Download as pdf or txt
You might also like
- BMAT Biology Revision NotesDocument9 pagesBMAT Biology Revision Notesmissymar123100% (5)
- Lung AnatomyDocument19 pagesLung AnatomyScott Yee100% (2)
- Your Breath On Yoga: The Anatomy & Physiology of Breathing for Teachers and Students of YogaFrom EverandYour Breath On Yoga: The Anatomy & Physiology of Breathing for Teachers and Students of YogaNo ratings yet
- F5 Exam P2 QuestionsDocument5 pagesF5 Exam P2 QuestionsTrevor G. Samaroo100% (3)
- Opgave 1: Side 1 Af 11Document11 pagesOpgave 1: Side 1 Af 11shamoNo ratings yet
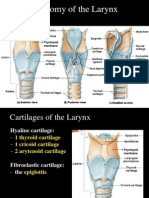
- Anatomy of The Larynx: Thyrohyoid MembraneDocument35 pagesAnatomy of The Larynx: Thyrohyoid MembraneVarsha Shende KhobragadeNo ratings yet
- Diaphragm: Mr. Abdur Rehman BS-cardiology Kmu-IpmsDocument19 pagesDiaphragm: Mr. Abdur Rehman BS-cardiology Kmu-IpmsAbdurrehman SafiNo ratings yet
- Structure of The Lung Biomechanics of BreathingDocument55 pagesStructure of The Lung Biomechanics of BreathingMohd Yunus KhiljiNo ratings yet
- Anatomy of Respiratory System - KMUDocument23 pagesAnatomy of Respiratory System - KMUSalman KhanNo ratings yet
- Anatomy and Physiology of RespirationDocument44 pagesAnatomy and Physiology of Respirationleenadevi90No ratings yet
- ThoraxDocument29 pagesThoraxapi-249972919No ratings yet
- Assessment of Lungs and ThoraxDocument58 pagesAssessment of Lungs and ThoraxShahmeerNo ratings yet
- Respiratory System (2015 - 06 - 09 22 - 21 - 55 Utc)Document57 pagesRespiratory System (2015 - 06 - 09 22 - 21 - 55 Utc)DiazNo ratings yet
- 224392278 BMAT Biology Revision Notesรรร PDFDocument9 pages224392278 BMAT Biology Revision Notesรรร PDFB. ChillNo ratings yet
- Anatomy RespiratoryDocument68 pagesAnatomy RespiratorydofezdsNo ratings yet
- Anatomy of The Heart: Epicardium Myocardium EndocardiumDocument8 pagesAnatomy of The Heart: Epicardium Myocardium EndocardiumTrishna ShahNo ratings yet
- Respiratory SystemDocument56 pagesRespiratory SystemSalma NawazNo ratings yet
- Gr. 9 Science LM (AG)Document33 pagesGr. 9 Science LM (AG)Aizalonica GalangNo ratings yet
- Vsp-Ug-5 (RS)Document59 pagesVsp-Ug-5 (RS)6qhx62pr42No ratings yet
- Respiratory SystemDocument4 pagesRespiratory Systemtarunesh1No ratings yet
- The Respiratory System of Human Body FactsDocument12 pagesThe Respiratory System of Human Body FactsjulianneboloronNo ratings yet
- Bio Notes Respiration in AnimalsDocument3 pagesBio Notes Respiration in AnimalssamanthahuangsamanthaNo ratings yet
- The Respiratory SystemDocument3 pagesThe Respiratory Systempaulo_camuaNo ratings yet
- Bio 103 Section 3 Circulatory, Respiratory & Excretory SystemDocument33 pagesBio 103 Section 3 Circulatory, Respiratory & Excretory SystemMD Reyadus SalihenNo ratings yet
- A&P - PHYSIOLOGY OF RESPIRATION - InspirationDocument32 pagesA&P - PHYSIOLOGY OF RESPIRATION - InspirationYAMINIPRIYAN100% (1)
- L5 Surface Anatomy & DiaphragmDocument45 pagesL5 Surface Anatomy & DiaphragmatefmoussaNo ratings yet
- 14788physiology Respiration Lecture 1 - RRS BlockDocument11 pages14788physiology Respiration Lecture 1 - RRS BlockHsay AyitehgNo ratings yet
- The Pathway: The Human Respiratory SystemDocument25 pagesThe Pathway: The Human Respiratory SystemKenneth Decker PrietoNo ratings yet
- Var 29 - 30Document4 pagesVar 29 - 30Honey BabaNo ratings yet
- Anatomy of LungsDocument20 pagesAnatomy of LungsAhmad NizamNo ratings yet
- Physiology of Respiration - Mechanism of Respiration, GaseousDocument39 pagesPhysiology of Respiration - Mechanism of Respiration, GaseousRakesh KumarNo ratings yet
- OxygenationDocument46 pagesOxygenationMuhammad Farooq SaeedNo ratings yet
- Ch.19 Thorax and LungsDocument14 pagesCh.19 Thorax and LungsJose R. MendozaNo ratings yet
- Autumn 2006 Q4 Write Short Notes On Three of The FollowingDocument4 pagesAutumn 2006 Q4 Write Short Notes On Three of The Following3cinr3bNo ratings yet
- 1) Anatomy & Physiology - 202243.15374-CCRN-1505-01 - MANAGEMENT OF CCHC - RESPIRATORYDocument12 pages1) Anatomy & Physiology - 202243.15374-CCRN-1505-01 - MANAGEMENT OF CCHC - RESPIRATORYafshin nikraveshNo ratings yet
- Thoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دDocument18 pagesThoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دMuhammad UsmanNo ratings yet
- Science ReviewerDocument19 pagesScience ReviewerfluyuuyyyNo ratings yet
- Respiratory AssessmentDocument25 pagesRespiratory AssessmentLIBIN PALLUPPETTAYIL JOSE100% (2)
- Anatomy 4 RespDocument46 pagesAnatomy 4 RespibrooavcNo ratings yet
- Respiratory system for Grade XIIDocument14 pagesRespiratory system for Grade XIIssah4155No ratings yet
- 1-Mechanism and Regulation of Respiration ModifiedDocument10 pages1-Mechanism and Regulation of Respiration Modifiedخالد القرشيNo ratings yet
- Respiratory System: Respiration (Oxidation of Food in Cells Cellular Respiration Energy Is Produced Along With WaterDocument15 pagesRespiratory System: Respiration (Oxidation of Food in Cells Cellular Respiration Energy Is Produced Along With WaterShuvanjan DahalNo ratings yet
- Chapter 1 Scs f3Document15 pagesChapter 1 Scs f3putridequenoNo ratings yet
- 1 Mechanism of RespirationDocument22 pages1 Mechanism of RespirationAhmed AliNo ratings yet
- Anatomy Personal NoteDocument7 pagesAnatomy Personal NoteShereen Al-ObinayNo ratings yet
- General Anatomy 4 Thoracic Cavity: Dr. Wesam BaderDocument46 pagesGeneral Anatomy 4 Thoracic Cavity: Dr. Wesam BaderAhmadNo ratings yet
- Respiratory SystemDocument33 pagesRespiratory SystemMusadiq Khan DurraniNo ratings yet
- Science: Quarter 1 - Module 1Document10 pagesScience: Quarter 1 - Module 1RUTH PIANGNo ratings yet
- Respiratory System: Nose and NostrilsDocument8 pagesRespiratory System: Nose and NostrilsKabang MoaNo ratings yet
- Unit 5.2 Pleura and LungsDocument27 pagesUnit 5.2 Pleura and LungsBidhan RegmiNo ratings yet
- Respiratory NotesDocument6 pagesRespiratory NotesBethany CrawfordNo ratings yet
- Physiology of RespirationDocument2 pagesPhysiology of RespirationIOSRjournalNo ratings yet
- POINTERS-SCIENCE Grade 9 Quarter 1Document7 pagesPOINTERS-SCIENCE Grade 9 Quarter 1Lunyl DelloNo ratings yet
- INGLES I TP 2 - Ud 2Document10 pagesINGLES I TP 2 - Ud 2DaniNo ratings yet
- Unit 6 Part 2 Thoracic CavityDocument56 pagesUnit 6 Part 2 Thoracic CavitySiraj ShiferawNo ratings yet
- Respiration, Types of Respiration and Anatomy of Human Respiratory SystemDocument8 pagesRespiration, Types of Respiration and Anatomy of Human Respiratory Systemegfr3yfgNo ratings yet
- Notes On The Thorax: Anatomy RHS 241Document71 pagesNotes On The Thorax: Anatomy RHS 241William JonathanNo ratings yet
- Respiratory System - AnatomyDocument28 pagesRespiratory System - AnatomyDinesh KumarNo ratings yet
- Respiratory gymnastics (Translated): Purification - Health - Strength - EnergyFrom EverandRespiratory gymnastics (Translated): Purification - Health - Strength - EnergyNo ratings yet
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksFrom EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksNo ratings yet
- Human Body Book | Introduction to the Respiratory System | Children's Anatomy & Physiology EditionFrom EverandHuman Body Book | Introduction to the Respiratory System | Children's Anatomy & Physiology EditionNo ratings yet
- Join The Club: C207 - Database Systems 2012Document237 pagesJoin The Club: C207 - Database Systems 2012hamzahNo ratings yet
- Egyptian PPP Law 67 For 2010 EnglishDocument17 pagesEgyptian PPP Law 67 For 2010 EnglishReham El AbnoudyNo ratings yet
- Recounttext 160409104911Document9 pagesRecounttext 160409104911Anif Ough GtuwNo ratings yet
- Sro 565-2006Document44 pagesSro 565-2006Abdullah Jathol100% (1)
- JD - Part Time Online ESL Teacher - Daylight PDFDocument2 pagesJD - Part Time Online ESL Teacher - Daylight PDFCIO White PapersNo ratings yet
- Physica A: Bilal Saoud, Abdelouahab MoussaouiDocument9 pagesPhysica A: Bilal Saoud, Abdelouahab MoussaouiHaroonRashidNo ratings yet
- 5 Leadership LessonsDocument2 pages5 Leadership LessonsnyniccNo ratings yet
- Runner of Francis Turbine:) Cot Cot (Document5 pagesRunner of Francis Turbine:) Cot Cot (Arun Kumar SinghNo ratings yet
- GSPI-QA of Teaching Staff-Draft3Document43 pagesGSPI-QA of Teaching Staff-Draft3Tempus WebsitesNo ratings yet
- Maxima and MinimaDocument12 pagesMaxima and MinimaDennis Dale60% (5)
- Cincinnati Retirement System Update: March 28, 2022Document24 pagesCincinnati Retirement System Update: March 28, 2022WVXU NewsNo ratings yet
- Revised 04/01/2021Document33 pagesRevised 04/01/2021Kim PowellNo ratings yet
- Chapter 6 Project ManagementDocument54 pagesChapter 6 Project ManagementSHAWN TAKAONANo ratings yet
- Persuasive Writing Assessment RubricDocument2 pagesPersuasive Writing Assessment Rubricapi-523656984No ratings yet
- Smart Contracts: Functioning and Legal Enforceability in IndiaDocument14 pagesSmart Contracts: Functioning and Legal Enforceability in IndiaPrasanth Raju100% (1)
- Plain Bearings Made From Engineering PlasticsDocument44 pagesPlain Bearings Made From Engineering PlasticsJani LahdelmaNo ratings yet
- Experiment 1Document9 pagesExperiment 1Mehar HamzaNo ratings yet
- Manual de Instalación - Tableros Centro de Carga - Marca GEDocument4 pagesManual de Instalación - Tableros Centro de Carga - Marca GEmariana0% (1)
- (IMechE Conference Transactions) PEP (Professional Engineering Publishers) - Power Station Maintenance - Professional Engineering Publishing (2000) PDFDocument266 pages(IMechE Conference Transactions) PEP (Professional Engineering Publishers) - Power Station Maintenance - Professional Engineering Publishing (2000) PDFAlexanderNo ratings yet
- Corporations: Organization and Capital Stock Transaction: Corporation Second GradeDocument113 pagesCorporations: Organization and Capital Stock Transaction: Corporation Second GradePeter WagdyNo ratings yet
- Note On Geneva ConventionDocument12 pagesNote On Geneva ConventionRajesh JosephNo ratings yet
- An Innovative Method To Increase The Resolution of Optical EncodersDocument6 pagesAn Innovative Method To Increase The Resolution of Optical EncodersFuadMuzaki09No ratings yet
- A G Gardiner EssaysDocument50 pagesA G Gardiner Essaysngisjqaeg100% (2)
- Defense Support of Civil Authorities (Dsca) : This Briefing IsDocument15 pagesDefense Support of Civil Authorities (Dsca) : This Briefing IsChris WhiteheadNo ratings yet
- Marcopolo Is A Leading Brazilian Bus Body ManufacturerDocument4 pagesMarcopolo Is A Leading Brazilian Bus Body ManufacturerCH NAIRNo ratings yet
- Geothermal Well Operation and Maintenance: Sverrir ThorhallssonDocument23 pagesGeothermal Well Operation and Maintenance: Sverrir ThorhallssonLaras PutiNo ratings yet
- Chapter 18: Concurrency Control: Database System Concepts, 7 EdDocument91 pagesChapter 18: Concurrency Control: Database System Concepts, 7 Edzhazhiy newNo ratings yet
- De Claro SinglesDocument96 pagesDe Claro Singlesapi-3701495No ratings yet