Download as pdf or txt
You might also like
- Beyond The CampfireDocument22 pagesBeyond The CampfireChristophe baudouxNo ratings yet
- Member List For Indonesia Mold & Die AssociationDocument14 pagesMember List For Indonesia Mold & Die AssociationDaniel Pandapotan MarpaungNo ratings yet
- Segregation of Duties Matrix SampleDocument3 pagesSegregation of Duties Matrix SampleNijith p.nNo ratings yet
- Amboss ECGDocument13 pagesAmboss ECGAllysahNo ratings yet
- Reten Modern Dressing 2023 PKDMTDocument51 pagesReten Modern Dressing 2023 PKDMTMasros TukiranNo ratings yet
- Recorrido Montacargas LaminaDocument1 pageRecorrido Montacargas LaminaPablo GandarillaNo ratings yet
- 3.reten Woundcare KKL March 2023Document2 pages3.reten Woundcare KKL March 2023Syah AizatNo ratings yet
- Straumann Dental System Map BoneLevelProstheticsDocument1 pageStraumann Dental System Map BoneLevelProstheticscarla1315No ratings yet
- Mindmap Meten 3Document1 pageMindmap Meten 3IpulCoolNo ratings yet
- 4 - RETEN WOUNDCARE KKL April 2023Document2 pages4 - RETEN WOUNDCARE KKL April 2023Syah AizatNo ratings yet
- Draft 2Document1 pageDraft 2K61 ĐOÀN HỒ GIA HUYNo ratings yet
- Poli PlaanDocument1 pagePoli Plaansuhana dhunganaNo ratings yet
- ContentDocument1 pageContentserena7205No ratings yet
- En OGC Catalogue MaxsealDocument32 pagesEn OGC Catalogue MaxsealHai Pham VanNo ratings yet
- Panduan Tugas Pip PDFDocument72 pagesPanduan Tugas Pip PDFMuhammad RienaldyNo ratings yet
- Panasonic RR-US360 - Operating Instructions (English)Document2 pagesPanasonic RR-US360 - Operating Instructions (English)mivamoura100% (2)
- DR.M Rafat Ka Tassure IlmDocument5 pagesDR.M Rafat Ka Tassure IlmMuhammad GhitreefNo ratings yet
- Smart Swadhan Plus - BrochureDocument10 pagesSmart Swadhan Plus - Brochureanil1216kumarNo ratings yet
- Riser DiagramDocument1 pageRiser Diagramomar esamNo ratings yet
- Projective Geometric Algebra: Norms Binary Operations Transformation GroupsDocument1 pageProjective Geometric Algebra: Norms Binary Operations Transformation GroupsKrutarth PatelNo ratings yet
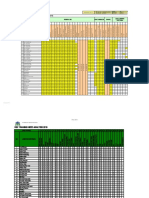
- Hse Traning Need Analisys 2018: Course CodeDocument7 pagesHse Traning Need Analisys 2018: Course Coderifki bahtiarNo ratings yet
- Business Model Canvas Poster-DikonversiDocument1 pageBusiness Model Canvas Poster-DikonversiHana NatashamuraNo ratings yet
- Screenshot 2024-01-03 at 09.58.50Document1 pageScreenshot 2024-01-03 at 09.58.50sagvantayebNo ratings yet
- Mind Map Sym&Parasym DrugsDocument2 pagesMind Map Sym&Parasym Drugsjitpinun.sNo ratings yet
- De - Mavenclad - Actrims 2024 Cladrina p481Document1 pageDe - Mavenclad - Actrims 2024 Cladrina p481magdecanedaNo ratings yet
- UntitledDocument48 pagesUntitledСергей КартавицкийNo ratings yet
- Angeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsDocument10 pagesAngeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsMiguel C. DolotNo ratings yet
- AmniSure ROM Test Instructions For Use (2019)Document1 pageAmniSure ROM Test Instructions For Use (2019)Hòa HồNo ratings yet
- Electric CAT375L-1JMDocument2 pagesElectric CAT375L-1JMTrần Tiến AnhNo ratings yet
- Unit 2 Reading Material-1Document85 pagesUnit 2 Reading Material-1Mister MarlegaNo ratings yet
- Notes AtherosclerosisDocument1 pageNotes AtherosclerosisElizabeth de GuzmanNo ratings yet
- Seepage BEDs On Site Layout Plan-M-DE-A-012Document1 pageSeepage BEDs On Site Layout Plan-M-DE-A-012nimodi lankaNo ratings yet
- Tehilim Im Piroush Tehilat ChmouelDocument282 pagesTehilim Im Piroush Tehilat ChmouelNathaniel SauraNo ratings yet
- Nog Energy Week 2023 May FloorplanDocument1 pageNog Energy Week 2023 May FloorplanojoladapoNo ratings yet
- Plano Electrico 777fDocument4 pagesPlano Electrico 777fTERONo ratings yet
- Esquema Coastal LineDocument2 pagesEsquema Coastal LineDaniel NiñoNo ratings yet
- Achievement Chart: Driving NciiDocument2 pagesAchievement Chart: Driving NciiRemelyn Bulahao LicyayoNo ratings yet
- Unit 5 - DirectionnDocument16 pagesUnit 5 - DirectionnAchmad SusantoNo ratings yet
- Dinas Kesehatan Dan: Kabupaten Kayong UtaraDocument1 pageDinas Kesehatan Dan: Kabupaten Kayong Utaraadie 999No ratings yet
- Ocular Manifestations of Systemic DiseaseDocument1 pageOcular Manifestations of Systemic DiseaseTanya HoNo ratings yet
- bản vẽ 2109 d01Document5 pagesbản vẽ 2109 d01thanh longNo ratings yet
- Chemistry Mock-TestDocument48 pagesChemistry Mock-TestsindhsanamNo ratings yet
- Mapa Campo RBDocument1 pageMapa Campo RBjavier florezNo ratings yet
- Ag Ug: 330 TH Ru GR Av El at El - +2 370 0Document1 pageAg Ug: 330 TH Ru GR Av El at El - +2 370 0John SmitNo ratings yet
- Redes Alcantarillado Pluvial Plancha: 1-Sa-P-Humconejer-493Document1 pageRedes Alcantarillado Pluvial Plancha: 1-Sa-P-Humconejer-493JOSE RODRIGO TORRES CORREANo ratings yet
- Chuva SAXDocument2 pagesChuva SAXFabio FalaguastaNo ratings yet
- Thirteen Previously Unpublished Letters of Ayn RandDocument28 pagesThirteen Previously Unpublished Letters of Ayn RandJOHN MORALES GONZALEZNo ratings yet
- Modul Praktikum Perancangan Tata Letak FasilitasDocument74 pagesModul Praktikum Perancangan Tata Letak FasilitasHafidz Asy'ari AkbarNo ratings yet
- HIRA (INST'L OF 1-Unit PHE & PIPING WORKS)Document1 pageHIRA (INST'L OF 1-Unit PHE & PIPING WORKS)Riemel IdjaoNo ratings yet
- (Aiims Awantipora) Kashmir: All India Institute of Medical SciencesDocument1 page(Aiims Awantipora) Kashmir: All India Institute of Medical SciencesAbilaash VelumaniNo ratings yet
- A380 Family Maintenance ConceptDocument1 pageA380 Family Maintenance Conceptyazan999100% (1)
- 1) Electric Circuits - Basic ConceptsDocument9 pages1) Electric Circuits - Basic ConceptsJOSE AUGUSTO MODESTO HUAYLINOS GUERRERONo ratings yet
- Royal Palm Beach Charter School Conceptual Design - 041917Document3 pagesRoyal Palm Beach Charter School Conceptual Design - 041917Anonymous WXJTn0No ratings yet
- NUVODocument2 pagesNUVOYousif AlkhalilNo ratings yet
- Board - Conceptual SiteDocument1 pageBoard - Conceptual SiteRaizel CustodioNo ratings yet
- A01461101 Ice & Water - Automatic Defrost Side by Side - R134ADocument2 pagesA01461101 Ice & Water - Automatic Defrost Side by Side - R134AJOSE JIMENEZNo ratings yet
- Algoritmo Trauma RenalDocument1 pageAlgoritmo Trauma RenalRobert MacedoNo ratings yet
- Rotodynamic PumpsDocument2 pagesRotodynamic PumpsDavid AguilarNo ratings yet
- MDR Flowchart Dec2017Document1 pageMDR Flowchart Dec2017kicklOp100% (2)
- Loop Diuretics in Heart FailureDocument8 pagesLoop Diuretics in Heart FailureKenWin NguyễnNo ratings yet
- CME NôiDocument106 pagesCME NôiKenWin NguyễnNo ratings yet
- ASHP Foundation Pharmacy Forecast 2018 Strategic PDocument32 pagesASHP Foundation Pharmacy Forecast 2018 Strategic PKenWin NguyễnNo ratings yet
- Digoxin, MortalityDocument12 pagesDigoxin, MortalityKenWin NguyễnNo ratings yet
- T2D Hospital 2022Document10 pagesT2D Hospital 2022KenWin NguyễnNo ratings yet
- Biology 2Document15 pagesBiology 2AlexanderGramtNo ratings yet
- Class 12 Investigatory Project by Heymang AgarwalDocument30 pagesClass 12 Investigatory Project by Heymang AgarwalHEYMANG AGARWALNo ratings yet
- Ex Post Facto ResearchDocument2 pagesEx Post Facto ResearchAnonymous JaUcX95No ratings yet
- GES Classroom Daily Health Monitoring ToolDocument4 pagesGES Classroom Daily Health Monitoring ToolBeverlyRose Bueno Delos SantosNo ratings yet
- Nutrient Management in Recirculating Hydroponic Culture: On What We Want The Plant To Take UpDocument14 pagesNutrient Management in Recirculating Hydroponic Culture: On What We Want The Plant To Take UpAnthony ContrerasNo ratings yet
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- PhysioEx Exercise 5Document21 pagesPhysioEx Exercise 5Sinisa Ristic100% (1)
- Exam 2021Document37 pagesExam 2021Yasser ezzatNo ratings yet
- Literature Review On Immunization in NigeriaDocument13 pagesLiterature Review On Immunization in Nigeriaaflsigfek100% (1)
- Hematology 1 LeukemiaDocument140 pagesHematology 1 LeukemiamaryantoinetteriveraNo ratings yet
- Key+Herbal+Remedies - Key+Concepts+070814 2Document11 pagesKey+Herbal+Remedies - Key+Concepts+070814 2Margot VazquezNo ratings yet
- Which of The Following Conditions Is Associated With Increased Risk of Breast Cancer?Document40 pagesWhich of The Following Conditions Is Associated With Increased Risk of Breast Cancer?Nessreen JamalNo ratings yet
- Insert Hep B Engerix-BDocument16 pagesInsert Hep B Engerix-BshifanahmedNo ratings yet
- Mucormycosis (Zygomycosis) - UpToDateDocument37 pagesMucormycosis (Zygomycosis) - UpToDatem BolañosNo ratings yet
- Ent Midterms SamplexDocument7 pagesEnt Midterms SamplexdeevoncNo ratings yet
- Og NGDocument22 pagesOg NGSandya PallapotuNo ratings yet
- Pharma Mar Smart Fund Short ThesisDocument24 pagesPharma Mar Smart Fund Short Thesisjulia skripka-serry20% (5)
- Volume II - SP82Document415 pagesVolume II - SP82zarcone7No ratings yet
- Lecture Colon 2016Document186 pagesLecture Colon 2016Mr AANo ratings yet
- Potential Application of Milk and Milk Products As Carrier For Herbs and NutraceuticalsDocument18 pagesPotential Application of Milk and Milk Products As Carrier For Herbs and NutraceuticalsSubhan Aristiadi RachmanNo ratings yet
- Importance of Prenatal CareDocument12 pagesImportance of Prenatal CarePinkymekala HasanparthyNo ratings yet
- 24 PublicationDocument44 pages24 PublicationDevi Ratna YuliantiNo ratings yet
- Cerebellar Disorders: EtiologyDocument3 pagesCerebellar Disorders: EtiologyNistara Singh ChawlaNo ratings yet
- SDH Nursing Health HistoryDocument2 pagesSDH Nursing Health HistorybojumsNo ratings yet
- MAY 2022 Mexican Edition, Volume 1, No. 5: ArticlesDocument33 pagesMAY 2022 Mexican Edition, Volume 1, No. 5: ArticlesJhonny MarquezNo ratings yet
- Treatment of Basicervical Femoral Neck Fractures With Proximal Femoral Nail AntirotationDocument11 pagesTreatment of Basicervical Femoral Neck Fractures With Proximal Femoral Nail AntirotationOrto MespNo ratings yet
- Tomasi Et Al 2017Document5 pagesTomasi Et Al 2017Cristiane TomasiNo ratings yet
- Biology EOC Review ALL StandardsDocument83 pagesBiology EOC Review ALL StandardsmspallardNo ratings yet
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) Virusshoaib chNo ratings yet