Download as pdf or txt
You might also like
- 46th National Safety Quiz - 17Document6 pages46th National Safety Quiz - 17NiranjanAryan100% (7)
- Yjmt 30 1992090Document13 pagesYjmt 30 1992090Luis Sebastian Arango OspinaNo ratings yet
- The Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewDocument7 pagesThe Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewIJAR JOURNALNo ratings yet
- Kuhn2013 PDFDocument9 pagesKuhn2013 PDFNati GallardoNo ratings yet
- 2023 JOT Radiological and Long Term Functional Outcomes of Displaced Distal Clavicle FracturesDocument7 pages2023 JOT Radiological and Long Term Functional Outcomes of Displaced Distal Clavicle FracturesjcmarecauxlNo ratings yet
- Heart & Lung: Care of Critically Ill AdultsDocument13 pagesHeart & Lung: Care of Critically Ill AdultsRabiyatul AwaliyahNo ratings yet
- Outcomes After Acute Versus Delayed Total Elbow ArDocument8 pagesOutcomes After Acute Versus Delayed Total Elbow ArLuis Guillermo Buitrago BuitragoNo ratings yet
- Two Decades of Hand TransplantationDocument10 pagesTwo Decades of Hand TransplantationTamsin Athalie NicholsonNo ratings yet
- Dy 2012Document5 pagesDy 2012Aldrovando JrNo ratings yet
- 1 s2.0 S2049080122006756 MainDocument5 pages1 s2.0 S2049080122006756 MainReskyAyuWulandariNo ratings yet
- Gadjradj2017 - Criterio Cirurgia ColunaDocument23 pagesGadjradj2017 - Criterio Cirurgia ColunaDr Aléssio NovaisNo ratings yet
- Clinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialDocument8 pagesClinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialfaundraNo ratings yet
- Hand Transplantation Current Concepts and ManagemeDocument10 pagesHand Transplantation Current Concepts and Managemeeliseoo8ortegaNo ratings yet
- 2010 Mars Group Descriptive Epidemiology of The Multicenter ACL Revision Study (MARS) CohortDocument8 pages2010 Mars Group Descriptive Epidemiology of The Multicenter ACL Revision Study (MARS) CohortArmin ParavlićNo ratings yet
- Parker 2020Document6 pagesParker 2020QuiroprácticaParaTodosNo ratings yet
- Patients Benefit While Surgeons Suffer: An Impending EpidemicDocument8 pagesPatients Benefit While Surgeons Suffer: An Impending EpidemicMiguel Fernando ALban VasquezNo ratings yet
- Jurnal Fraktur PDFDocument9 pagesJurnal Fraktur PDFdwi vaniNo ratings yet
- Functional Outcome of Total Hip Arthroplasty With Dual Mobility Cups in Hip Arthritis-A Prospective Cohort StudyDocument7 pagesFunctional Outcome of Total Hip Arthroplasty With Dual Mobility Cups in Hip Arthritis-A Prospective Cohort StudyIJAR JOURNALNo ratings yet
- Barriers To Ultrasound GuidanceDocument9 pagesBarriers To Ultrasound GuidanceHarm ScholtenNo ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- Jurnal Tendon 1Document10 pagesJurnal Tendon 1hendrabecaxNo ratings yet
- Clinical ResearcheffectsDocument7 pagesClinical ResearcheffectsJackielyn C. AportaderaNo ratings yet
- Time and Travel Burden Associated With Hexapod Assisted Correction of Lower Extremity DeformityDocument6 pagesTime and Travel Burden Associated With Hexapod Assisted Correction of Lower Extremity DeformityAthenaeum Scientific PublishersNo ratings yet
- Int Orthop 2022 Jun - 46 (6) 1253-1279Document27 pagesInt Orthop 2022 Jun - 46 (6) 1253-1279MarianoNo ratings yet
- No 4Document8 pagesNo 4Dinda Amalia Amanah BarokahNo ratings yet
- Hemipelvectomia INCADocument7 pagesHemipelvectomia INCAdrjccanciolopesNo ratings yet
- Goh 2019Document5 pagesGoh 2019Maya RafidaNo ratings yet
- Midshaft Clavicle Fractures: Surgery Provides Better Results As Compared With Nonoperative TreatmentDocument10 pagesMidshaft Clavicle Fractures: Surgery Provides Better Results As Compared With Nonoperative TreatmentS3V4_9154No ratings yet
- 2022 - Association Between Compliance With Enhanced Recovery After Surgery (ERAS) ProtocolsDocument13 pages2022 - Association Between Compliance With Enhanced Recovery After Surgery (ERAS) ProtocolsClarissa Simon FactumNo ratings yet
- Four Corner Fusion Vs PRCDocument6 pagesFour Corner Fusion Vs PRC79rdhsygngNo ratings yet
- Sys Rev TT of Intermittent ClaudicationDocument20 pagesSys Rev TT of Intermittent ClaudicationMaria PopNo ratings yet
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsDocument9 pagesReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- Characterization of Device-Related Interruptions in Minimally Invasive Surgery: Need For Intraoperative Data and Effective Mitigation StrategiesDocument7 pagesCharacterization of Device-Related Interruptions in Minimally Invasive Surgery: Need For Intraoperative Data and Effective Mitigation Strategiestabsf41No ratings yet
- 2017 Article 528Document12 pages2017 Article 528Marios GhobrialNo ratings yet
- Dfa 7 30079 PDFDocument8 pagesDfa 7 30079 PDFfakhrul arifinNo ratings yet
- Comparative Health Technology Assessment of Robotic-AssistedDocument9 pagesComparative Health Technology Assessment of Robotic-AssistedDanica SavićNo ratings yet
- Arthroscopic Irrigation and Debridement Is Associated With Favourable Short-Term Outcomes vs. Open Management - An ACS-NSQIP Database AnalysisDocument7 pagesArthroscopic Irrigation and Debridement Is Associated With Favourable Short-Term Outcomes vs. Open Management - An ACS-NSQIP Database AnalysisLaura AreizaNo ratings yet
- Clinical Outcomes in Patients With Scaphoid Non UnDocument5 pagesClinical Outcomes in Patients With Scaphoid Non UndominguezdoradopatriciaNo ratings yet
- Minimally Invasive Surgery Techniques in Pelvic Exenteration - A Systematic and Meta-Analysis ReviewDocument9 pagesMinimally Invasive Surgery Techniques in Pelvic Exenteration - A Systematic and Meta-Analysis ReviewWarren SeowNo ratings yet
- Complication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011Document6 pagesComplication and Revision Rates Following Total Elbow Arthroplasty JHS Am 2011JT DanielsNo ratings yet
- A Survey of Hip Society Surgeons Concerning The Direct Anterior Approach Total Hip ArthroplastyDocument5 pagesA Survey of Hip Society Surgeons Concerning The Direct Anterior Approach Total Hip ArthroplastybranislavNo ratings yet
- Preoperative Embolization in Patients With Metastatic Spinal Cord Compression: Mandatory or Optional?Document8 pagesPreoperative Embolization in Patients With Metastatic Spinal Cord Compression: Mandatory or Optional?karrameliaNo ratings yet
- Protocol ErasDocument13 pagesProtocol ErasanyelomdpNo ratings yet
- Anesthetic Management of Geriatric Patients: Review ArticleDocument22 pagesAnesthetic Management of Geriatric Patients: Review Articleagita kartika sariNo ratings yet
- Bessire 2014Document7 pagesBessire 2014andrei3cucuNo ratings yet
- Assessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryDocument8 pagesAssessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryIJAR JOURNALNo ratings yet
- Correlation Between Nursing Practices Regarding Blood Transfusion and Its Adverse Reactions, 2020Document6 pagesCorrelation Between Nursing Practices Regarding Blood Transfusion and Its Adverse Reactions, 2020fitriNo ratings yet
- STITCH Protocol 2011Document9 pagesSTITCH Protocol 2011Crhistian GarcíaNo ratings yet
- Simplified Frailty Index As A Predictor of Adverse Outcomes in Total Hip and Knee ArthroplastyDocument6 pagesSimplified Frailty Index As A Predictor of Adverse Outcomes in Total Hip and Knee ArthroplastyJohn SmithNo ratings yet
- Machine Learning Based Models To Support Decision Maki - 2021 - International JoDocument7 pagesMachine Learning Based Models To Support Decision Maki - 2021 - International JobasubuetNo ratings yet
- Follow-Up Observation of Patients With Obstructive Sleep Apnea Treated by Maxillomandibular AdvancementDocument8 pagesFollow-Up Observation of Patients With Obstructive Sleep Apnea Treated by Maxillomandibular AdvancementNaveenNo ratings yet
- The Journal of ArthroplastyDocument8 pagesThe Journal of Arthroplasty阿欧有怪兽No ratings yet
- Ekhtiari 2017Document9 pagesEkhtiari 2017QuiroprácticaParaTodosNo ratings yet
- Surgical Risk Preoperative Assessment System (SURPAS)Document7 pagesSurgical Risk Preoperative Assessment System (SURPAS)Guilherme AnacletoNo ratings yet
- PDR Pinning Systematic ReviewDocument8 pagesPDR Pinning Systematic ReviewCleff FlowersNo ratings yet
- Cirugía de HAV y Calidad de VidaDocument8 pagesCirugía de HAV y Calidad de VidaAlejandro Fernandez GibelloNo ratings yet
- Belykh, E., Krutko, A. V., Baykov, E. S., Giers, M. B., Preul, M. C., & Byvaltsev, V. A. (2017). Preoperative estimation of disc herniation recurrence after microdiscectomy predictive value of a multivariate model basedDocument11 pagesBelykh, E., Krutko, A. V., Baykov, E. S., Giers, M. B., Preul, M. C., & Byvaltsev, V. A. (2017). Preoperative estimation of disc herniation recurrence after microdiscectomy predictive value of a multivariate model basedRobert AndreiNo ratings yet
- Kiper 2018Document13 pagesKiper 2018annisayaNo ratings yet
- Early Vascular Surgery Response To The COVID-19 Pandemic: Results of A Nationwide SurveyDocument9 pagesEarly Vascular Surgery Response To The COVID-19 Pandemic: Results of A Nationwide SurveyAji Prasetyo UtomoNo ratings yet
- Damage Control Resuscitation: Identification and Treatment of Life-Threatening HemorrhageFrom EverandDamage Control Resuscitation: Identification and Treatment of Life-Threatening HemorrhagePhilip C. SpinellaNo ratings yet
- Lambert 2018Document7 pagesLambert 2018Tamsin Athalie NicholsonNo ratings yet
- Two Decades of Hand TransplantationDocument10 pagesTwo Decades of Hand TransplantationTamsin Athalie NicholsonNo ratings yet
- NDFriendly WorkbookDocument81 pagesNDFriendly WorkbookTamsin Athalie Nicholson100% (2)
- Jama Biglino 2017 Am 170018Document3 pagesJama Biglino 2017 Am 170018Tamsin Athalie NicholsonNo ratings yet
- Lambert 2020Document10 pagesLambert 2020Tamsin Athalie NicholsonNo ratings yet
- Henry KrukenbergDocument12 pagesHenry KrukenbergTamsin Athalie NicholsonNo ratings yet
- Example Systermatic Review and Narrative SynthesisDocument11 pagesExample Systermatic Review and Narrative SynthesisTamsin Athalie NicholsonNo ratings yet
- The Art of Surgery: The Strange World of The Placebo ResponseDocument4 pagesThe Art of Surgery: The Strange World of The Placebo ResponseTamsin Athalie NicholsonNo ratings yet
- RMVS001 Rapidly Manufactured Ventilator Specification PDFDocument9 pagesRMVS001 Rapidly Manufactured Ventilator Specification PDFjalmeida88No ratings yet
- A Qualitative Study of CyberseDocument24 pagesA Qualitative Study of Cybersehannahade1No ratings yet
- Assessment Tool For Authentic Learning Performance: Ferment Fish and Other Marine Products (TLE - AFFP9-12FR-lllh-i-5)Document3 pagesAssessment Tool For Authentic Learning Performance: Ferment Fish and Other Marine Products (TLE - AFFP9-12FR-lllh-i-5)mary kennie griarNo ratings yet
- Domestic Violence Restraining Order Against Alicia ChampionDocument16 pagesDomestic Violence Restraining Order Against Alicia ChampionNationwide ReporterNo ratings yet
- Lesson 3 SELF-ASSESSES HEALTH RELATED PARTICIPATION AND ONE'S DIET FITNESSDocument20 pagesLesson 3 SELF-ASSESSES HEALTH RELATED PARTICIPATION AND ONE'S DIET FITNESSRio TomasNo ratings yet
- AI Report 2024 DavosDocument99 pagesAI Report 2024 DavosKarthikeyan GanesanNo ratings yet
- Molecular Ecology - 2023 - Velsko - High Conservation of The Dental Plaque Microbiome Across Populations With DifferingDocument20 pagesMolecular Ecology - 2023 - Velsko - High Conservation of The Dental Plaque Microbiome Across Populations With Differingloayza55No ratings yet
- HRT BenefitsDocument3 pagesHRT BenefitsJas SinNo ratings yet
- Traditional BSN Degree Plan 2022 2023 202220Document1 pageTraditional BSN Degree Plan 2022 2023 202220Edgar MartínezNo ratings yet
- CowspiracyDocument3 pagesCowspiracyNisah MacaronsingNo ratings yet
- Psyu 101 Course TipsDocument9 pagesPsyu 101 Course Tipsapi-546565206No ratings yet
- DayanaDocument27 pagesDayananenethgf95No ratings yet
- TFN - WagasDocument2 pagesTFN - WagasKen Kyle WagasNo ratings yet
- Bio SafetyDocument18 pagesBio SafetyMuhammad ShaikhNo ratings yet
- Prost Ho Don TicDocument175 pagesProst Ho Don Ticrxmskdkd33No ratings yet
- Menstrual Cups Report Studying The MarketDocument48 pagesMenstrual Cups Report Studying The MarketSheetal MishraNo ratings yet
- Accident Prevention Plan FINALDocument74 pagesAccident Prevention Plan FINALsakrakirfanNo ratings yet
- Empowerment and Advocacy PDFDocument9 pagesEmpowerment and Advocacy PDFLianne CasinoNo ratings yet
- Unit 8.2 - Planning Final (1-9-2019)Document23 pagesUnit 8.2 - Planning Final (1-9-2019)Josephine TorresNo ratings yet
- Muhammad+Iqbal+et+al +2023Document10 pagesMuhammad+Iqbal+et+al +2023alamzebNo ratings yet
- Approaches To Professional SupervisionDocument26 pagesApproaches To Professional SupervisionYvette Lopez CarpinteroNo ratings yet
- Nursing Care of The Community CHP 7Document20 pagesNursing Care of The Community CHP 7marissaNo ratings yet
- Life Assurance Application Form-EDocument8 pagesLife Assurance Application Form-Elisa marieNo ratings yet
- Propofol Infusion Syndrome PDFDocument3 pagesPropofol Infusion Syndrome PDFPGI AnaesthesiaNo ratings yet
- URIKAR - The Most Advanced & Powerful Percussion Massager With AI Chip For Daily Stress Relief and Workout RecoveryDocument2 pagesURIKAR - The Most Advanced & Powerful Percussion Massager With AI Chip For Daily Stress Relief and Workout RecoveryPR.comNo ratings yet
- The 5 Am Club Sharma en 36369Document7 pagesThe 5 Am Club Sharma en 36369smartagsarun80No ratings yet
- DextroseDocument1 pageDextroseAdrianne BazoNo ratings yet
- Full Test Bank For Mastering The World of Psychology 6Th Editionellen Green Wood Samuel E Wood Denise Boyd PDF Docx Full Chapter ChapterDocument36 pagesFull Test Bank For Mastering The World of Psychology 6Th Editionellen Green Wood Samuel E Wood Denise Boyd PDF Docx Full Chapter Chapterrhinovehicledkd1a7100% (12)
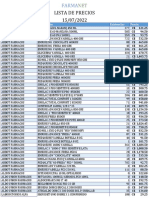
- Farmanet CatalogoDocument23 pagesFarmanet CatalogoYader ChamorroNo ratings yet