Download as docx, pdf, or txt
You might also like
- Simplified Group Application FormDocument1 pageSimplified Group Application FormJammie Rize GautaneNo ratings yet
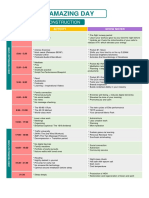
- The Amazing DayDocument1 pageThe Amazing DayLê Công HậuNo ratings yet
- Maxicare Healthcare CorporationDocument3 pagesMaxicare Healthcare CorporationOut-Patient Services MMCNo ratings yet
- Maxicare Application FormDocument3 pagesMaxicare Application Formbzkid82No ratings yet
- Neuroanatomy Through Clinical Cases, 2E PDFDocument3 pagesNeuroanatomy Through Clinical Cases, 2E PDFjwongggg55140% (6)
- MEDICARDDocument1 pageMEDICARDFei TrinidadNo ratings yet
- Application Form Revision 9 July 3 2017Document2 pagesApplication Form Revision 9 July 3 2017OrlanNo ratings yet
- MediCard Standard Plan FormDocument31 pagesMediCard Standard Plan FormCheskaPink TemonesNo ratings yet
- 2024 Medicard IF Application FormDocument2 pages2024 Medicard IF Application FormAlyzza EscalanteNo ratings yet
- AttachmentDocument3 pagesAttachmentfarooq qadirNo ratings yet
- Appl Form OCLDocument2 pagesAppl Form OCLNikki Gaskins CampbellNo ratings yet
- Accident/Hospital Indemnity Wellness Benefit Claim Form: CW 061999 Page 1 of 2 02/14Document2 pagesAccident/Hospital Indemnity Wellness Benefit Claim Form: CW 061999 Page 1 of 2 02/14Stam AnNo ratings yet
- App Form - New 1Document1 pageApp Form - New 1Nexan Delos AngelesNo ratings yet
- Mississippi State Board of Medical Licensure: Complaint FormDocument5 pagesMississippi State Board of Medical Licensure: Complaint FormScott SistersNo ratings yet
- Health Statement FormDocument2 pagesHealth Statement FormRose Ann DuqueNo ratings yet
- (212202114500 PM) SASOLMED - Application - For - Membership - Fillable - NewDocument6 pages(212202114500 PM) SASOLMED - Application - For - Membership - Fillable - NewLenox D LengauNo ratings yet
- Medical History ReportDocument4 pagesMedical History ReportRacel AbulaNo ratings yet
- Relationship Beyond Insurance: Health Guard: Proposal FormDocument2 pagesRelationship Beyond Insurance: Health Guard: Proposal FormAmardeep SinghNo ratings yet
- Proposal Form Yuva Bharat Health PolicyDocument7 pagesProposal Form Yuva Bharat Health PolicyVirendra VedNo ratings yet
- PMA Member Registration FormDocument1 pagePMA Member Registration FormRose PeranteNo ratings yet
- Patient Consent Form (Hiv) : Treating Doctor'S DetailsDocument1 pagePatient Consent Form (Hiv) : Treating Doctor'S DetailsValentino KhojaNo ratings yet
- My Maxicare Application Form 2023Document3 pagesMy Maxicare Application Form 2023Engilbert MaqueraNo ratings yet
- Harris Health Trainees Registration Packet (10!8!19)Document8 pagesHarris Health Trainees Registration Packet (10!8!19)Carolyn FanNo ratings yet
- Attending Physician's Statement-Hospital Income BenefitDocument1 pageAttending Physician's Statement-Hospital Income BenefitVennus RacraquinNo ratings yet
- DMC Patient FormsDocument6 pagesDMC Patient FormsScott cosentinoNo ratings yet
- PMA Member Registration FormDocument1 pagePMA Member Registration FormMary patrize GonzalesNo ratings yet
- My Maxicare Application Form 2023Document2 pagesMy Maxicare Application Form 2023Engilbert Maquera0% (1)
- Application Form For MJDocument2 pagesApplication Form For MJMJNo ratings yet
- Group Five: Safety, Health, Environmental & Quality Personal Information For Emergency PurposesDocument1 pageGroup Five: Safety, Health, Environmental & Quality Personal Information For Emergency PurposesgrantNo ratings yet
- Application - Regency For Expats Essential FullDocument2 pagesApplication - Regency For Expats Essential FullLucas GomezNo ratings yet
- Anthem Medical Claim FormDocument2 pagesAnthem Medical Claim FormsaiprojectworkNo ratings yet
- Sample Marion County Non-Fillable Financial Decl FormDocument5 pagesSample Marion County Non-Fillable Financial Decl FormTrezanay Michelle AtkinsNo ratings yet
- Authorization Form For Doctor'S Consultation Only: 03/21/2023 Dr. James Bermas 03/28/2023Document1 pageAuthorization Form For Doctor'S Consultation Only: 03/21/2023 Dr. James Bermas 03/28/2023Vincent GarciaNo ratings yet
- Claim For Dental Care Expenses: Dentist InformationDocument2 pagesClaim For Dental Care Expenses: Dentist InformationAbdelbassit Abdessamed SenhadjiNo ratings yet
- MS Birth Cert. AppDocument2 pagesMS Birth Cert. AppJonathanKiehlNo ratings yet
- AppForm Select 2018 3-23Document6 pagesAppForm Select 2018 3-23BWP DeveloperNo ratings yet
- Latihan 8 (Tabel Lanjutan)Document2 pagesLatihan 8 (Tabel Lanjutan)Andi KurniantoNo ratings yet
- ESAP FormsDocument17 pagesESAP FormsKa PuringNo ratings yet
- Claimant'S Statement - Death ClaimDocument2 pagesClaimant'S Statement - Death ClaimChristian DazaNo ratings yet
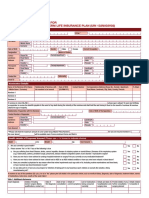
- Voluntary Group Life Insurance Application Form FinalDocument1 pageVoluntary Group Life Insurance Application Form FinalNoli Azanza IIINo ratings yet
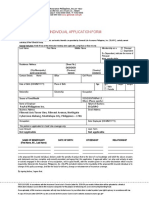
- Application For Individual Insurance FormDocument2 pagesApplication For Individual Insurance FormShenna RojasNo ratings yet
- ENDOCRINODocument14 pagesENDOCRINOreogomezNo ratings yet
- Medical Benefits For Qualified Dependents Enrolment/Cancelation FormDocument1 pageMedical Benefits For Qualified Dependents Enrolment/Cancelation FormAnne MartinezNo ratings yet
- GMI Brochure PDFDocument2 pagesGMI Brochure PDFSulakhe ShounakNo ratings yet
- Claim FormDocument1 pageClaim FormShyam SundarNo ratings yet
- Gsis-Sti Educational Assistance Application Form: For GSIS Members, Pensioners or Qualified DependentDocument2 pagesGsis-Sti Educational Assistance Application Form: For GSIS Members, Pensioners or Qualified DependentArmilyn Macasero LubuguinNo ratings yet
- Select/Premier Medical Plan: Application FormDocument6 pagesSelect/Premier Medical Plan: Application Formadobo sinigangNo ratings yet
- ETIQADocument1 pageETIQAジョン ジーNo ratings yet
- Life Insurance Beneficiary Designation Form - GeneraliDocument2 pagesLife Insurance Beneficiary Designation Form - Generalijohn gerald reynoNo ratings yet
- Reforms in Marriage Related LawsDocument109 pagesReforms in Marriage Related LawsPradeep Kumar Kunche100% (1)
- StateApplication SD Vital Record's RequestDocument2 pagesStateApplication SD Vital Record's RequestAlex OwensNo ratings yet
- The Oriental Insurance Company Limited: A. POLICY TERM: (Please Tick The Relevant Box)Document6 pagesThe Oriental Insurance Company Limited: A. POLICY TERM: (Please Tick The Relevant Box)Gana SNo ratings yet
- MSWD Form IIDocument3 pagesMSWD Form IIDanicaNo ratings yet
- Personal Data Sheet: Print NameDocument3 pagesPersonal Data Sheet: Print NameedithaNo ratings yet
- Intrams Form UpdatedDocument9 pagesIntrams Form Updatedjoy anticosaNo ratings yet
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- Food Gis 2024Document4 pagesFood Gis 2024Princess juhanisah BanocagNo ratings yet
- Member Enrolment Form-GTL-without Addendum-19 Nov 2018Document2 pagesMember Enrolment Form-GTL-without Addendum-19 Nov 2018Rajesh MukkavilliNo ratings yet
- Authorization To Release Medical CertificateDocument1 pageAuthorization To Release Medical CertificatePsychology TodayNo ratings yet
- Sunlife Grepa Application FormDocument2 pagesSunlife Grepa Application Formkathreentracy0% (1)
- Report Ko.Document6 pagesReport Ko.Rhodora AnsayNo ratings yet
- Survey QuestionnaireDocument3 pagesSurvey QuestionnaireRhodora AnsayNo ratings yet
- Fitt 1 SyllabusDocument13 pagesFitt 1 SyllabusRhodora AnsayNo ratings yet
- Needs of LibraryDocument2 pagesNeeds of LibraryRhodora AnsayNo ratings yet
- PathfitDocument1 pagePathfitRhodora AnsayNo ratings yet
- Related StudiesDocument2 pagesRelated StudiesRhodora AnsayNo ratings yet
- LACUAA - Program WordDocument2 pagesLACUAA - Program WordRhodora AnsayNo ratings yet
- Client Satisfactory Survey Result As of June 2022Document3 pagesClient Satisfactory Survey Result As of June 2022Rhodora AnsayNo ratings yet
- 30 Mins.Document3 pages30 Mins.Jude NapireNo ratings yet
- Teaching StrategiesDocument2 pagesTeaching Strategiesnicole bejasaNo ratings yet
- BT Hoan Thanh CauDocument4 pagesBT Hoan Thanh CauNhi HoàngNo ratings yet
- Unit Plan Healthy Relationships 3Document60 pagesUnit Plan Healthy Relationships 3api-269745950No ratings yet
- Compensation Analysis of Manufacturing IndustriesDocument14 pagesCompensation Analysis of Manufacturing IndustriesSankar Rajan100% (13)
- Philosophy StatementDocument1 pagePhilosophy Statementapi-583007789No ratings yet
- Ipcn Edukasi JurnalDocument16 pagesIpcn Edukasi JurnalJono ParmiNo ratings yet
- Operating Manual: Single and Combination Lights Chromophare E 778, E 668, E 558Document166 pagesOperating Manual: Single and Combination Lights Chromophare E 778, E 668, E 558hluevanoNo ratings yet
- Accuracy in Football: Scoring A Goal As The Ultimate Objective of Football GameDocument5 pagesAccuracy in Football: Scoring A Goal As The Ultimate Objective of Football Gamepat patNo ratings yet
- PhilCare-FAQ Coverage PDFDocument1 pagePhilCare-FAQ Coverage PDFNoel EboniaNo ratings yet
- SSG Prental ConsentDocument2 pagesSSG Prental ConsentRamil MorenoNo ratings yet
- Health: Concept of Health & WellnessDocument5 pagesHealth: Concept of Health & WellnessEm VibarNo ratings yet
- Ron Kosloff ArticlesDocument75 pagesRon Kosloff ArticlesJoe Jong100% (1)
- Biocheck C2P - PSK Pharma PDFDocument9 pagesBiocheck C2P - PSK Pharma PDFFari ShaikhNo ratings yet
- Game - The Compleat Strategyst (Theory of Games of Strategy) (PDFDrive)Document285 pagesGame - The Compleat Strategyst (Theory of Games of Strategy) (PDFDrive)namsNo ratings yet
- Golden RiceDocument6 pagesGolden RiceJoshua AgravioNo ratings yet
- Principles of Aseptic TechniqueDocument5 pagesPrinciples of Aseptic TechniqueNicole Audrey JoaquinNo ratings yet
- 31Document15 pages31Amit TamboliNo ratings yet
- Creatina FosfoquinasaDocument1 pageCreatina Fosfoquinasasusey tepaNo ratings yet
- Acitivity 4Document2 pagesAcitivity 4Elijah Mae MundocNo ratings yet
- Important News About Your Health Benefits: Francisco Gianan 1842 Plaza Del Amo Apt 2 TORRANCE, CA 90501Document13 pagesImportant News About Your Health Benefits: Francisco Gianan 1842 Plaza Del Amo Apt 2 TORRANCE, CA 90501Nina GiananNo ratings yet
- Concept MapDocument4 pagesConcept MapCasison Mark ArrysonNo ratings yet
- How To Survive Christmas After LossDocument14 pagesHow To Survive Christmas After LossVenetta CoetzeeNo ratings yet
- ERA2010 Journal Title ListDocument1,020 pagesERA2010 Journal Title ListChristopher BoyleNo ratings yet
- Annotated Bibliography MindfulnessDocument14 pagesAnnotated Bibliography Mindfulnessapi-255289819No ratings yet
- OddDocument9 pagesOddapi-644464737No ratings yet
- Skills Training Workshop For MD Surgery TraineesDocument2 pagesSkills Training Workshop For MD Surgery TraineesNibras Sauqath AliNo ratings yet
- Citizen S CharterDocument211 pagesCitizen S CharterHope Hope100% (1)