Disorder in Children and AdolescentsGender Spectrum100% (3)
- From Emotional Abuse in Childhood To Psy PDFDocument24 pagesFrom Emotional Abuse in Childhood To Psy PDFNicoleta VasiliuNo ratings yet
- When Nowhere Is Safe: Interpersonal Trauma and Attachment Adversity As Antecedents of Posttraumatic Stress Disorder and Developmental Trauma DisorderDocument12 pagesWhen Nowhere Is Safe: Interpersonal Trauma and Attachment Adversity As Antecedents of Posttraumatic Stress Disorder and Developmental Trauma DisorderNerea F GNo ratings yet
- Foster Care IrrDocument7 pagesFoster Care Irrapi-530384945100% (1)
- Collishaw Et Al. (2007)Document49 pagesCollishaw Et Al. (2007)voooNo ratings yet
- Washignton ReportDocument8 pagesWashignton ReportSaim AliNo ratings yet
- Nurs 401 Case Study 5Document4 pagesNurs 401 Case Study 5Aliza SaddalNo ratings yet
- Block 4 Renal Lecture 1 MCQDocument5 pagesBlock 4 Renal Lecture 1 MCQMahmoud ElshrkawyNo ratings yet
- HEPAB Vax DSDocument3 pagesHEPAB Vax DSSheena Marie M. TarleNo ratings yet
- SepticemiaDocument1 pageSepticemiaomarwalidalhussaini2005No ratings yet
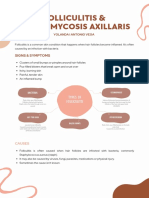
- Folliculitis and TrichomycosisDocument4 pagesFolliculitis and TrichomycosisYolisNo ratings yet
- C6.1clasificare LimfoameDocument10 pagesC6.1clasificare LimfoameRădulescu AndreeaNo ratings yet
- Typhoid PresentationDocument40 pagesTyphoid PresentationmakioedesemiNo ratings yet
- Atualização NeuromuscularDocument5 pagesAtualização NeuromuscularRodrigo VanzelliNo ratings yet
- Amir + Lev-Wiesel - 2007 - Dissociation As Depicted in Traumatic DrawingsDocument10 pagesAmir + Lev-Wiesel - 2007 - Dissociation As Depicted in Traumatic DrawingsAlejandra IsabelNo ratings yet
- DS SalbutamolDocument1 pageDS SalbutamolLarr SumalpongNo ratings yet
- ATPL08HumanPerformanceNPA29 2Document100 pagesATPL08HumanPerformanceNPA29 2André Luiz BragaNo ratings yet
- GDMTDocument2 pagesGDMTapi-690342013No ratings yet
- NN 2Document10 pagesNN 2Thành ĐinhNo ratings yet
- Ophthalmology Set 1Document6 pagesOphthalmology Set 1ajay khadeNo ratings yet
- Liver Cirrhosis 2020Document27 pagesLiver Cirrhosis 2020Gabriela SalasNo ratings yet
- EAU Guidelines 2023 PDFDocument2,012 pagesEAU Guidelines 2023 PDFEncep SetiawanNo ratings yet
- A Case Study On MalariaDocument10 pagesA Case Study On MalariaAnant KumarNo ratings yet
- Practical Aspects of IVUS-Guided Percutaneous Coronary InterventionDocument7 pagesPractical Aspects of IVUS-Guided Percutaneous Coronary InterventionRajesh JayakumarNo ratings yet
- 311 Topotecan Monotherapy 5 DayDocument4 pages311 Topotecan Monotherapy 5 DayRuxandra BănicăNo ratings yet
- Progress Report National Cancer Registry in IndonesiaDocument47 pagesProgress Report National Cancer Registry in IndonesiaIndonesian Journal of Cancer100% (1)
- Airport Security ForcesDocument2 pagesAirport Security ForcesJamsher BalochNo ratings yet
- LeptospirosisDocument26 pagesLeptospirosisDinesh KumarNo ratings yet
- DebateDocument12 pagesDebate•Kai yiii•No ratings yet
- 1 - VSD (Part 2) - Hatem HosnyDocument28 pages1 - VSD (Part 2) - Hatem Hosnyrami ibrahiemNo ratings yet
- Glimmers of Hope For Targeting Oncogenic KRAS-G12D: Cancer Gene TherapyDocument3 pagesGlimmers of Hope For Targeting Oncogenic KRAS-G12D: Cancer Gene Therapychato law officeNo ratings yet