
Hypertension Gigi
Hypertension Gigi
You might also like
- Research ProposalDocument5 pagesResearch ProposalAishwarya Bharath100% (2)
- NCP (Rheumatic Heart Disease)Document2 pagesNCP (Rheumatic Heart Disease)Jenny Ajoc75% (4)
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersDocument8 pagesJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonNo ratings yet
- Nursing Care Plan For HypertensionDocument5 pagesNursing Care Plan For HypertensionJessy MalloNo ratings yet
- Assessment Nursing Diagnosis Expected Outcome Interventions Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Expected Outcome Interventions Rationale EvaluationQueenzee AsuncionNo ratings yet
- NCP Risk For Decreased CO 1 PDFDocument2 pagesNCP Risk For Decreased CO 1 PDFdubsNo ratings yet
- NCPDocument4 pagesNCPNurhaifa MocademaNo ratings yet
- Risk For Decreased Cardiac Output NCPDocument2 pagesRisk For Decreased Cardiac Output NCPMae Denn LabordoNo ratings yet
- Nanda NCP BasedDocument14 pagesNanda NCP Baseddeliejoyce100% (1)
- Risk For Decreased Cardiac Output: Nursing DiagnosisDocument4 pagesRisk For Decreased Cardiac Output: Nursing DiagnosisRiska RamadaniNo ratings yet
- Soal Kasus HipertensiDocument3 pagesSoal Kasus HipertensiAlya NamiraNo ratings yet
- NCP-DP NCM112LecDocument4 pagesNCP-DP NCM112LecShane CabucosNo ratings yet
- Anesthetic Management of The Hypertensive Patient: Part I: Continuing Education in Memory of Norman Trieger, DMD, MDDocument8 pagesAnesthetic Management of The Hypertensive Patient: Part I: Continuing Education in Memory of Norman Trieger, DMD, MDFitri Aesthetic centerNo ratings yet
- Chlorthalidone For Hypertension in Advanced CKDDocument13 pagesChlorthalidone For Hypertension in Advanced CKDKhudur AlhamdanNo ratings yet
- Essentials of Ambulatory Blood Pressure Monitoring (ABPM) : November 2017Document7 pagesEssentials of Ambulatory Blood Pressure Monitoring (ABPM) : November 2017Apt RiskaNo ratings yet
- Readiness For Enhanced Health ManagementDocument6 pagesReadiness For Enhanced Health ManagementJIMENEZ, TRISHA MARIE D.No ratings yet
- Materi Koas GinjalDocument30 pagesMateri Koas GinjalRichard 151289No ratings yet
- Acute Pericarditis: Clinical PracticeDocument8 pagesAcute Pericarditis: Clinical PracticeGaby Alejandra Ordonez AndradeNo ratings yet
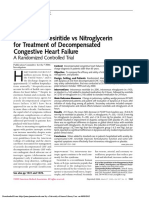
- Intravenous Nesiritide Vs Nitroglycerin For Treatment of Decompensated Congestive Heart Failure - A Randomized Controlled TrialDocument11 pagesIntravenous Nesiritide Vs Nitroglycerin For Treatment of Decompensated Congestive Heart Failure - A Randomized Controlled TrialAnderson Alexander Gonzales RojasNo ratings yet
- Hypertension: S F Vascular SystemDocument12 pagesHypertension: S F Vascular SystemSNo ratings yet
- 6 Alterations On Tissue Perfusion Poleno Serrano TajalaDocument18 pages6 Alterations On Tissue Perfusion Poleno Serrano TajalaSophia A. GoNo ratings yet
- HypertensionDocument2 pagesHypertensionBlessie FernandezNo ratings yet
- Patient's Says (The Worst So Far: Ssessment Diagnosis Planning Interventions RationaleDocument1 pagePatient's Says (The Worst So Far: Ssessment Diagnosis Planning Interventions RationaleDl Al-azizNo ratings yet
- Antihypertensive Drug LongDocument21 pagesAntihypertensive Drug Longa.muhsinNo ratings yet
- Heart Failure With Preserved Ejection Fraction: Clinical PracticeDocument10 pagesHeart Failure With Preserved Ejection Fraction: Clinical PracticeOngky AristianNo ratings yet
- Imed History TakingDocument8 pagesImed History TakingWest AfricaNo ratings yet
- Jolly Hannah Management of Hypertensive Emergencies 2021Document7 pagesJolly Hannah Management of Hypertensive Emergencies 2021Angela Moreira ArteagaNo ratings yet
- Angiotensin-Converting Enzyme (ACE)Document5 pagesAngiotensin-Converting Enzyme (ACE)Isabella SamsonNo ratings yet
- NCP BeeaDocument3 pagesNCP BeeaKiko BernardinoNo ratings yet
- Topic 10 Internal Medicine Ali SaifDocument5 pagesTopic 10 Internal Medicine Ali SaifAnkit Kumar PatelNo ratings yet
- NCP Partial, Micu Medcor DutyDocument7 pagesNCP Partial, Micu Medcor DutyYana PotNo ratings yet
- Clase 7Document10 pagesClase 7felipaocosasNo ratings yet
- Jurnal HTDocument8 pagesJurnal HTseruniallisaaslimNo ratings yet
- Emergency Room Management of Hypertensive Urgencies and EmergenciesDocument7 pagesEmergency Room Management of Hypertensive Urgencies and Emergenciesandrea coelloNo ratings yet
- 6 HypertensionDocument95 pages6 HypertensionZeleke temechewNo ratings yet
- Amlo, Simvastatin, TamsulosinDocument7 pagesAmlo, Simvastatin, TamsulosinGwyn RosalesNo ratings yet
- Nursing Care Plan Format X1Document3 pagesNursing Care Plan Format X1Ramiel ChristopherNo ratings yet
- Drugs For Cardiovascular DiseasesDocument74 pagesDrugs For Cardiovascular Diseasesmjd13mjd4No ratings yet
- Heart Failure With Preserved OriginalDocument10 pagesHeart Failure With Preserved OriginalReinaldo MarchenaNo ratings yet
- R02Y2002N04A0219Document7 pagesR02Y2002N04A0219gustiNo ratings yet
- Nursing Care Plan 1Document4 pagesNursing Care Plan 1Kiko BernardinoNo ratings yet
- Daily ReqDocument29 pagesDaily ReqPsyche YonaNo ratings yet
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac Outputaudreyann.acobNo ratings yet
- 2 Article Presentation (Chlorthalidone)Document26 pages2 Article Presentation (Chlorthalidone)Palak GuptaNo ratings yet
- Drug StudyDocument5 pagesDrug StudySharies ArgelNo ratings yet
- Nurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Document27 pagesNurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Nurulilmi hajarNo ratings yet
- NCP AgnDocument2 pagesNCP Agnj3nann3No ratings yet
- Conns Syndrome Gonzales NickaDocument10 pagesConns Syndrome Gonzales Nickamafeehney feehilyNo ratings yet
- Art Hipertension SecundariaDocument15 pagesArt Hipertension SecundariaLisset FernandezNo ratings yet
- Penatalaksanaan Hipertensi EmergensiDocument6 pagesPenatalaksanaan Hipertensi Emergensiain17001No ratings yet
- Classification of HT Goal of Therapy Lifestyle Modifications Pharmacological Therapy Management HT ConclusionDocument82 pagesClassification of HT Goal of Therapy Lifestyle Modifications Pharmacological Therapy Management HT ConclusionBima Ewando KabanNo ratings yet
- Resistant Hypertension A Review of Diagnosis and Management: Grand RoundsDocument9 pagesResistant Hypertension A Review of Diagnosis and Management: Grand RoundsCarmen Giselt Sanchez AgudeloNo ratings yet
- White Coat HypertensionDocument6 pagesWhite Coat HypertensionOmar MedinaNo ratings yet
- Marcos Er NCPDocument1 pageMarcos Er NCPAssasination ClassroomNo ratings yet
- 001 Chapter 6 Hemodynamic MonitoringDocument18 pages001 Chapter 6 Hemodynamic MonitoringMahesh Boopathy100% (2)
- Patofisiologi Krisis HipertensiDocument4 pagesPatofisiologi Krisis HipertensiAfriodita Ary PratiwiNo ratings yet
- Resistant Hypertension - Cleveland Clinic (2023)Document11 pagesResistant Hypertension - Cleveland Clinic (2023)Areli KamuiNo ratings yet
- Clinical Cases in Heart FailureFrom EverandClinical Cases in Heart FailureRavi V. ShahNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Manuskrip Frengki 2014201061Document13 pagesManuskrip Frengki 2014201061frengki FranzNo ratings yet
- Gero Study GuideDocument42 pagesGero Study GuideAbby Schmidt100% (1)
- MAPEH 9 Second GradingDocument9 pagesMAPEH 9 Second GradingSittie Rahma AlawiNo ratings yet
- Hypertensive Disorders in PregnancyDocument27 pagesHypertensive Disorders in PregnancyHarleyquinn96 DrNo ratings yet
- Normal Laboratory Values - Patient Test Charts: Determination Normal Reference ValueDocument10 pagesNormal Laboratory Values - Patient Test Charts: Determination Normal Reference ValueGita Elisa Berlina GintingNo ratings yet
- 4TH PT G7Document4 pages4TH PT G7Arlan Delos ReyesNo ratings yet
- Form No. 31AhEALTHDocument2 pagesForm No. 31AhEALTHPrasanta PatnaikNo ratings yet
- A Study of Prescribing Pattern of Antihypertensive Drugs in Hypertensive Patients With Co Morbid Diabetes in A Tertiary Care Teaching HospitalDocument6 pagesA Study of Prescribing Pattern of Antihypertensive Drugs in Hypertensive Patients With Co Morbid Diabetes in A Tertiary Care Teaching HospitalSandhya kumarNo ratings yet
- 1 Compression Therapy..Document43 pages1 Compression Therapy..Nermeen7No ratings yet
- Pengaruh Pemberian Smoothies Campuran Pisang Ambon Dan Melon Terhadap Penurunan Tekanan Darah Pada Perempuan Penderita Hipertensi Usia 45-59 TahunDocument9 pagesPengaruh Pemberian Smoothies Campuran Pisang Ambon Dan Melon Terhadap Penurunan Tekanan Darah Pada Perempuan Penderita Hipertensi Usia 45-59 TahunAyu WidyaningsihNo ratings yet
- Sample Family Care Study (N107)Document51 pagesSample Family Care Study (N107)Dan Dan Soi T97% (31)
- CHN 1st and 2nd Level 2nd SemDocument9 pagesCHN 1st and 2nd Level 2nd SemCharlaine Gripal SudlaNo ratings yet
- AACE Abstracts 2019 Los AngelesDocument357 pagesAACE Abstracts 2019 Los Angelesmimran1974No ratings yet
- Karangan Tentang KesehatanDocument2 pagesKarangan Tentang KesehatanMega FadillahNo ratings yet
- Blood Pressure ChartDocument27 pagesBlood Pressure ChartRamakrishna Kurapati100% (1)
- Med MathDocument22 pagesMed Mathmeanne073No ratings yet
- Rokh 2e ST4 PDFDocument141 pagesRokh 2e ST4 PDFMahmud DipuNo ratings yet
- Casos Clínicos InglésDocument15 pagesCasos Clínicos InglésClaudio R. MonteroNo ratings yet
- OET WritingDocument34 pagesOET WritingWarangkana91% (91)
- Cardio SNAP-BNP NT-proBNP IdexxDocument4 pagesCardio SNAP-BNP NT-proBNP IdexxXenia FernandezNo ratings yet
- English Prophetic Medicine HerbalismDocument198 pagesEnglish Prophetic Medicine HerbalismAnonymous wUdPm0M8100% (1)
- What Is Cardiomyopathy?Document11 pagesWhat Is Cardiomyopathy?ImmanuelNo ratings yet
- 11. 201909 抗高血压 antihypertensionDocument72 pages11. 201909 抗高血压 antihypertensionShanon LimNo ratings yet
- Medical Surgical ComprehensiveDocument15 pagesMedical Surgical ComprehensiveMatt Lao DionelaNo ratings yet
- BJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With ADocument9 pagesBJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With AHanifa W PNo ratings yet
- ACOG 2020 SMI-hypertension-bundle-slidesDocument34 pagesACOG 2020 SMI-hypertension-bundle-slidesLuciana Salomé Bravo QuintanillaNo ratings yet
- 1 Hypertensive Disorders in PregnancyDocument54 pages1 Hypertensive Disorders in PregnancyChew JessyNo ratings yet
- Acid UricDocument3 pagesAcid UricCosmin AndreiNo ratings yet
- BM35 Blood Pressure MonitorDocument22 pagesBM35 Blood Pressure MonitorAdrian DumitrescuNo ratings yet























































































Download as docx, pdf, or txt
You might also like
- Research ProposalDocument5 pagesResearch ProposalAishwarya Bharath100% (2)
- NCP (Rheumatic Heart Disease)Document2 pagesNCP (Rheumatic Heart Disease)Jenny Ajoc75% (4)
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersDocument8 pagesJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonNo ratings yet
- Nursing Care Plan For HypertensionDocument5 pagesNursing Care Plan For HypertensionJessy MalloNo ratings yet
- Assessment Nursing Diagnosis Expected Outcome Interventions Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Expected Outcome Interventions Rationale EvaluationQueenzee AsuncionNo ratings yet
- NCP Risk For Decreased CO 1 PDFDocument2 pagesNCP Risk For Decreased CO 1 PDFdubsNo ratings yet
- NCPDocument4 pagesNCPNurhaifa MocademaNo ratings yet
- Risk For Decreased Cardiac Output NCPDocument2 pagesRisk For Decreased Cardiac Output NCPMae Denn LabordoNo ratings yet
- Nanda NCP BasedDocument14 pagesNanda NCP Baseddeliejoyce100% (1)
- Risk For Decreased Cardiac Output: Nursing DiagnosisDocument4 pagesRisk For Decreased Cardiac Output: Nursing DiagnosisRiska RamadaniNo ratings yet
- Soal Kasus HipertensiDocument3 pagesSoal Kasus HipertensiAlya NamiraNo ratings yet
- NCP-DP NCM112LecDocument4 pagesNCP-DP NCM112LecShane CabucosNo ratings yet
- Anesthetic Management of The Hypertensive Patient: Part I: Continuing Education in Memory of Norman Trieger, DMD, MDDocument8 pagesAnesthetic Management of The Hypertensive Patient: Part I: Continuing Education in Memory of Norman Trieger, DMD, MDFitri Aesthetic centerNo ratings yet
- Chlorthalidone For Hypertension in Advanced CKDDocument13 pagesChlorthalidone For Hypertension in Advanced CKDKhudur AlhamdanNo ratings yet
- Essentials of Ambulatory Blood Pressure Monitoring (ABPM) : November 2017Document7 pagesEssentials of Ambulatory Blood Pressure Monitoring (ABPM) : November 2017Apt RiskaNo ratings yet
- Readiness For Enhanced Health ManagementDocument6 pagesReadiness For Enhanced Health ManagementJIMENEZ, TRISHA MARIE D.No ratings yet
- Materi Koas GinjalDocument30 pagesMateri Koas GinjalRichard 151289No ratings yet
- Acute Pericarditis: Clinical PracticeDocument8 pagesAcute Pericarditis: Clinical PracticeGaby Alejandra Ordonez AndradeNo ratings yet
- Intravenous Nesiritide Vs Nitroglycerin For Treatment of Decompensated Congestive Heart Failure - A Randomized Controlled TrialDocument11 pagesIntravenous Nesiritide Vs Nitroglycerin For Treatment of Decompensated Congestive Heart Failure - A Randomized Controlled TrialAnderson Alexander Gonzales RojasNo ratings yet
- Hypertension: S F Vascular SystemDocument12 pagesHypertension: S F Vascular SystemSNo ratings yet
- 6 Alterations On Tissue Perfusion Poleno Serrano TajalaDocument18 pages6 Alterations On Tissue Perfusion Poleno Serrano TajalaSophia A. GoNo ratings yet
- HypertensionDocument2 pagesHypertensionBlessie FernandezNo ratings yet
- Patient's Says (The Worst So Far: Ssessment Diagnosis Planning Interventions RationaleDocument1 pagePatient's Says (The Worst So Far: Ssessment Diagnosis Planning Interventions RationaleDl Al-azizNo ratings yet
- Antihypertensive Drug LongDocument21 pagesAntihypertensive Drug Longa.muhsinNo ratings yet
- Heart Failure With Preserved Ejection Fraction: Clinical PracticeDocument10 pagesHeart Failure With Preserved Ejection Fraction: Clinical PracticeOngky AristianNo ratings yet
- Imed History TakingDocument8 pagesImed History TakingWest AfricaNo ratings yet
- Jolly Hannah Management of Hypertensive Emergencies 2021Document7 pagesJolly Hannah Management of Hypertensive Emergencies 2021Angela Moreira ArteagaNo ratings yet
- Angiotensin-Converting Enzyme (ACE)Document5 pagesAngiotensin-Converting Enzyme (ACE)Isabella SamsonNo ratings yet
- NCP BeeaDocument3 pagesNCP BeeaKiko BernardinoNo ratings yet
- Topic 10 Internal Medicine Ali SaifDocument5 pagesTopic 10 Internal Medicine Ali SaifAnkit Kumar PatelNo ratings yet
- NCP Partial, Micu Medcor DutyDocument7 pagesNCP Partial, Micu Medcor DutyYana PotNo ratings yet
- Clase 7Document10 pagesClase 7felipaocosasNo ratings yet
- Jurnal HTDocument8 pagesJurnal HTseruniallisaaslimNo ratings yet
- Emergency Room Management of Hypertensive Urgencies and EmergenciesDocument7 pagesEmergency Room Management of Hypertensive Urgencies and Emergenciesandrea coelloNo ratings yet
- 6 HypertensionDocument95 pages6 HypertensionZeleke temechewNo ratings yet
- Amlo, Simvastatin, TamsulosinDocument7 pagesAmlo, Simvastatin, TamsulosinGwyn RosalesNo ratings yet
- Nursing Care Plan Format X1Document3 pagesNursing Care Plan Format X1Ramiel ChristopherNo ratings yet
- Drugs For Cardiovascular DiseasesDocument74 pagesDrugs For Cardiovascular Diseasesmjd13mjd4No ratings yet
- Heart Failure With Preserved OriginalDocument10 pagesHeart Failure With Preserved OriginalReinaldo MarchenaNo ratings yet
- R02Y2002N04A0219Document7 pagesR02Y2002N04A0219gustiNo ratings yet
- Nursing Care Plan 1Document4 pagesNursing Care Plan 1Kiko BernardinoNo ratings yet
- Daily ReqDocument29 pagesDaily ReqPsyche YonaNo ratings yet
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac Outputaudreyann.acobNo ratings yet
- 2 Article Presentation (Chlorthalidone)Document26 pages2 Article Presentation (Chlorthalidone)Palak GuptaNo ratings yet
- Drug StudyDocument5 pagesDrug StudySharies ArgelNo ratings yet
- Nurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Document27 pagesNurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Nurulilmi hajarNo ratings yet
- NCP AgnDocument2 pagesNCP Agnj3nann3No ratings yet
- Conns Syndrome Gonzales NickaDocument10 pagesConns Syndrome Gonzales Nickamafeehney feehilyNo ratings yet
- Art Hipertension SecundariaDocument15 pagesArt Hipertension SecundariaLisset FernandezNo ratings yet
- Penatalaksanaan Hipertensi EmergensiDocument6 pagesPenatalaksanaan Hipertensi Emergensiain17001No ratings yet
- Classification of HT Goal of Therapy Lifestyle Modifications Pharmacological Therapy Management HT ConclusionDocument82 pagesClassification of HT Goal of Therapy Lifestyle Modifications Pharmacological Therapy Management HT ConclusionBima Ewando KabanNo ratings yet
- Resistant Hypertension A Review of Diagnosis and Management: Grand RoundsDocument9 pagesResistant Hypertension A Review of Diagnosis and Management: Grand RoundsCarmen Giselt Sanchez AgudeloNo ratings yet
- White Coat HypertensionDocument6 pagesWhite Coat HypertensionOmar MedinaNo ratings yet
- Marcos Er NCPDocument1 pageMarcos Er NCPAssasination ClassroomNo ratings yet
- 001 Chapter 6 Hemodynamic MonitoringDocument18 pages001 Chapter 6 Hemodynamic MonitoringMahesh Boopathy100% (2)
- Patofisiologi Krisis HipertensiDocument4 pagesPatofisiologi Krisis HipertensiAfriodita Ary PratiwiNo ratings yet
- Resistant Hypertension - Cleveland Clinic (2023)Document11 pagesResistant Hypertension - Cleveland Clinic (2023)Areli KamuiNo ratings yet
- Clinical Cases in Heart FailureFrom EverandClinical Cases in Heart FailureRavi V. ShahNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Manuskrip Frengki 2014201061Document13 pagesManuskrip Frengki 2014201061frengki FranzNo ratings yet
- Gero Study GuideDocument42 pagesGero Study GuideAbby Schmidt100% (1)
- MAPEH 9 Second GradingDocument9 pagesMAPEH 9 Second GradingSittie Rahma AlawiNo ratings yet
- Hypertensive Disorders in PregnancyDocument27 pagesHypertensive Disorders in PregnancyHarleyquinn96 DrNo ratings yet
- Normal Laboratory Values - Patient Test Charts: Determination Normal Reference ValueDocument10 pagesNormal Laboratory Values - Patient Test Charts: Determination Normal Reference ValueGita Elisa Berlina GintingNo ratings yet
- 4TH PT G7Document4 pages4TH PT G7Arlan Delos ReyesNo ratings yet
- Form No. 31AhEALTHDocument2 pagesForm No. 31AhEALTHPrasanta PatnaikNo ratings yet
- A Study of Prescribing Pattern of Antihypertensive Drugs in Hypertensive Patients With Co Morbid Diabetes in A Tertiary Care Teaching HospitalDocument6 pagesA Study of Prescribing Pattern of Antihypertensive Drugs in Hypertensive Patients With Co Morbid Diabetes in A Tertiary Care Teaching HospitalSandhya kumarNo ratings yet
- 1 Compression Therapy..Document43 pages1 Compression Therapy..Nermeen7No ratings yet
- Pengaruh Pemberian Smoothies Campuran Pisang Ambon Dan Melon Terhadap Penurunan Tekanan Darah Pada Perempuan Penderita Hipertensi Usia 45-59 TahunDocument9 pagesPengaruh Pemberian Smoothies Campuran Pisang Ambon Dan Melon Terhadap Penurunan Tekanan Darah Pada Perempuan Penderita Hipertensi Usia 45-59 TahunAyu WidyaningsihNo ratings yet
- Sample Family Care Study (N107)Document51 pagesSample Family Care Study (N107)Dan Dan Soi T97% (31)
- CHN 1st and 2nd Level 2nd SemDocument9 pagesCHN 1st and 2nd Level 2nd SemCharlaine Gripal SudlaNo ratings yet
- AACE Abstracts 2019 Los AngelesDocument357 pagesAACE Abstracts 2019 Los Angelesmimran1974No ratings yet
- Karangan Tentang KesehatanDocument2 pagesKarangan Tentang KesehatanMega FadillahNo ratings yet
- Blood Pressure ChartDocument27 pagesBlood Pressure ChartRamakrishna Kurapati100% (1)
- Med MathDocument22 pagesMed Mathmeanne073No ratings yet
- Rokh 2e ST4 PDFDocument141 pagesRokh 2e ST4 PDFMahmud DipuNo ratings yet
- Casos Clínicos InglésDocument15 pagesCasos Clínicos InglésClaudio R. MonteroNo ratings yet
- OET WritingDocument34 pagesOET WritingWarangkana91% (91)
- Cardio SNAP-BNP NT-proBNP IdexxDocument4 pagesCardio SNAP-BNP NT-proBNP IdexxXenia FernandezNo ratings yet
- English Prophetic Medicine HerbalismDocument198 pagesEnglish Prophetic Medicine HerbalismAnonymous wUdPm0M8100% (1)
- What Is Cardiomyopathy?Document11 pagesWhat Is Cardiomyopathy?ImmanuelNo ratings yet
- 11. 201909 抗高血压 antihypertensionDocument72 pages11. 201909 抗高血压 antihypertensionShanon LimNo ratings yet
- Medical Surgical ComprehensiveDocument15 pagesMedical Surgical ComprehensiveMatt Lao DionelaNo ratings yet
- BJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With ADocument9 pagesBJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With AHanifa W PNo ratings yet
- ACOG 2020 SMI-hypertension-bundle-slidesDocument34 pagesACOG 2020 SMI-hypertension-bundle-slidesLuciana Salomé Bravo QuintanillaNo ratings yet
- 1 Hypertensive Disorders in PregnancyDocument54 pages1 Hypertensive Disorders in PregnancyChew JessyNo ratings yet
- Acid UricDocument3 pagesAcid UricCosmin AndreiNo ratings yet
- BM35 Blood Pressure MonitorDocument22 pagesBM35 Blood Pressure MonitorAdrian DumitrescuNo ratings yet